
Abstract
We evaluate personality traits, anxiety and depression in a population of paediatric and adolescent patients, correlating personality characteristics with headache and sociodemographic variables. The clinical features of headache include specific personality traits. We report a clinical study of 57 patients (age 8–18 years), divided up as follows: 12 migraine with aura, 29 migraine without aura and 16 tension-type headache. One of Cattel's tests was administered to every patient; the Children's Depression Inventory test was administered to 53 patients and the Test Anxiety Inventory test to 43 subjects. The scores obtained by every patient in each test were correlated with the characteristics of headache and with sociodemographic data. We found that patients affected by idiopathic headache share some personality traits, mainly emotional rigidity and tendency to repress anger and aggression. These traits do not seem to be correlated with sociodemographic data and the duration of headache: we considered these as characteristic of migrainous patients.
Introduction
The clinical description of headache often embraces a series of psychopathological personality traits found in anxiety-linked or depressive disorders, with studies of headache based on data of a clinical and epidemiological nature and, in more recent times, on the use of standardized tests and/or check lists. However, it must be stressed that discrepancies very often emerge between the results of the different studies conducted in this field. Furthermore, it is not easy to interpret the eventual correlation of headache with depression and anxiety. To begin with, despite the opposing views of some authors such as Wolff (1), there is not yet sufficient proof that cephalalgic subjects do in fact present characteristic and constant personality traits. Then there is the question of whether or not such personality factors play a specific role in the aetiopathogenesis of headache, especially since some think that these factors may represent an effect rather than a cause of this disorder.
One of the tests most widely used in the study of adult headache patients is the Minnesota Multiphasic Personality Inventory (MMPI), which, covering many items grouped into different scales, is designed to investigate two areas of personality: neurotic and psychotic. The various studies conducted are substantially in agreement with one another in the detection of high scores on the hypochondria, depression, hysteria and psychaesthenia scales, and some authors have associated different characteristics with different headache types. While some authors (2, 3) maintain that a patient's ‘neurotic’ profile and the depressive component of his/her personality can be correlated with the duration and the intensity of the clinical picture, others (4) consider these traits to be characteristics of headache sufferers and not correlated with the duration of the symptomatology. Dieter & Swerdlow (5), on the other hand, even question the ability of the MMPI to define a complete psychological picture of headache sufferers generally.
The Children's Depression Inventory (CDI) and the Test Anxiety Inventory (TAI), devised, respectively, by Kovacs (6) and Spielberger (7), are also widely employed. These inventories are based on a series of questions to which different answers are possible—selected according to the frequency of subjects' moods. Authors generally tend to find high levels of anxiety, depression and neurotic ‘traits’ in headache sufferers (8–13). The prominence of psychological factors in the clinical profile of headache, particularly in children and adolescents, is such that these factors cannot be regarded as secondary ones within the diagnostic and therapeutic process.
We set out to evaluate the personality traits and the presence of anxiety and depression in a population of paediatric and adolescent patients referred to a Headache Centre (either for Hospitalization or as out-patients), correlating personality characteristics with headache type, headache duration and sociodemographic variables.
Subjects and methods
Fifty-seven subjects (23 males and 34 females), aged between 8 and 18 years (average age 12.43 ± 3.24 years), consecutively referred as out-patients (n = 28) or admitted as in-patients (n = 29) to the Child Neuropsychiatry Division of the University of Pavia, were enrolled in the present study. On the basis of the classification criteria proposed by the International Headache Society (IHS) (14), the sample was subdivided into three groups: (i) migraine with aura: n = 12 (five boys, seven girls; average age 14 ± 2.89 years); (ii) migraine without aura: n = 29 (11 boys, 18 girls; average age 11.58 ± 3.17 years); (iii) tension-type headache: n = 16 (seven boys, nine girls; average age 12.81 ± 3.27 years).
Our study was conducted using the following tests:
The Cattell test (15), divided into three sections (ESPQ, CPQ, HSPQ) each applicable to subjects of different ages: (i) ESPQ (Early School Personality Questionnaire). This test (16), suitable for administration to children aged 6–8 years, is divided into two parts (A1 and A2) and measures 13 dimensions of the subject's personality. The test is made up of 80 items: six items in each of the 12 personality measurement scales and eight items in the general intelligence scale; (ii) CPQ (Children's Personality Questionnaire) (17), intended for use with children aged 9–13 years. This test, totalling 280 items, is made up of Form A (divided into parts A1 and A2, each of which is composed of 70 items, five for each of the 14 personality factors) and Form B (likewise divided into two parts, B1 and B2, each containing 70 items); (iii) HSPQ (High School Personality Questionnaire) (18), for persons aged 14–18 years. The test is divided into two forms, A and B, each of which contains 140 items, 10 items for each of the 14 personality factors being investigated.
