
Abstract

Introduction
The subclavian steal phenomenon (SSP) leads to several changes in brain haemodynamics, and those changes might cause many clinical manifestations (1), including headaches. To our knowledge, clusterlike headaches secondary to the SSP have never been previously reported.
Case report
A 60-year-old woman, 9 years before her first consultation, started to have recurring attacks of headaches, initially at 3-month intervals, but progressively reaching three to four attacks daily. Headaches were reported to start with a low intensity left frontal pain that increased progressively to a severe lancinating pain over the left frontal area. Bilateral lacrimation and nasal obstruction, more marked on the left side, would occur associated with the pain. Attacks lasted 30–45 min, being triggered by sitting or standing, also emerging during sleep. Between the attacks the patient was asymptomatic. Her neurological examination was normal, but her physical examination disclosed absence of the left radial pulse. Brain angiography disclosed an occluded left subclavian artery. There was retrograde flow from the left vertebral artery to the left subclavian artery, featuring a SSP (Fig. 1). Indomethacin, up to 150 mg daily, and verapamil, up to 160 mg daily, failed to prevent attacks that could otherwise be arrested by 7 L/min of 100% oxygen by mask for 6 min. The patient was submitted to a safenous vein bypass between the left common carotid artery and the left subclavian artery. The patient presented with only a mild episode of cluster-like headache 30 days after surgery. She has remained asymptomatic during 3 years of follow-up.
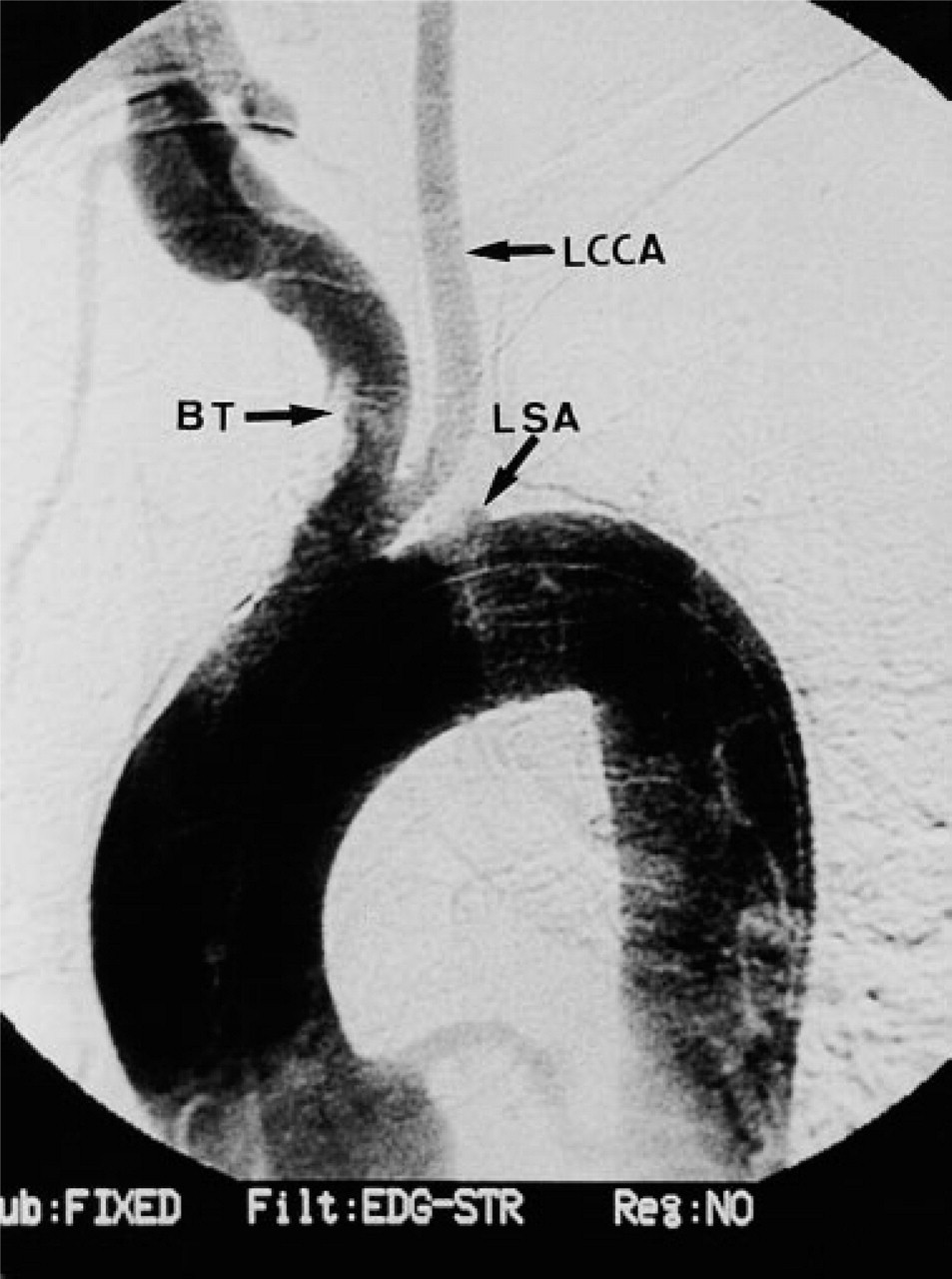
Left common carotid artery (LCCA) originating from the brachiocephalic trunk (BT); left subclavian artery (LSA) obstruction at its origin in the aortic arch.
Discussion
Headache in the SSP occurs as a lancinating pain referred over the mastoid area, radiating to the parietal and occipital aspects of the head. Head pains are chronic or long-lasting, of severe intensity, and triggered by physical activities (1). One of the mechanisms hypothesized for cluster headaches is an impairment of local sympathetic pathways at the middle fossa (2), leading to an increase of the cavernous sinus blood flow and secondary venous distention and pain. The severity of pain may lead to a reactive vasoconstriction of arteries innervated by the sympathetic pathways, pain resuming as a consequence of the blood flow reduction (3). When those arteries relax, new bouts of pain may occur. The headache attacks keep recurring until normalization of the vascular and/or sympathicoplegic changes (4).
