
Abstract
Studies in normal volunteers have demonstrated that the lateral atlanto-axial joints (C1-2) are capable of causing pain in the occiput, but few clinical studies have validated this source of occipital headache. The present study tested the null hypothesis that the lateral atlanto-axial joints are not a common source of occipital headache. Patients presenting with occipital pain underwent diagnostic blocks of their lateral atlanto-axial joints if they demonstrated clinical features presumptively suggestive of a C1-2 origin for their pain. Of 34 patients investigated, 21 obtained complete relief of their headache following diagnostic blocks, indicating that a C1-2 source of occipital pain is not rare. The clinical features used to select patients for blocks, however, had a positive predictive value of only 60%. Further study of headaches from C1-2 seems justified in order to establish more definitively the prevalence of this condition and how it might become better recognized in practice.
Introduction
Since it was first conceived, the notion of cervicogenic headache has been controversial. The original diagnostic criteria were entirely clinical (1, 2), but some investigators found that these criteria did not allow physicians to distinguish cervicogenic headache from migraine or tension-type headache (3, 4). Others, however, were more able (5). Nevertheless, according to the most recent study, when restricted to history and clinical examination, headache experts and pain specialists are still apt to disagree as to whether a patient has cervicogenic headache, migraine or tension-type headache (6). Agreement amounts to only 76%, with the hardest distinction being between cervicogenic headache and tension-type headache.
Revised criteria (7, 8) require that any clinical diagnosis should be corroborated by the results of diagnostic blocks. Blockade of a cervical structure or a cervical nerve should abolish the patient's pain. Listed as possible sources of cervicogenic headache are the nerves, nerve roots, ganglia, uncovertebral joints, intervertebral disks, facet joints, periosteum, muscles and ligaments of the neck or back of the head (8). However, few of these sources of pain have been subjected to diagnostic blocks. Formal studies have concentrated on the greater occipital nerve or the C2–3 zygapophysial joint (9), and occasional reports have described relief of headache following anaesthetization of occipital muscles (10).
Amongst the possible sources of occipital pain and referred pain to the forehead are the upper cervical synovial joints. Studies in normal volunteers have demonstrated that distending the atlanto-occipital (11), the lateral atlanto-axial (11) or the C2–3 zygapophysial (12) joints with contrast medium in normal volunteers evokes pain in the occiput or suboccipital region. Of these joints, the C2–3 zygapophysial joints have been the most extensively studied clinically and reported in the literature (13–15). The lateral atlanto-axial joints have been promoted in conference papers (16) and in descriptive studies of diagnostic techniques (11, 17), but no substantive studies have been published.
Although the lateral atlanto-axial joints can be demonstrated on plain radiographs, medical imaging does not provide a means of determining whether or not the joints are painful. The presence of arthropathy does not guarantee that the joint is painful for, elsewhere in the neck, osteoarthrosis is more often than not painless (18). Nor does a normal image necessarily preclude the joint from being painful. The only means of determining if a joint is painful is to abolish the patient's pain by anaesthetizing the joint.
Some investigators have anaesthetized the lateral atlanto-axial joints using periarticular blocks (19). Such blocks, however, are not target specific, because local anaesthetic agents delivered to the back of the joint capsule may affect the C2 spinal nerve which crosses the posterior aspect of the joint (20). On the other hand, intra-articular blocks will selectively anaesthetize the joint, provided that the injectate does not escape from within the joint capsule.
Intra-articular blocks constitute an objective means of determining if a patient's occipital pain arises from a lateral atlanto-axial joint. These blocks, however, are far from conventional in nature and are not universally available. Specialists in headache are therefore unlikely to have been accustomed to using them in the investigation of occipital headache. On the other hand, lateral atlanto-axial joint blocks are part of the standard armamentarium of some pain specialists and radiologists who concentrate on the investigation and management of spinal pain.
