
Abstract
This paper describes the vascular effects of almotriptan in comparison with sumatriptan in human vessels and tissues in vitro. The contractile properties of almotriptan and sumatriptan were evaluated in vitro in the following arteries: meningeal, temporal, basilar, internal carotid, ophthalmic, pulmonary and coronary. In addition, the effects of almotriptan on the pulmonary vein and on bronchial tissues were studied. Almotriptan showed selectivity of action for migraine-related arteries (i.e. contractile EC50 of 30 and 700 nM for meningeal and temporal arteries, respectively), whereas the effect on arteries supplying blood to the brain was lower. The contractile effect of almotriptan was lower than that of sumatriptan in pulmonary arteries, whereas in bronchial preparations no clinically relevant contractile responses were observed for either almotriptan or sumatriptan. In ophthalmic arteries the contractile effects of almotriptan and sumatriptan were similar, whereas lower contractile effects were obtained with almotriptan than with sumatriptan in coronary arteries.
Introduction
Migraine, which affects up to 16% of the general population, is characterized by a pulsating unilateral headache lasting for hours and is often associated with other neurological alterations, such as aura. Acute episodes vary in frequency, from one to six per month, and mostly affect women (1). As migraine often prevents people from working it has important economic implications (2).
Sumatriptan is a 5-HT1B/1D agonist, with proven efficacy in relieving migraine (3). However, its low bioavailability and side-effects – namely paraesthesiae, flushing and chest pain – have meant that the search for new compounds has been ongoing (4). Consequetly, other 5-HT1B/1D receptor agonists are under study, in late clinical development, or on the market (e.g. zolmitriptan, rizatriptan, naratriptan and almotriptan) (5).
Sumatriptan is known to cause vasoconstriction in certain cerebral arteries (3) and recent studies have demonstrated that in human middle meningeal arteries and cerebral arteries the vasoconstrictor effects of triptans are mediated through the 5-HT1B-receptor subtype (6, 7). Nevertheless, the effects of 5-HT1B/1D agonists, including 5-HT, on human bronchial muscle are still not fully understood. In the human isolated bronchus, 5-HT has been shown to cause contraction (8), minor responses or relaxation (9, 10). The effects of inhaling 5-HT in humans have yet to be confirmed (11, 12). On the other hand, the human pulmonary artery and vein have a mixed functional population of 5-HT1B/1D and 5-HT2A receptors mediating the contractile response to 5-HT (13) as suggested also by binding studies, but at physiological and pathophysiological concentrations of 5-HT the vasoconstriction in pulmonary arteries is mediated by the 5-HT1B receptor (14).
Chest symptoms associated with sumatriptan treatment have been related to coronary vasoconstriction, although extracardiac mechanisms have also been suggested (15). Thus, there is considerable interest in the development of compounds with less spasmogenic capacity at the coronary level (16). Recent studies suggest that the contractile effects of sumatriptan on human coronary arteries involve the 5-HT1B and 5-HT2A receptors rather than the 5-HT1D receptor (17). This assertion is supported by the fact that a recently developed selective 5-HT1D agonist, L-775,606, showed less vasoconstriction in coronary arteries than mixed 5-HT1B/1D-receptor agonists (34).
This study was designed to evaluate the in vitro effects of almotriptan, a new 5-HT1B/1D agonist (18), in comparison with sumatriptan in meningeal, temporal, basilar, internal carotid, ophthalmic, pulmonary and coronary arteries. In addition, the in vitro effects of almotriptan and sumatriptan were compared in the human pulmonary vein and bronchial tissue. The results of this study are intended to further characterize the profile of almotriptan regarding its pharmacology and safety for treating migraine patients.
Materials and methods
Tissue samples
Human vessels were obtained from autopsies carried out in the Pathology and Anatomy Department of the Hospital Clı́nic i Provincial de Barcelona (School of Medicine, University of Barcelona, Barcelona, Spain), with the exception of the samples from lung tissue, which were obtained from patients who had undergone surgery for carcinoma of the lung (Chest Surgery Unit, Hospital Universitario La Fe, València, Spain). After the resection of a lung or pulmonary lobe, healthy parts of the bronchus, pulmonary artery and vein were dissected from the macroscopically abnormal lung tissue. Specimens were collected in accordance with Spanish legislation.