The Children's Depression Inventory (CDI), created by Kovacs in 1977 (6) on the basis of the Beck Depression Inventory for adults. This is a 27-item questionnaire conceived as a means of quantifying a wide range of depressive symptoms.
The Test Anxiety Inventory (TAI), formulated by Spielberger et al. in 1980 (7). This is a self-assessment scale, allowing individual differences in the manifestation of anxiety upon performance of the test to be measured.
All the tests listed above are based on self-assessment and all were compiled by the participants individually in the presence of an examiner who, unaware both of the aim of the study and of the type of diagnosis reached, ensured that the subjects carried out the tests properly.
We administered one of the three Cattell personality tests to all 57 members of our study group, depending on their age (six were given the ESPQ, 29 the CPQ and 22 the HSPQ).
The CDI was administered to 53 patients who were then subdivided into two age groups: 8–11 years and 12–17 years (14 and 39 subjects, respectively). The TAI was administered to 42 subjects, subdivided on the basis of their age and gender: 11–14-year-olds (n = 20; 12 males, eight females); 14–18-year-olds (n = 22; six males, 16 females).
Given the considerable time needed to administer the questionnaires in the way we chose, and the complexity of the operation, it was impossible to form a local control group large enough to render group comparisons statistically valid.
The results were thus compared with the average values for the Italian population which was used to standardize the test and comprised the following samples: ESPQ=590 subjects, CPQ = 1750 subjects, HSPQ=1189 subjects, CDI = 550 subjects, TAI 1174 subjects.