The present study capitalized on the resources of a spinal diagnostic centre experienced in the conduct of lateral atlanto-axial and similar diagnostic blocks (21–25). The study explored the conjecture that occipital headaches could stem from the lateral atlanto-axial joints, by subjecting patients with such headaches to diagnostic blocks of these joints. Furthermore, the study assessed the predictive value of certain, presumptive clinical criteria by which this source of headache might be recognized clinically.
Methods
The practice in which the present study was conducted specializes in diagnostic procedures such as discography and joint blocks for the investigation of spinal pain, particularly back pain and neck pain (21–31). Patients are seen on referral from specialists in physical medicine and rehabilitation, orthopaedics and neurosurgery. In the period from January 1997 to December 1999, 1435 patients with back pain and 772 patients with neck pain were seen. Of the patients with neck pain, 120 also had headache as a dominant or major complaint. These latter patients constituted the source population for the present study.
Since the prevalence of pain from lateral atlanto-axial joints was not known at the time of the study, lateral atlanto-axial joint blocks could not be justified as a routine procedure in every patient with neck pain or with headache. If the condition was rare, too many patients would undergo blocks to no avail, if blocks were routinely performed in every patient. Consequently, certain presumptive clinical criteria were adopted that, on theoretical grounds, would be more likely to be associated with pain from the lateral atlanto-axial joints. These criteria were pain in the occipital or suboccipital region, together with maximal or focal tenderness in the suboccipital region, maximal or focal tenderness over the tip of the left or right transverse process of C1, restricted rotation of C1 on C2 on manual examination of that segment, and aggravation of their accustomed headache by passive rotation of the C1 vertebra to the left or right. For purposes of definition, ‘focal’ tenderness means that the patient was tender to palpation only at the point in question; ‘maximal’ tenderness means that although tender elsewhere the patient complained of greater pain when the site in question was palpated with the same finger pressure as applied to other tender regions; ‘restricted rotation’ means that the segment exhibited less than 50% of the normal range of passive motion expected by the examiner.
If patients exhibited at least four of these clinical features they were eligible for blocks of the lateral atlanto-axial joints. Prior to undergoing blocks, the patients completed a pain drawing that illustrated the location, extent and quality of their headache, and completed a visual analogue scale that rated their present pain.
Blocks were performed using a posterior approach (24, 26). For the procedure, the patient lies prone on a fluoroscopy table, with their forehead supported by a pillow, and their mouth clear of the table, not only to allow freedom to breath but also to allow the mouth to be opened, if required. In order to optimize the view of the lateral atlanto-axial joints, the orientation of the head is adjusted into slight flexion or extension to remove overlying shadows of teeth. In particular, because it can obstruct the passage of a needle into the target joint, the posterior arch of the atlas must be identified, and its position adjusted so that it does not overlie the target joint.
The skin over the suboccipital region is prepared as for an aseptic procedure and an insertion point is selected directly behind the lateral third of the target joint. Under fluoroscopic control, a 90-mm 25-gauge spinal needle is inserted through the skin and upper neck muscles, aiming for the posterior aspect of the lateral third of the inferior margin of the inferior articular process of the atlas (Fig. 1a). Aiming for this point secures subsequent access to the joint but avoids contact with the C2 spinal nerve and ganglion which cross the radiological midpoint of the joint (20). It is critical to contact bone at the target point in order to establish depth of insertion safely. In inexperienced hands, aiming directly for the joint may result in over-penetration, with the needle passing freely through the joint and into the anterior cervical region. Once the inferior articular process of the atlas is reached, a lateral view should confirm that the needle lies on the back of the lateral mass of the atlas (Fig. 1b). Note is taken of the depth of insertion, and the needle is withdrawn slightly and adjusted to point towards the lateral third of the joint cavity (Fig. 2a). Slowly it is reinserted, under fluoroscopic control, either until it is felt to penetrate the joint capsule, or until it has been inserted no more than a few millimetres deeper than it was when it contacted the atlas. At this stage, a lateral view should confirm passage of the needle anterior to the posterior margin of the joint (Fig. 2b).