All the donors were Caucasian.
Meningeal arteries
The upper part of the dura mater containing the meningeal arteries was dissected from 15 donors of each sex, aged between 52 and 85 years. After extraction, the samples were placed in Krebs solution at 4°C.
The meningeal arteries were cannulated with Microlance 3, 21G (0.8 ×
2.5 mm) needles, connected to polyethylene cannulas 1.22 × 0.76 mm in
diameter. The meninges were placed on an anatomical support in a thermostatic
chamber at 37°C. Immediately, Krebs solution at constant flow (5
ml/min) at 37°C gassed with 5% carbon dioxide in oxygen
and supplemented with N-nitro-l-arginine-methyl-esther (L-NAME, 10
µ
Each preparation was used for a single curve with the agonist used, although a variable number of concentration-response curves (from one to four) were obtained depending on the integrity of the meningeal artery. The response of the perfused vessel is measured as a change in perfusion pressure in mmHg. Almotriptan was studied in seven preparations and sumatriptan in 11.
Temporal arteries
Temporal tissues were obtained from five donors of each sex, aged between 62 and 80 years. After extraction, the samples were placed in Krebs solution at 4°C. Rings of 2–3 mm in width were cut and suspended isometrically at a tension of 2 g in organ baths (Letica, LE 01.004) containing Krebs solution at 37°C, gassed with 5% carbon dioxide in oxygen. Almotriptan was studied in 23 preparations and sumatriptan in 21.
Basilar arteries
Tissues were obtained from 14 donors of each sex, aged between 40 and 84 years and with no clinical evidence of vascular disease. After extraction the samples were maintained in Krebs solution at 4°C. Rings of 2–3 mm in width were cut and suspended isometrically at a tension of 2 g in organ baths containing Krebs solution at 37°C, gassed with 5% carbon dioxide in oxygen. The maximum possible number of rings was obtained from each donor. Tissues were distributed between 5-HT (n = 10, three donors), almotriptan (n = 12, four donors) and sumatriptan (n = 11, four donors).
Internal carotid arteries
The tissues were from donors of both sexes, aged from 51 to 85 years. After extraction, the samples were kept in Krebs solution at 4°C. Rings of approximately 2–3 mm in length were obtained, and suspended isometrically under 2 g resting tension in organ baths containing Krebs solution at 37°C, gassed with 5% carbon dioxide in oxygen. The maximum number of preparations possible was obtained from each sample for use with almotriptan (n = 9, six donors) or sumatriptan (n = 9, five donors).
Ophthalmic arteries
Helicoid preparations of human ophthalmic artery came from eight donors of both sexes, aged between 61 and 79 years. After extraction, the samples were preserved in Krebs solution at 4°C. Spirals 1–2 mm wide and approximately 10 mm long were obtained, and isometrically suspended at a tension of 2 g in organ baths containing Krebs solution at 37°C, gassed with 5% carbon dioxide in oxygen. The greatest number of preparations possible was obtained from each donor and assigned to test 5-HT (n = 4, four donors), almotriptan (n = 5, five donors) or sumatriptan (n = 7, seven donors).
Pulmonary tissues
Vascular or bronchial ring preparations (3–4 mm length × 2–3 mm internal diameter) were set up under 2–2.5 g of initial load to ensure that responses to spasmogens were maximal. The tissues were allowed to equilibrate for 90 min in Krebs solution at 37°C, gassed with 5% carbon dioxide in oxygen. Changes in force were measured from isometric recordings.
Coronary arteries
Two female donors were selected (aged 27 and 54 years), with no heart disease or coronary atheromatous inclusions. After extraction, the samples were kept in Krebs solution at 4°C. Rings of 2–3 mm in length were obtained, and suspended isometrically at a tension of 2 g in organ baths containing Krebs solution at 37°C, gassed with 5% carbon dioxide in oxygen. Almotriptan was studied in 17 preparations and sumatriptan in 14.
