
Abstract
Objectives
To investigate prognostic factors for long-term outcome of patients after inpatient withdrawal because of drug-induced chronic daily headache.
Procedures
Fifty-five patients (36 females) were re-examined by means of a standardized interview after inpatient withdrawal. The mean observation period was 9.28 ± 2.85 years (mean ±
Results
Five years after withdrawal, one-third of the patients (34.6%) had an overall favourable outcome, one-third (32.7%) had no recurrent drug overuse and reported a clear-cut improvement of headache, and one-third (32.7%) developed recurrent drug overuse. Most relapses occurred within 2 years, and a small percentage within 5 years. No predictors for long-term outcome after inpatient withdrawal were found.
Conclusions
All patients with drug-induced chronic daily headache should be considered as good candidates for inpatient withdrawal, and no patient should be excluded from that therapy.
Keywords
Introduction
Recurrent headache, particularly migraine (MIG) as well as tension-type headache (TTH) (1, 2), often leads to excessive analgesic and/or ergotamine intake and the development of drug-induced chronic daily headache (CDH) (3–7). CDH refers to headache that occurs at least 15 days per month with an average duration of at least 4 h (8). CDH can evolve from an initial headache type of MIG, developing into transformed migraine (TM), as well as from episodic TTH, developing into chronic tension-type headache (CTTH) (9). In rare cases, CDH occurs abruptly as new daily persistent headache (NDPH) (within < 3 days) without remission (8). The development of TM and CTTH does not necessarily depend on medication overuse (8), but there is a high coincidence of CDH and medication overuse, leading to the vicious circle of chronic substance-induced headache. The latter is defined as the daily ergotamine intake (oral > 2 mg, rectal > 1 mg) for at least 3 months or as the intake of at least 50 g of aspirin per month or an equivalent of other mild analgesics for at least 3 months (1). All drugs with a potential psychotropic effect, including analgesics and ergotamine (10–12), can lead to dependency. However, concerning the development of drug overuse, headache patients are more prone to be caught in that vicious circle than patients suffering from other pain (13). The pathogenesis of drug overuse in patients suffering from substance-induced headache is not known in detail (12). The only effective therapy is to break the habit of recurrent but ineffective drug intake by drug withdrawal (13–18).
In earlier studies, we have already tried to find out predictive factors with regard to the outcome after withdrawal in patients with headache and drug overuse. The results were equivocal; in one sample we could not find any predictive factor (16), in the other study we found some tendencies for distinct patient groups (17). Literature on this topic is scant and the results are equivocal (15, 19–21).
In patients with drug-induced CDH, earlier investigations (22) found a significantly reduced critical flicker frequency as a subclinical sign of subtle organic brain syndrome and increased values in the MMPI (Minnesota Multiphasic Personality Inventory) scales of hypochondriasis, hysteria and depression. At least for hours to days, occupational performance is reduced in many of these patients. An inpatient withdrawal for approximately 10–12 days is a financial burden for the public health system (23). Thus, it is of great relevance to evaluate the long-term efficacy of treatments offered to patients with headache and drug overuse. The present study was therefore carried out to identify prognostic factors concerning the long-term course of patients after drug withdrawal because of drug-induced CDH.