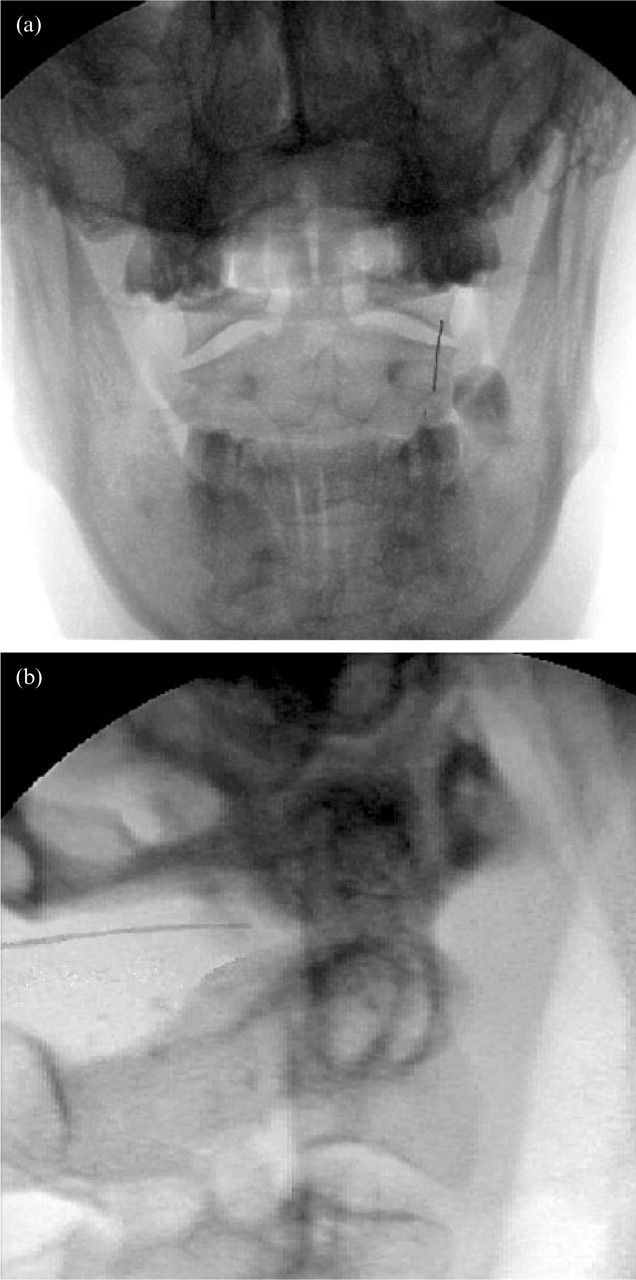
Needle resting on the back of the inferior articular process of the atlas prior to adjustment into the right lateral atlanto-axial joint. a: Postero-anterior view. b: Lateral view.
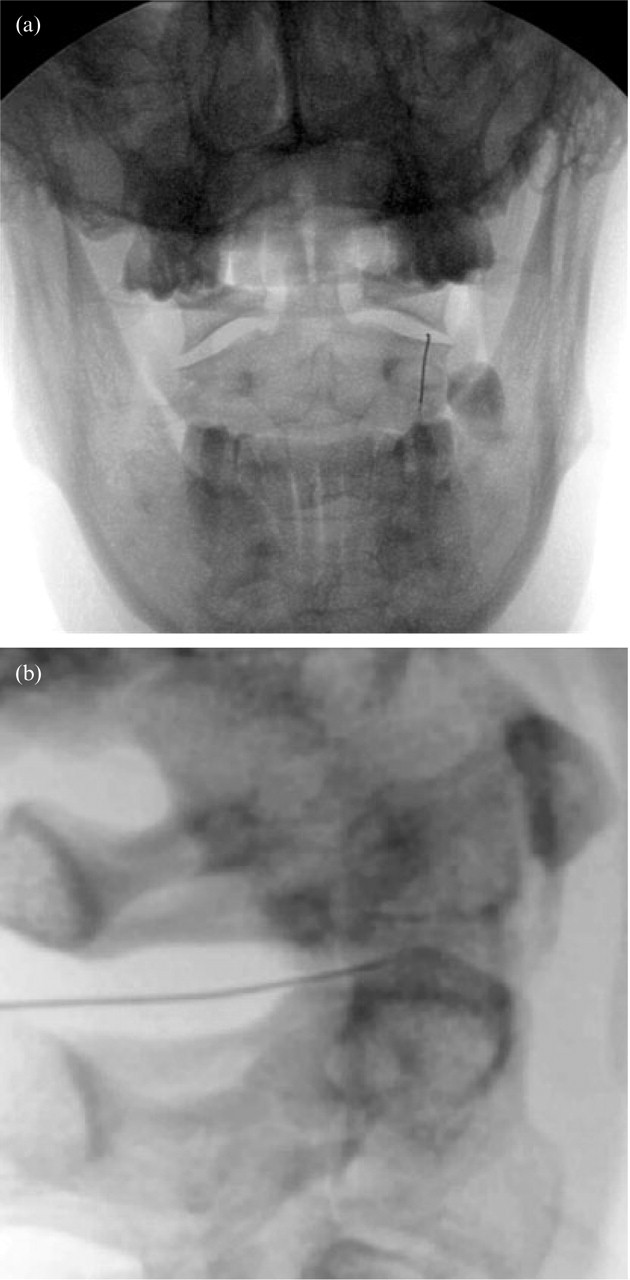
Needle placed within the lateral atlanto-axial joint prior to the injection of contrast medium. a: Postero-anterior view. b: Lateral view.
In order to verify intra-articular placement, and in order to establish that the capsule of the joint is competent and that any injectate will not escape from the joint, an arthrogram is obtained using a small quantity (0.3–0.5 ml) of contrast medium. Antero-posterior and lateral views should confirm that the contrast medium remains within the joint (Fig. 3). The joint space may communicate