Experimental procedure
After a 30–45-min stabilization period, the functionality of the
tissue was tested with 40 m
Recording systems
The recording systems employed were: TRA 021 pressure transducers, TRI 010 isometric transducers, PRS 205/206 amplifiers and Letigraph 4000/4006 polygraph, from LETICA (L'Hospitalet del Llobregat, Spain); K30 isometric transducers, DBA amplifiers and Mark 8 polygraph, from Hugo Sachs (March-Hugstetten, Germany); and isometric force-displacement transducers (FTO3) and a model 7P Grass polygraph, from Grass Instruments (Quincy, Massachusetts, USA).
Evaluation of data and statistics
The values were expressed as a percentage (mean±
Solutions and compounds
The Krebs solution composition was (in mM) NaCl 118, KCl 4.7, NaHCO3
25, MgCl2 1.2, CaCl2 2.6 and glucose 11.1. L-NAME
(hydrochloride) was dissolved directly in the perfusion fluid. Ach (chloride),
5-HT (creatinin sulphate) and almotriptan (hydrochloride or malate acid) were
dissolved in distilled water. Sumatriptan (base) was dissolved in distilled
water and 0.5% 1 N HCl at the initial concentration of 1 m
Results
Meningeal arteries
Almotriptan was superior to sumatriptan in terms of both potency and efficacy (Fig. 1 and Table 1) in contracting the meningeal artery. Indeed, almotriptan was seven-fold more potent than sumatriptan reaching statistical significance (P < 0.05) (Table 1).
Comparative contractile effects of almotriptan and sumatriptan on several human tissues