Patients and methods
In our second long-term outcome study after inpatient withdrawal because of medication-induced headache (17), we re-evaluated 38 patients who had been treated at the Department of Clinical Neurology at the University of Vienna from 1984 to 1990. All those patients were contacted by mail again in 1999, and 29 of them were re-interviewed for the present study. Additionally, another 26 patients, who had undergone inpatient withdrawal between 1991 and 1994, were interviewed. Thus, a total of 55 patients (36 female, 19 male) were investigated by personal (n = 27) or telephone (n = 28) interview. The mean observation period was 9.28 ± 2.85 (mean ±
Before withdrawal, all patients had suffered from CDH of severe intensity, most of them with a frequency far beyond the above mentioned cut-off of at least 15 days per month (8). For withdrawal, the patients were admitted to the hospital for 10–12 days and drug intake was discontinued abruptly. To mitigate possible rebound effects, the patients received metamizol, metoclopramide, piracetam and, if necessary, diazepam, given intravenously per infusion. Furthermore, all patients received tablets containing prothipendyl, a mild neuroleptic substance. To avoid venous thromboembolism, all patients received low-molecular-weight heparin subcutaneously. Break-through migraine attacks were treated with triptans. After the first week, a basis prophylaxis was initiated in most cases. Patients with MIG received predominantly beta-blocking agents (metoprolol, propranolol or atenolol) and/or tricyclic antidepressants. In a few cases, we offered the calcium-channel blocker flunarizine or valproate. Patients with TTH received tricyclic antidepressants (amitriptyline or doxepine).
The clinical outcome was evaluated by means of a standardized interview. The following factors were selected as possible predictive factors (Table 4): initial headache type (MIG vs. TTH), substance overused (containing ergotamine vs. containing no ergotamine), gender, amount of doses taken per month (more vs. less than 160 doses a month, the sample was dichotomized), family history of headache in parents, arterial hypertension, arterial hypotension, smoking, alcohol intake (no intake; no more than 400 g per week; more than 400 g per week), educational level, profession (blue vs. white collar workers), private living situation (singles vs. living together with other person(s)), age at onset of headache, age at onset of drug overuse, age at withdrawal, duration from onset of headache to onset of overuse, duration of overuse, and duration from onset of headache to drug withdrawal. Five years after drug withdrawal, the clinical outcome was evaluated using three different categories. The long-term outcome was defined as ‘good’ in patients with:
Outcome 5 years after drug withdrawal. Positive outcome: no or only mild intensity of headache, less than 8 1s with headache per month, no recurrent drug overuse. Fisher's exact test (two-tailed); given are P-values; n.s. not significant

a headache frequency of < 8 days per month;
a headache intensity of at most ‘mild’; and
no recurrent drug overuse.
Descriptive univariate tests without multiplicity adjustment were performed using Fisher's exact test (two-tailed). To analyse the time periods until the re-occurrence of headache, the re-occurrence of medication intake, and the re-occurrence of drug overuse, stepwise Cox proportional hazard models were used. The following prognostic factors were available for stepwise selection: gender, profession, headache type, substance overused, duration of overuse, and age at withdrawal. A P-value < 0.05 was taken as an indication for the significance of a factor for prognosis.
Results
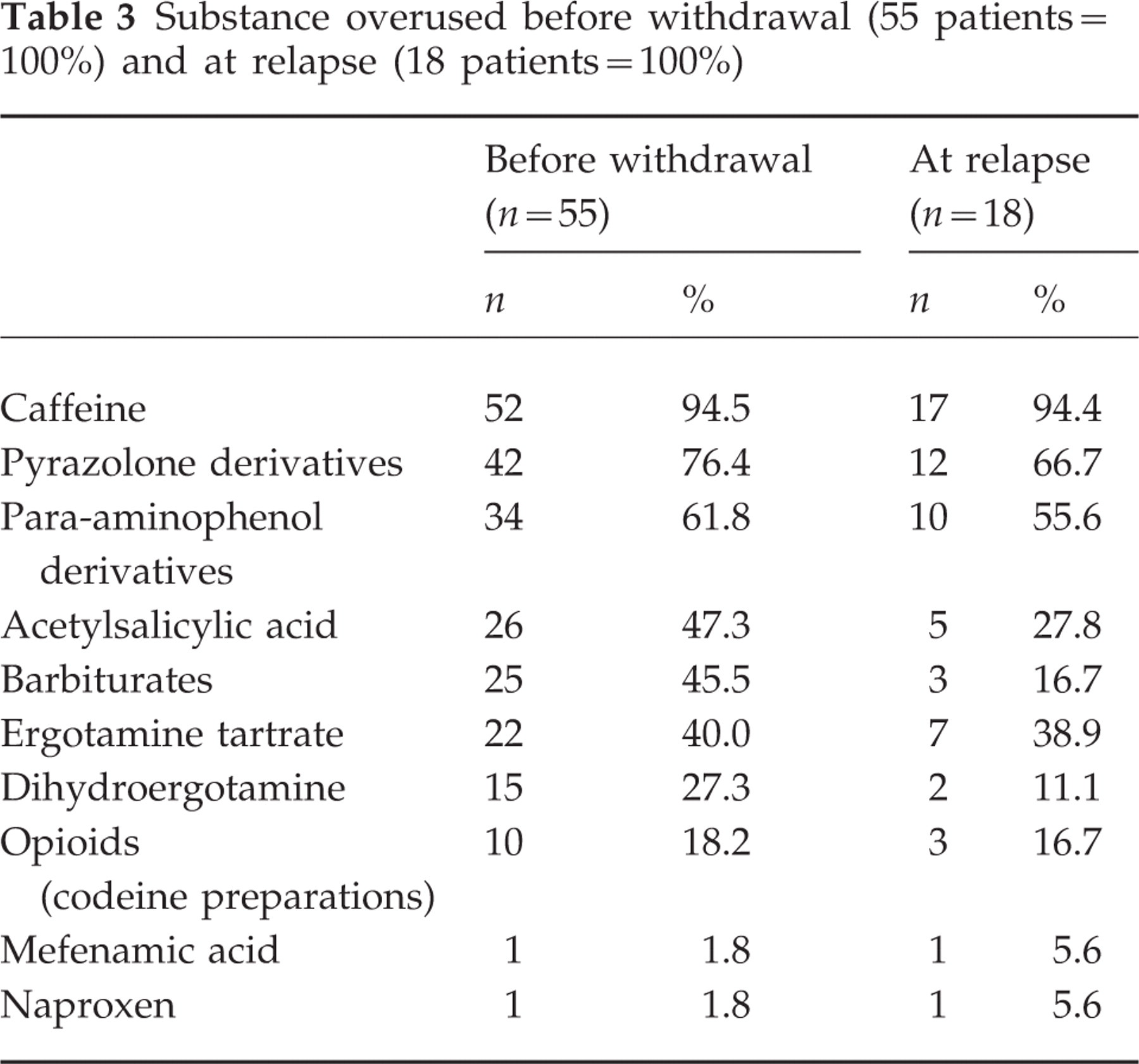
The headache types, the substances overused, the histories, as well as the sociodemographic characteristics, of all 55 patients are shown in Table 1. The data concerning drug overuse and withdrawal are given in Table 2. Percentages of the different substances overused before withdrawal and at relapse are shown in Table 3.
Substance overused before withdrawal (55 patients=100%) and at relapse (18 patients=100%)
Data concerning drug overuse and withdrawal (n = 55; mean ±

Patients’ characteristics

Five years after inpatient withdrawal, 19 patients (34.6%) had an overall favourable outcome in all three categories (frequency of less than 8 days with headache per month, no or only mild intensity of headache, and no recurrent drug overuse). A further 18 patients (32.7%) exhibited no recurrent drug overuse and 18 patients (32.7%) relapsed. Sixteen (88.9%) of the relapsing patients overused the same drugs again, except for barbiturates, which successively came out of use because of governmental restrictions in the 1990s. From those 18 patients with recurrent drug overuse, 13 relapsed within 2 years and the remaining five patients within 5 years. After more than 5 years, no further relapse was observed (mean observation period: 8.92 ± 2.75 years; range 5.00–13.50 years).