Furthermore, the scores obtained from the patients examined in each of the tests were compared with several sociodemographic variables standardized to reflect the Italian population: composition of the family unit, parents' geographical origins, social class, type of background (e.g. town, inner city), gender; and with the duration of headache (divided into three categories: 1–6 months, 7–12 months and > 13 months). In the case of the CDI and the TAI, we also assessed, with reference to each headache type, the significance of the recurrence of answers to single items.
All the data were analysed statistically using non-parametric tests, t-test,
Results
Here, we analyse the results of the Cattell personality tests which, as we have seen, apply to different age groups (Figs 1, 2 and 3). We report only the factors found on t-test, which compares the ‘normal’ averages (the standard values) with those of the patients, to be significant:

Early School Personality Questionnaire (ESPQ): mean values profile in patients with age < 9 years. Patients n = 6. Mean value 5.5 ± 2. Normal sample n = 590.
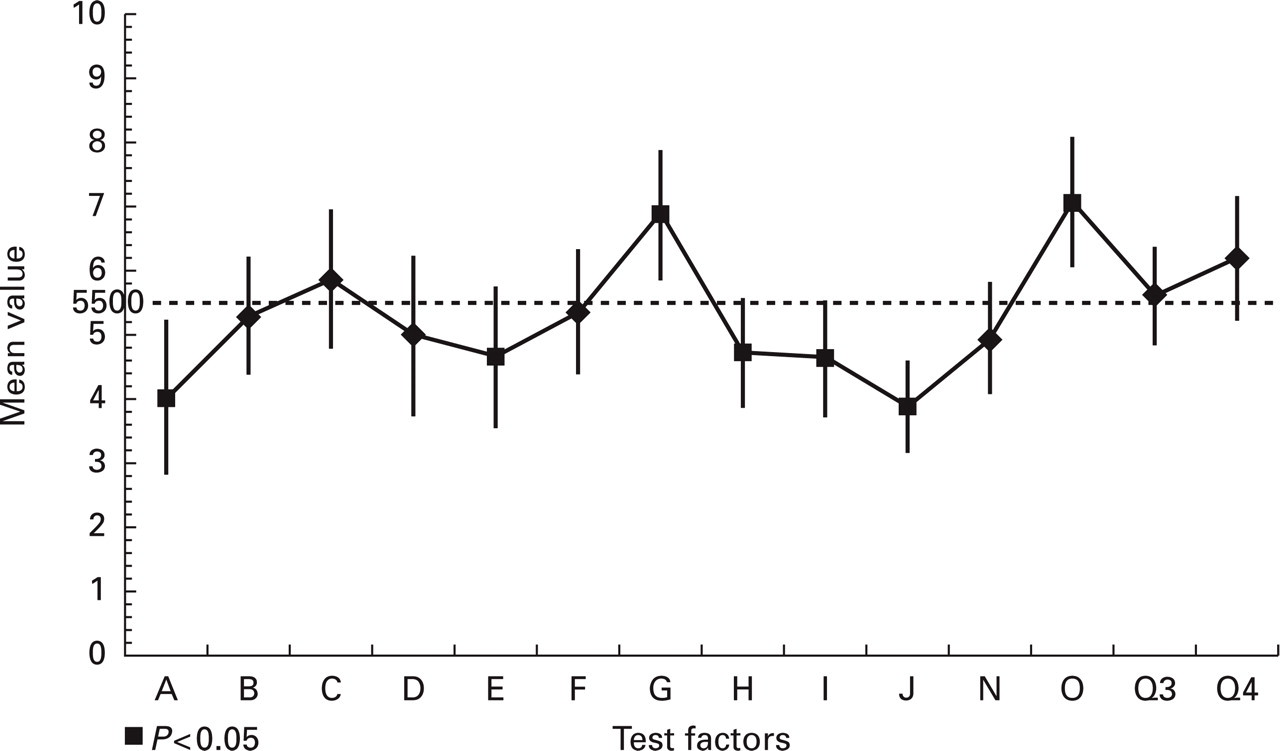
Children's Personality Questionnaire (CPQ): mean values profile in patients with age between 9 and 14 years. Patients n = 29. Mean value 5.5 ± 2. Normal sample n = 1750.
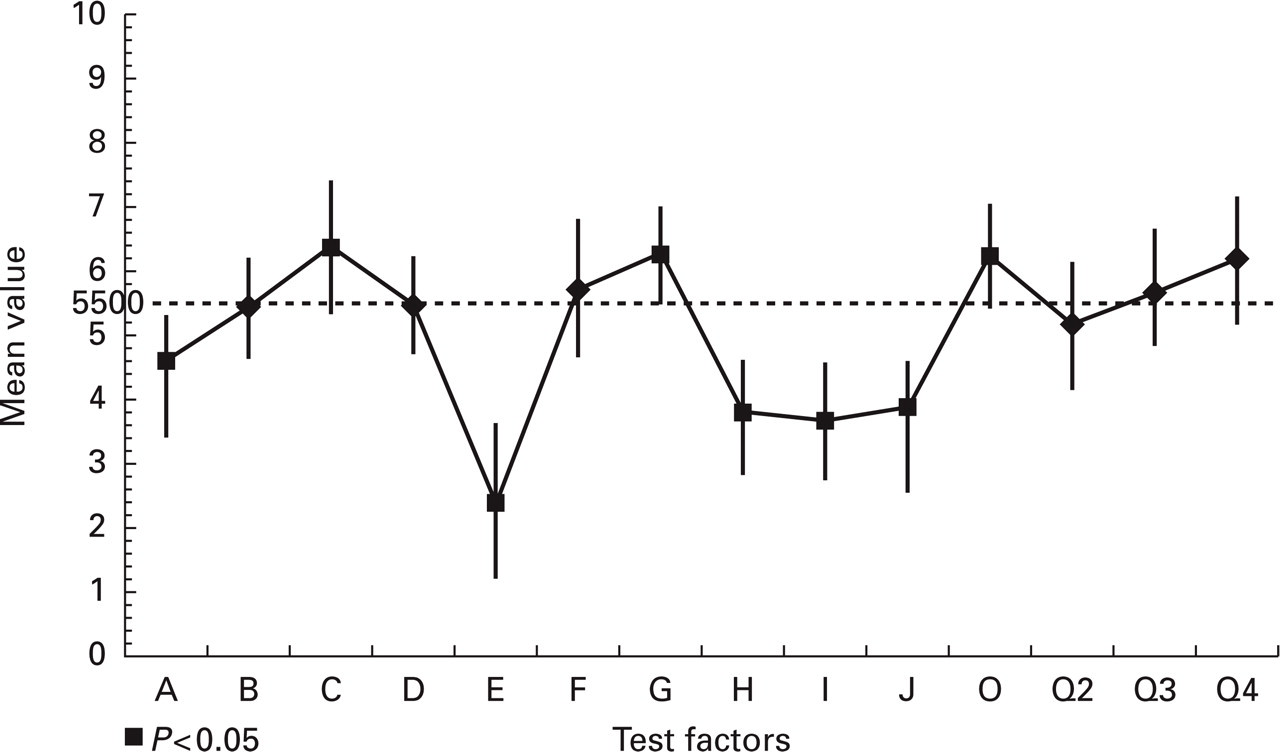
High School Personality Questionnaire (HSPQ): mean values profile in patients with age between 14 and 18 years. Patients n = 22. Mean value 5.5 ± 2. Normal sample n = 778.