EC50 (µM) is the drug concentration that produced 50% of the contractile effect elicited by initial 5-HT; Emax is the maximum effect elicited in percentage of 5-HT. In human bronchus the used reference compound was ACh.
∗ P < 0.05 and
∗∗∗ P < 0.001 vs. sumatriptan, Student's t-test.

Cumulative concentration–response curves to almotriptan
(▪) and sumatriptan (▴) in human isolated
meningeal arteries. Data are expressed on the ordinate as a percentage
of the response elicited by a 0.1-µ
Temporal arteries
Figure 2 shows that almotriptan and sumatriptan had a similar effect on temporal artery tissue. Both compounds showed comparable maximum effects; 5-HT produced greater response, probably by activating 5-HT2 receptors in addition to 5-HT1 receptors, whilst triptans act only at 5-HT1B receptors (Table 1).
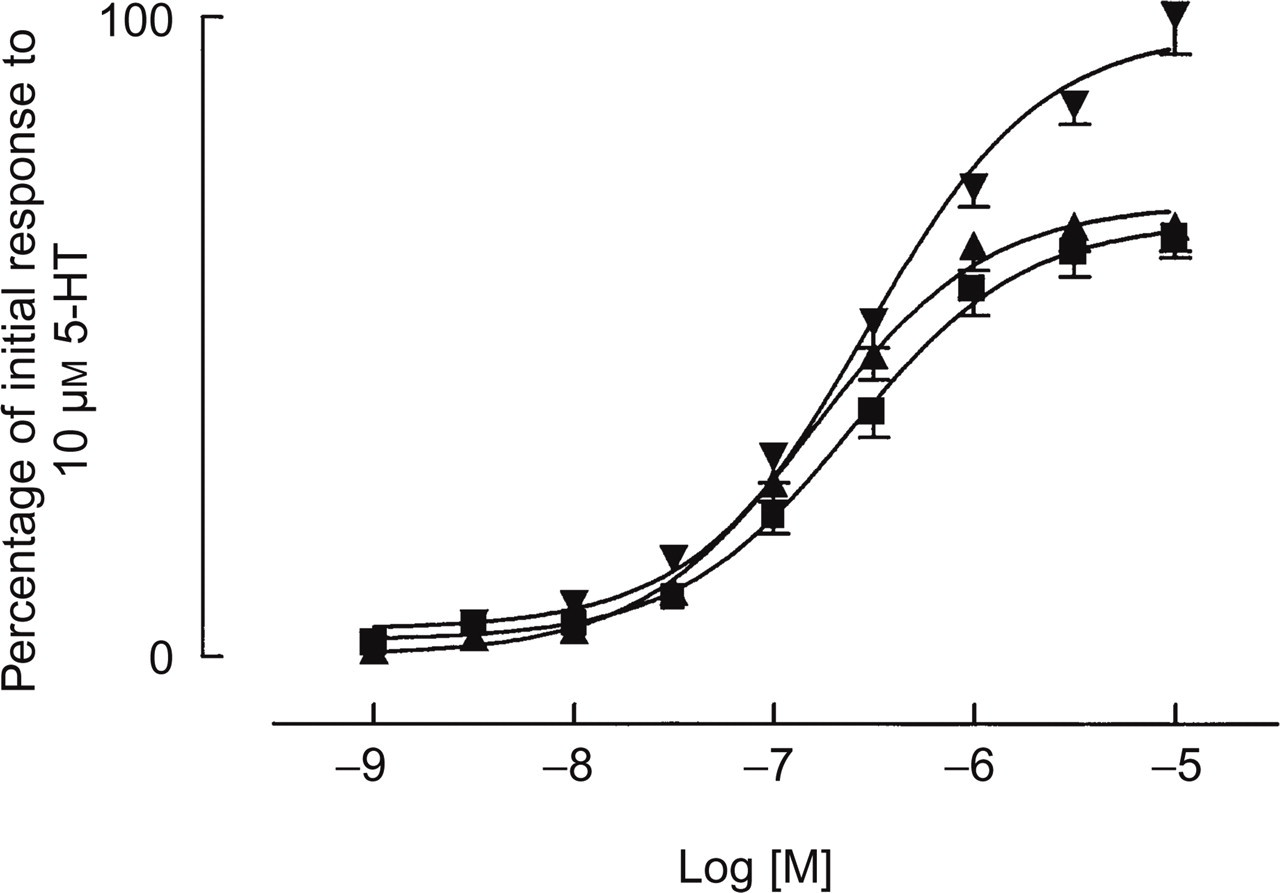
Cumulative concentration–response curves to almotriptan
(▪), sumatriptan (▴) and 5-HT (▾) in
human isolated temporal arteries. Data are expressed on the ordinate as
a percentage of the response elicited by 10 µ
Basilar arteries
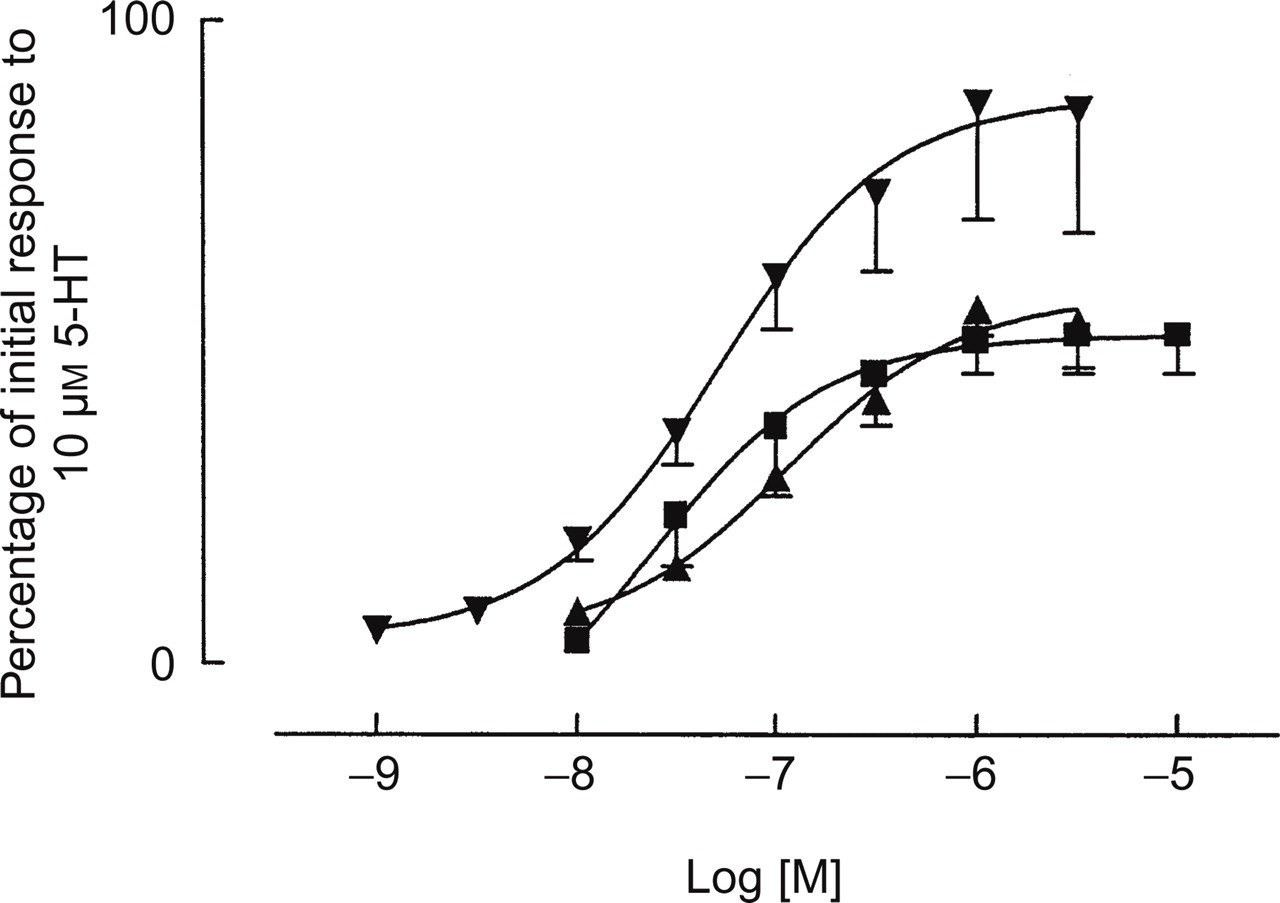
Almotriptan was found to contract basilar artery tissue with less potency and efficacy in comparison with sumatriptan and 5-HT (Fig. 3 and Table 1). The contractile effect of almotriptan on the basilar artery was 12 times less potent than that of sumatriptan reaching statistical significance (P < 0.001).

Cumulative concentration–response curves to almotriptan
(▪), sumatriptan (▴) and 5-HT (▾) in
human isolated basilar arteries. Data are expressed on the ordinate as a