with that of the median atlanto-axial joint and even with that of the contralateral atlanto-axial joint. This is normal and does not compromise the specificity of the block, provided that any injectate remains within the target joint and does not substantially spread to a communicating joint. What is critical is that the contrast medium does not escape from the target joint into the epidural space, or posteriorly or laterally.
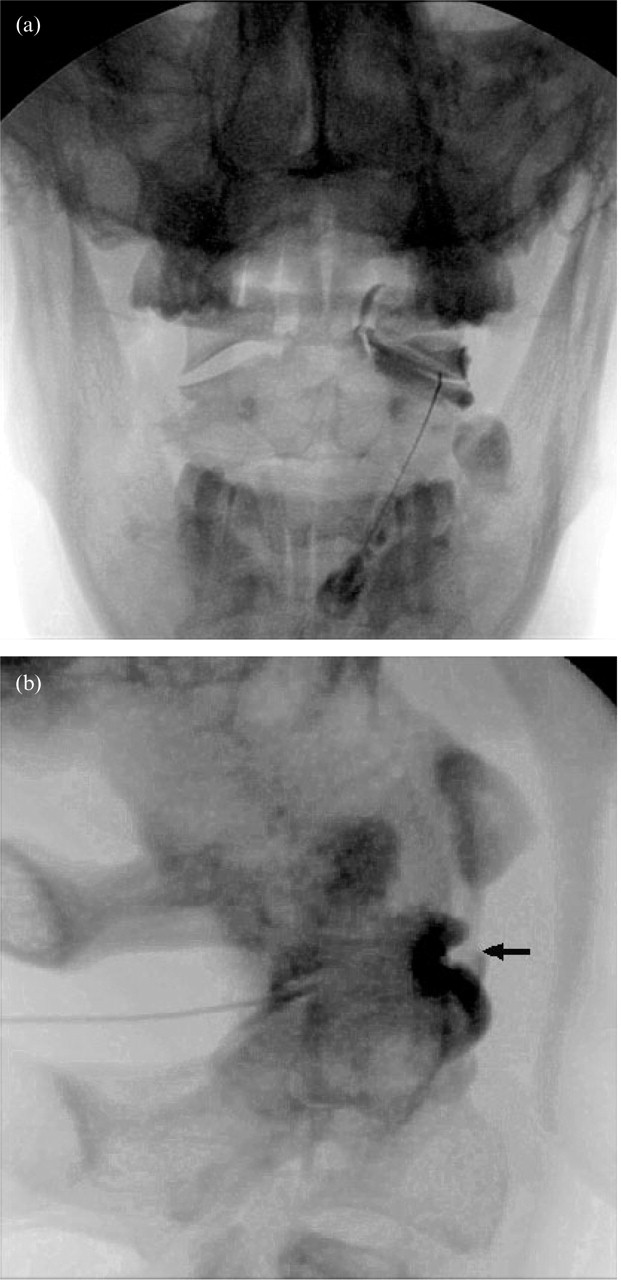
Arthrogram of a lateral atlanto-axial joint obtained with 0.75 ml of contrast medium. a: Postero-anterior view. A trace of contrast medium extends beside the odontoid process towards the median atlanto-axial joint. b: Lateral view. Note the silhouette of a meniscoid (arrow) projecting into the joint from its anterior capsule.