Recent studies carried out on patients with cluster headache have shown abnormalities in pulse and blood pressure responses, suggesting more widespread abnormalities of the sympathetic mediated vascular responses (5). Changes in brain blood flow, associated with dilation of the middle cerebral artery, unrelated to sympathicoplegia, have been reported to occur on the same side of the cluster headache (6). This finding suggest that brain hypoxia, such as that seen in sleep apnoea, might be a triggering factor for cluster headache attacks (7). Although cluster headache responsiveness to oxygen inhalation therapy supports this view, it has been disputed by recent evidence (8). In episodic cluster headache, an increase in pCO2 during brain hypoxia lowers vascular tone, leading to an increase in blood flow at the common carotid arteries and to a painful dilation of the cavernous sinus and its tributary veins (9).
The bypass between the left vertebral artery and the left subclavian artery has been shown to determine an increase of the blood flow in all the large intracranial arteries. Increase ratio was reported to be of 78% for the left vertebral artery, 22% and 23% for the right and the left common carotid arteries, respectively, and 43% and 45% for the right and the left internal carotid arteries, respectively. In spite of the increased intracranial blood flow, there is a 37 mL/min steal of blood from the brain to the left subclavian artery, through the left vertebral artery, which leads to a 41% reduction of the oxygen supply to the brain and to an increase of the pCO2 at the jugular veins (1).
Recurrent and transient brain hypoxia, associated with an increased blood flow at the internal carotid arteries, and with a secondary engorgement of the cavernous sinuses (1), can hypothetically lead to cluster-like headaches. In the case described above, increased blood flow in the intracavernous carotid arteries, secondary to brain hypoxia due tho the SSP, may have been the pathophysiological basis of the cluster-like headache. It is our opinion that in patients presenting with cluster-like headaches, a SSP should be carefully sought, as the headache may be an ominous sign of an impending brain ischaemia.