percentage of the response elicited by 10 µ
Internal carotid arteries
The results for internal carotid artery demonstrate that almotriptan and sumatriptan had the same maximum effects, their spasmogenic potential being inferior to that of 5-HT (Fig. 4). No statistically significant differences in potency were observed.
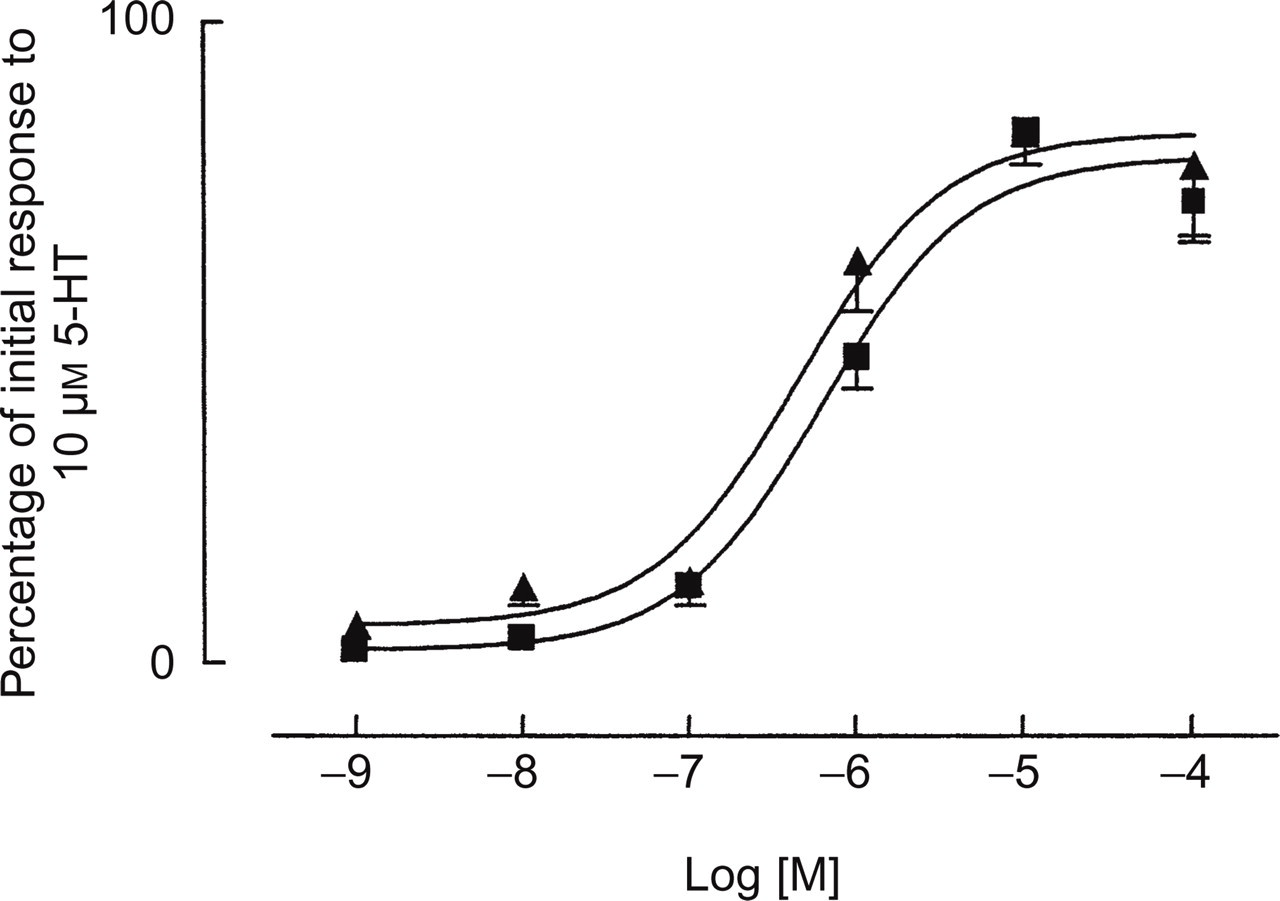
Cumulative concentration–response curves to almotriptan
(▪) and sumatriptan (▴) in human isolated internal
carotid arteries. Data are expressed on the ordinate as a percentage of
the response elicited by 10 µ
Ophthalmic arteries
Almotriptan and sumatriptan produced smaller contraction than 5-HT, probably by the same reason exposed for temporal arteries. Almotriptan and sumatriptan had similar maximum effects (Table 1) but the potency of both compounds was significantly (P < 0.05) inferior to that of 5-HT (pEC50 7.32) (Fig. 5).
Cumulative concentration–response curves to almotriptan
(▪), sumatriptan (▴) and 5-HT (▾) in
human isolated ophthalmic arteries. Data are expressed on the ordinate
as a percentage of the response elicited by 10 µ
Pulmonary tissues
Responses in human isolated vascular preparations
In human pulmonary arterial preparations, almotriptan (0.1–10
µ
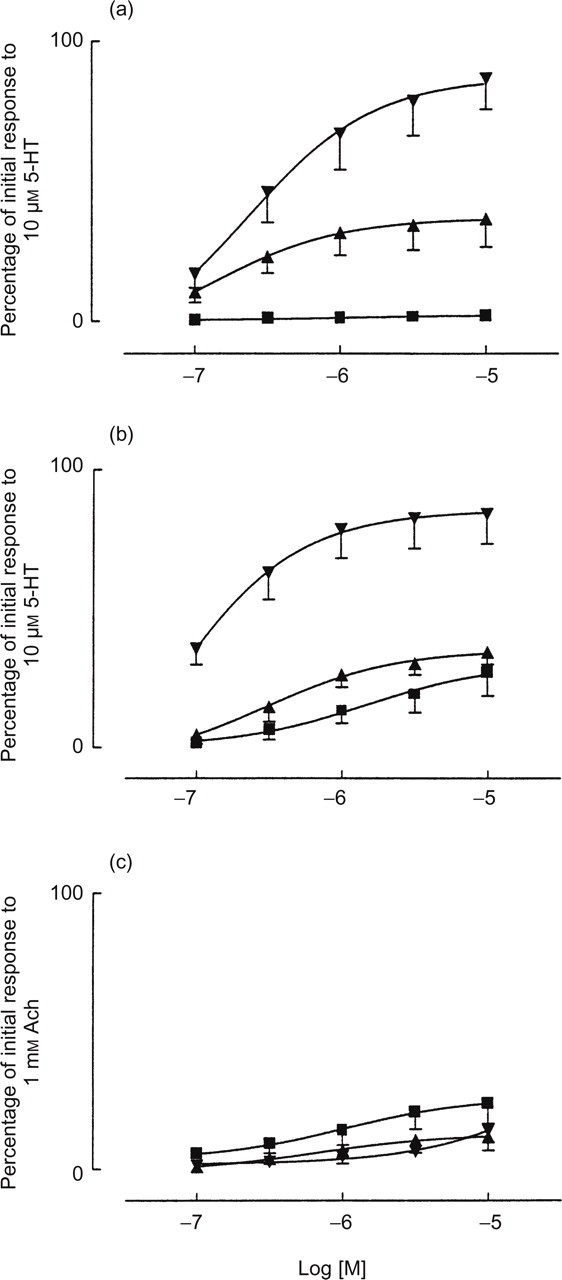
Cumulative concentration–response curves to almotriptan
(▪), sumatriptan (▴) and 5-HT (▾)
in human isolated pulmonary artery (a), pulmonary vein (b) and
bronchus (c). Data are expressed on the ordinate as a percentage of
the response elicited by 10 µ