Resistance to injection may be encountered if the tip of the needle lies within the posterior intra-articular meniscoid of the joint (33), or blood may be drawn from this structure upon aspiration prior to injection. In either event, the needle can be inserted, under lateral fluoroscopic guidance, more deeply into the joint, until its tip lies at the midpoint of the joint and therefore beyond the central edge of the meniscoid. If resistance to injection occurs in that position it could be due to insertion of the needle into the articular cartilage, in which event the needle needs only to be withdrawn by one or to millimeters in order to disengage the cartilage.
Once intra-articular placement has been achieved and verified, local anaesthetic can be injected in order to anaesthetize the joint. In the present study 1.0 ml of a mixture of 1 ml 0.5% bupivacaine and 1 ml (6.25 mg) of betamethasone was used. Although there are no data that show that corticosteroids are effective for synovial joint pain in the neck, betamethasone was administered in the present study on the grounds that it did not compromise the effectiveness of the diagnostic block, yet afforded the patient the possible benefit of a presumptive therapy without the need to return for a therapeutic injection.
In patients with unilateral pain, or in whom the headache was substantially worse on one side, the ipsilateral lateral atlanto-axial joint was anaesthetized. In patients with bilateral pain, both joints were anaesthetized. Responses to blocks were recorded by the patient and by a nurse independent of the radiologist who performed the procedure.
The records of all patients who underwent lateral atlanto-axial joint blocks during the period of study were reviewed by the third investigator (NB). A positive response to the block was considered to have occurred if the patient had reported that their headache was relieved for at least the expected duration of action of the local anaesthetic used (at least 2 hours for bupivacaine) and if their pain drawing after the block indicated elimination of pain in the previously affected regions of the head or suboccipital regions, and their visual analogue pain score dropped to zero or less than 1 on a 10-point scale. A score of 1 was accepted if the patient ascribed that residual pain to soreness of the needle track rather than to their previous pain. Furthermore, the patient needed to demonstrate that previously painful movements were no longer painful. Any response that did not satisfy all of these criteria was considered negative or indeterminate.
Patients underwent only single, uncontrolled blocks. Controlled blocks were not undertaken for a variety of reasons. Controlled blocks would have required additional, sham procedures that would have required informed consent and ethics approval, as well as funding approval from insurance carriers for the additional procedures. However, such additional and sham procedures could not be justified when, in the first instance, it was not known if any patients would respond to blocks. Accordingly, the present study was undertaken as an exploratory, observational study to determine if there was any prima facie evidence that the lateral atlanto-axial joint could indeed be a source of occipital pain.
Results
During the period of study, 34 patients underwent lateral atlanto-axial joint blocks. Their demographic and clinical features are recorded in Table 1, along with their responses to blocks. Of the 34 patients, 21 obtained complete relief of their headache, at least for the duration of action of the local anaesthetic used. Their presenting patterns of pain are depicted in Fig. 4. Each patient was relieved of the entire distribution of their pain by the block that they underwent. The remaining 13 patients (Fig. 5) did not obtain relief.