Factor A: this scale ranges from ‘reservedness, aloofness’ (A−) to ‘warmth, sensitivity’ (A+). The scores obtained from the patients older than 9 years were significantly lower (P < 0.05) than normal and indicative of a rigid and detached temperament, a sort of ‘emotional flatness’.
Factor C: ranges from ‘low ego strength’ (C−) to ‘high ego strength’ (C+). Without reaching statistical significance (P > 0.05), raised factor C scores were nevertheless found in the subjects aged 6–8 years, and in those aged 8–13 years (Figs 1 and 2). In the older subjects (14–18 years; see Fig. 3) on the other hand, these scores were significantly raised, indicating a high degree of emotional self-control.
Factor E: ranges from ‘submissiveness’ (E−) to ‘assertiveness’ (E+). All the patients gave significantly low scores (P < 0.05), the average score in the 14–18 years age group being particularly low. Values corresponding to E− indicate submissiveness and lack of emotional independence, as well as a tendency to conform.
Factor G: ranges from ‘low superego strength’ (G−) to ‘high superego strength’ (G+). The G scores obtained from patients aged 9–13 years were significantly high (P < 0.05), indicating a marked adherence to moral values and regulations, and a clear sense of duty and responsibility.
Factor H: ranges from ‘susceptibility to threat, timidity, withdrawal’ (H−) to ‘venturesomeness, bold equanimity, non-susceptibility to threat’ (H+). The scores obtained from the subjects older than 9 years were significantly low (P < 0.05). H− subjects are, typically, reserved individuals who respect rules and exist in a state of repression.
Factor I: ranges from ‘decisiveness, realism’ (I−) to ‘tender-mindedness’ (I+). With reference to factor I, our subjects (in all the three age groups taken into consideration) gave markedly low scores (P < 0.05), indicative of a marked pragmatism and lack of imagination.
Factor J: ‘lack of rigid superego’ (J−) as opposed to ‘individualistic, uncooperative behaviour’ (J+). All our patients tended to give low scores, with those obtained from the subjects in the 9–13 years age groups reaching statistical significance (P < 0.01), indicating an inclination to aggregate with a group and to ‘move with the tide’.
Factor N: ranges from ‘naiveté’ (N−) to ‘shrewdness’ (N+). This factor is examined only in the ESPQ and CPQ. The subjects aged 6–8 years gave significantly low scores (P < 0.001), reflecting their faith in human nature, and their spontaneity and sincerity. The scores obtained from the other subjects were in line with average values.
Factor O: ranges from ‘low guilt proneness’ (O−) to ‘high guilt proneness’ (O+). Significantly high factor O values were recorded in the 6–9 years group of headache patients (P < 0.05). Our subjects therefore displayed low self-esteem and a tendency to feel guilty.
The influence of migraine was analysed using χ2. For this purpose the patients were subdivided according to the three diagnoses (migraine with aura, migraine without aura, tension-type headache) and the scores were grouped into three categories (low: 1, 2, 3; normal: 4, 5, 6, 7; high: 8, 9, 10). The 3 × 3 χ2 test gave the following results.
Patients with migraine with aura had low scores more frequently than expected (P < 0.001) in factor B (B−: poor capacity for dealing with abstract problems) and high scores (P < 0.01) in factor C (C+: high ego strength). Other factors do not seem to be sensitive to the diagnosis.
The answers to the CDI were analysed using three statistical tests. A t-test compared the scores of the patients divided by age with those of the standard samples (see Fig. 4). Both the age groups had higher score values (P < 0.05). An

Children's Depression Inventory (CDI): mean values and standard deviation (SD).