Both almotriptan and sumatriptan contracted the pulmonary veins but their efficacy was substantially less than that of 5-HT (Fig. 6). Significant differences were not found in the potency of almotriptan and sumatriptan in pulmonary veins (Table 1).
Responses in human isolated bronchus
5-HT produced very small contractile responses in bronchial preparations
(Fig.
6). The contraction to the highest concentration tested (10
µ
Coronary arteries
The results obtained indicate that both almotriptan and sumatriptan have less affinity for the receptor than 5-HT (Fig. 7). The concentration–response curves indicate that almotriptan has a statistically significant (P < 0.05) lower spasmogenic capacity compared with sumatriptan in the human coronary artery (Table 1).

Cumulative concentration–response curves to almotriptan
(▪), sumatriptan (▴) and 5-HT (▾) in
human isolated coronary arteries. Data are expressed on the ordinate as
a percentage of the response elicited by 10 µ
Discussion
Almotriptan has demonstrated anti-migraine activity in clinical trials (19) and has been shown to have high oral bioavailability (70%) in humans (20). This paper is the first to report in detail the effects of almotriptan, a selective and potent 5-HT1B/1D agonist (18), in preparations of isolated human blood vessels. The contractile effects of almotriptan were studied, in comparison with sumatriptan, using isolated vessels from the brain (meningeal, temporal, basilar and internal carotid arteries) and other relevant vascular beds, including coronary arteries.