Demographic and clinical features of patients undergoing lateral atlanto-axial joint blocks, according to their response to blocks. MVA: motor vehicle accident


The distribution of pain in 21 patients whose pain was completely relieved by anaesthetization of one or both lateral atlanto-axial joints. All patients illustrated obtained complete relief of pain in the areas shown after anaesthetization of the joints.

The distribution of pain in 13 patients whose pain was not relieved by anaesthetizing one or both lateral atlanto-axial joints.
With respect to demographic features, those patients who responded did not differ from those who did not (Table 1). Nor was there any difference in clinical features. Those patients who responded tended to exhibit more abnormalities on physical examination, but the difference in prevalence was not statistically significant.
There was no discernible difference in the patterns of pain relieved (Fig. 4) and not relieved (Fig. 5) by lateral atlanto-axial joint blocks. Patients who responded to blocks and those who did not, equally had pain centred over the suboccipital, low occipital or high occipital regions. The only trend was that patients whose pain was exclusively cervical in distribution and did not encompass or extend into the occipital region were less unlikely to respond to lateral atlanto-axial joint blocks (one positive vs. three negative).
Discussion
The pain maps of the patients in the present study who responded to blocks of the lateral atlanto-axial joints were consistent with those described in normal volunteers following experimental stimulation of the these joints (11). However, they are also consistent with the maps of pain evoked from the atlanto-occipital (11) or the C2–3 zygapophysial joints (12). The distribution of pain therefore is not indicative of its source. This should not be surprising.
The atlanto-occipital joint is innervated by the C1 ventral ramus (34), and the lateral atlanto-axial joint by the C2 ventral ramus (34, 35), while the C2–3 zygapophysial joint is innervated by the C3 dorsal ramus (36). Upon entering the spinal cord, however, all three upper cervical spinal nerves ramify at multiple segments and converge with trigeminal afferents on cells in the dorsal grey column of C1–3 (37–39). Because of this convergence, pain from any of the upper three cervical synovial joints is liable to be perceived in the same region and referred to the occiput and to regions innervated by the trigeminal nerve.
At the outset of the present study it seemed plausible that pain from the lateral atlanto-axial joints (C1–2) would more likely be associated with physical signs at C1–2, such as reduced range of motion at that level or reproduction of pain upon selective rotation of the atlas. This proved not to be the case. The clinical signs assessed in the present study did not validly distinguish those patients who responded to blocks of the lateral atlanto-axial joint from those who did not. At best, they had a positive predictive value of 60%.
The sensitivity and specificity of these signs could not be determined because no patients who lacked the signs were subjected to diagnostic blocks, nor were patients with these signs subjected to blocks at other segmental levels. It was considered unethical, in the first instance, to perform such extraneous procedures while it was not known if any patients, at all, would respond to blocks of the lateral atlanto-axial joints.
The results of the present study provide prima facie evidence that the lateral atlanto-axial joints are not a rare cause of occipital pain. Positive responses to diagnostic blocks were encountered in 60% of patients in whom the diagnosis was suspected. This figure, however, is not an estimate of the prevalence of lateral atlanto-axial joint pain. For that to be determined, a sample of patients with occipital pain would need to be subjected systematically to controlled diagnostic blocks. The results of the present study now indicate that such a controlled study would be ethically justified.
Recognizing the lateral atlanto-axial joints as a source of occipital pain is not an idle academic exercise. In the past there was no treatment that could be offered even if the pain was traced to the lateral atlanto-axial joints. However, encouraging studies have recently reported that lateral atlanto-axial joint pain can be successfully relieved by arthrodesis (40, 41). That being the case, lateral atlanto-axial joint blocks have therapeutic utility. Instead of languishing with chronic pain, patients in whom the lateral atlanto-axial joints can be proven to be the source of pain can be offered definitive treatment.