Not even one predictive factor was identified with regard to any of the three outcome categories (headache frequency; headache intensity; no recurrent drug overuse) (Table 4). However, concerning headache intensity, a tendency towards a better outcome was found for patients suffering from migraine. Patients at a lower age at withdrawal exhibited a tendency towards a better prognosis with regard to the frequency of headache after inpatient withdrawal. None of the prognostic factors of gender, profession, headache type, substance overused, duration of overuse and age at withdrawal was observed to be of significant influence on either the time until the re-occurrence of headache, the re-occurrence of medication intake or the re-occurrence of drug overuse.
Discussion
One-third of our patients (34.6%) had an overall favourable outcome, one-third (32.7%) experienced a clear-cut improvement with regard to the frequency and the intensity of headache and developed no recurrent drug overuse, and one-third of the patients (32.7%) relapsed. In the last group, the substances overused at relapse were mostly the same. The reduction in barbiturate overuse does not correspond with a better outcome but is an artificial effect because of governmental restriction.
No predictors for long-term outcome after inpatient withdrawal were found. In accordance with the results of previous studies, a tendency towards a better outcome (intensity) was found for patients with MIG compared with patients suffering from TTH (15, 17). In addition, in comparison with older patients, younger patients exhibited a tendency towards a better prognosis (frequency). Smokers and singles also showed a statistically noticeable better outcome regarding headache intensity and recurrent drug overuse, respectively. At the moment we cannot interpret these findings clearly; further studies will be necessary.
In the literature, the results are not conclusive (Table 5). In the study by Tfelt-Hansen et al. (19), the prognosis of patients with ergotamine overuse was better in cases with a short duration of drug overuse than in cases with drug overuse over a longer period. Diener et al. (15) found MIG as primary headache (vs. TTH or ‘combination’ headache), chronic headache lasting less than 10 years, and regular intake of ergotamine (vs. other analgesics including barbiturates), as predictors for a successful treatment. In the study performed by Suhr et al. (21), only the headache type (TTH or combined headache) presented as a statistically significant risk factor for a relapse. In a former study (16), including a sample of 38 patients after inpatient withdrawal, we could not identify any predictive factor concerning the probability of recurrent drug overuse. Schnider et al. (17) re-examined 38 patients with CDH and ergotamine and/or analgesic overuse 5 years after inpatient drug withdrawal. With respect to recurrent drug overuse, none of the 12 variables investigated proved to be a significant predictor for a favourable outcome. There was, however, a tendency towards a better prognosis for patients with MIG compared with patients with TTH (P < 0.1) or to patients with combined MIG and TTH (P < 0.1), respectively. Regarding the frequency of headache, a shorter mean time interval between the onset of drug overuse and withdrawal was predictive for good long-term outcome. Regarding the intensity of headache, patients with a favourable outcome had taken significantly less tablets per month.
Predictive factors after withdrawal of drug overuse in chronic daily headache (literature survey)

However, other variables may influence the long-term outcome. In the process of chronification, Siniatchkin (24) found an analgesic overuse less essential than the degree of psychological disability. He assumed that improvement among patients during acute withdrawal resulted from the behavioural effect, with a change in patient's attribution and the possibility of coping strategies other than analgesic intake. Based on a literature survey from 1966 to June 1998, Zed (25) proposed that the long-term prognosis does not depend on the method of withdrawal, but rather on the degree of follow-up, education, and support provided.
In conclusion, 5 years after inpatient drug withdrawal, one-third of the patients had an overall favourable outcome, one-third had no recurrent drug overuse with a clear-cut improvement of pain, and one-third developed recurrent drug overuse. Our data show that the majority of relapses occur within the first 2 years after withdrawal, and a small percentage of patients relapse within 5 years. The mean observation period in our patients without relapse was almost 9 years, and a relapse after more than 5 years did not occur. Thus, patients can be considered as healed from drug overuse 5 years after withdrawal. As we found no predictive factors concerning the outcome after drug withdrawal in CDH patients, all patients with analgesic and/or ergotamine overuse can be considered as good candidates, and no patient should be excluded from that therapy.