Meningeal arteries were identified as the target organs to determine the vasoconstrictor action of triptans and it is fully accepted that tissue perfusion assays are more predictive of what will occur in physiological conditions because both resistance and conductance vessels are involved. In contrast, the ring preparation shows only a vasoconstrictor effect, mainly in capacitance vessels. The effects of almotriptan and sumatriptan were therefore studied in the perfused meningeal arteries preparation. In the present experiment with perfused human meningeal arteries, almotriptan proved to have a statistically significant, seven-fold greater potency and a greater effectiveness in contracting this vessel in comparison with sumatriptan. These effects are probably due to an agonistic activity on the 5-HT1B receptor population (6).
Sumatriptan is the most widely studied triptan in different isolated human cerebral arteries. According to the literature, as reviewed by Perry and Markham (3), sumatriptan produced contractile effects on human isolated cerebral, meningeal, temporal arteries and basilar, pial and dura mater vessels. The contractile effects of sumatriptan on isolated rings of human meningeal arteries have been studied by several authors, who have reported obtaining the following pEC50 values: 7.28, 7.15, 7.05, 6.91 and 6.5 (6, 21–24). Similar pEC50 values have been reported for rizatriptan and eletriptan: 7.05 and 7.30, respectively (21, 22). In the present study the Emax of almotriptan was significatively higher than that of sumatriptan.
On the human superficial temporal artery, almotriptan presented a vasoconstrictor
profile similar to that of sumatriptan (EC50 of 0.7 and 0.4
µ
In the present study, almotriptan showed no differences in contractile effects in comparison with sumatriptan on either the internal carotid artery or the ophthalmic artery. Sumatriptan has been said to cause constriction of the internal carotid artery in patients during migraine attacks (26). However, to our knowledge there are no in vitro studies of the effect of triptans on internal carotid arteries or ophthalmic arteries.
Although some patients have experienced chest pain or symptoms of angina pectoris
after the use of sumatriptan (27), it is not clear whether the
chest pain is associated with patients' cardiovascular risk factors or
not (28). Other
possible explanations for these symptoms include pulmonary vasoconstriction,
oesophageal spasm, intercostal muscle spasm or bronchoconstriction (15). 5-HT has
previously been shown to induce spasms of pulmonary blood vessels in human
preparations (13), whereas almotriptan and sumatriptan have low or minor contractile
effects on human pulmonary vascular smooth muscle. In addition, the responses
elicited by almotriptan in the present study were substantially smaller than those
produced by either 5-HT or sumatriptan (except in veins). Recently, Morecroft et al.
(14)
demonstrated maximum contractile response to sumatriptan in pulmonary arteries,
similar to the maximum contraction of the tissue in response to 50 m
In non-precontracted bronchial preparations, almotriptan and sumatriptan produced minor contractile responses that would not be likely to have clinical relevance and that were similar to those obtained with 5-HT.
The potential of sumatriptan to cause cardiac ischaemia is supported by its contractile effects on normal and atherosclerotic isolated human coronary rings from explanted hearts (29). In addition, a recent review (36) showed that triptans moderately contract isolated human coronary arteries. The potencies (pEC50) reported for sumatriptan ranged between 6.10 and 6.70. On the other hand, the magnitude of contraction effected by sumatriptan observed in the present study (77 ± 10%) differ from those reported previously (ranging from 21 to 43%). However, the recent study by Longmore et al. (34) found the contractile effect of sumatriptan on isolated coronary arteries to be approximately 60%, a figure that is consistent with our own observation. These discrepancies, together with the aforementioned ones concerning temporal arteries, may be attributable to different methodological approaches, as the present study was performed on human samples coming from necropsies, whereas other studies used fresh samples obtained during surgery (24, 34, 35, 37) or from heart-beating organ donors (30). In addition, some authors have used vessels that were endothelium-denuded (34), while others used intact vessels (24, 30, 35) even though the integrity of the endothelium sometimes was not tested (37), as we did not. As far as we know, Maassen Van Den Brink et al. are the only authors that have compared the effects of most triptans on human coronary arteries using the same experimental conditions for all compounds (30). Their study compared the contractile effects of nine anti-migraine drugs on isolated human coronary rings and they further analysed the relationship between the coronary contractile effects (EC50) and the human plasma levels (Cmax) reached by a therapeutic dose of the compound, devising a ratio to estimate the coronary constriction to be expected during therapeutic use. The greater the value of the ratio, the lower the safety margin of the compound. Applying the same approach to the present study, almotriptan at the dose of 12.5 mg gave plasma levels of 49.5 ng/ml (31), thus giving a ratio of 0.03 which was lower than the values obtained for oral sumatriptan at a dose of 100 mg (ratio 0.14–0.18) and subcutaneous sumatriptan at a dose of 6 mg (ratio 0.24–0.26). This suggests that almotriptan's vasoconstrictive effect on isolated human coronary rings is lower than that of sumatriptan at effective therapeutic doses.
In summary, almotriptan has a greater contractile effect than sumatriptan on vessels responsible for migraine attacks (i.e. meningeal arteries); a similar effect to sumatriptan on cranial vessels that are not clearly related to migraine and on extracranial vessels, and a lower contractile effect on vessels that have putatively been linked to some adverse events in association with sumatriptan treatment (i.e. on coronary arteries). The results of the present study match those of clinical studies demonstrating that almotriptan 12.5 mg has very good anti-migraine activity and is very well tolerated (32).
Footnotes
Acknowledgements
The skillful technical assistance of L. Capdevila, A. Coll, J. Prieto, M.C. Soler and M. Verdú is acknowledged. We specially thank also J. Prieto for data management and Mary Ellen Kerans for correction of the English style.