Looking at the recurrence of individual answers to the various items, through a χ2 test the answer ‘I always have to force myself to do my homework’ was given more frequently (P < 0.0001) by migraine with aura patients.
Finally, the same three statistical tests were applied to the answers to the TAI. TAI was administered to 42 patients aged between 11 and 18 years. Only the older subjects (15–18 years old), as shown in Fig. 5, gave significantly raised scores, both males (P < 0.001) and females (P < 0.01) indicating a greater tendency to manifest anxiety over the test. Furthermore, the χ2 test revealed that the frequency of high scores given by migraine with aura patients was, in relation to the migraine without aura and tension-type headache patients, significantly higher than expected (P < 0.05).

Test Anxiety Inventory (TAI): mean values and standard deviation (SD) in patients with age between 15 and 18 years.
The migraine with aura patients and the tension-type headache patients gave, with significant frequency, the following answers: ‘I often/nearly always freeze up when taking important examinations’ (P < 0.005).
The comparison of the various personality factors with the sociodemographic variables did not prove significant.
No significant correlation with headache duration emerged in any of the tests used. Neither did any difference emerge when comparing the Hospitalized patients with those seen as out-patients.
Discussion
The literature on personality characteristics and headache still presents considerable discrepancies, as regards both the eventual pathogenic role of personality characteristics, and the possible association between certain personality traits and different headache types.
As far as paediatric and adolescent patients are concerned, there is also disagreement over whether or not the picture of emotional disturbance in these subjects is related to the different age groups, to gender, or to the characteristics of the family unit.
On the basis of the Cattell tests, the subjects involved in our study were found to have several characteristics. The first finding is the low factor A score, indicating a certain emotional flatness and ‘rigidity’ in our subjects, who feel inhibited in situations characterized by emotional intensity, especially of an aggressive nature.
These characteristics are in accordance with the reports in the literature: indeed, Furmanski, as early as 1952 (19), described headache as a ‘vegetative’ neurosis (in other words, as a manifestation of suppressed or repressed aggression). According to Blaszczynski (9), the central conflict in a cephalalgic subject arises from his/her feelings of hostility, especially towards family members, which in reality hide a sense of fragility and a desire to be emotionally dependent on them. Passchier (20, 21) and Blaszczynski (9) have both highlighted the ‘rigidity’ of cephalalgic subjects, as well as their difficulty in expressing feelings of anger and resentment. Lanzi et al. (22) identified ambivalence over these feelings of hostility as the central conflict in migraineurs.
This finding, taken as a starting point, was confirmed by our patients' low factor E scores, indicating submissiveness and dependence, as well as conformist tendencies (factor E being the dominance factor studied by Maslow (23) and by Allport (24)). It must be pointed out that the older subjects (aged 14–18 years) tended to give lower scores.
Conformity with accepted social behaviour is indicative of a personality with little creative capacity, which in the view of other authors (25) seems to be hidden behind an outward appearance, a striving for originality, which would seem to suggest the complete opposite. The inability of cephalalgic subjects to enter into the affective sphere of life and their impotence in the face of environmental stimuli (26) are indicative of the difficulty they experience in interacting with others; this leads to a passive adaptability to environmental changes (27).
When we analysed the Cattell test profiles relating to our sample, we noted that the younger subjects (under 9 years old) and the adolescent patients give scores which are more disharmonious than those given by the rest of the sample. This fact may be seen as confirmation that certain personality traits are peculiar to cephalalgic subjects, emerging early on, tending to become ‘flattened’ in a latent period (preadolescence), and subsequently re-emerging more predominantly in adolescence.
Further support for the data reported so far is provided by the low factor H scores recorded in our sample (which are indicative of those facets of personality based on poor emotional resources and on the sense of inhibition experienced in situations characterized by emotional intensity, especially if this is of an aggressive nature). It is, according to the test's creators, essentially a ‘constitutional’ factor.
With regard to factor I, there is a connection between this factor and the previous ones. On the negative side (I−), this factor indicates realism and solidity and is one determined by environmental and cultural influences, as well as by a certain tendency inherent in the personality.
I+ individuals tend to come from indulgent and liberal families, and I− subjects from demanding and hyperprotective families. The I− factor is usually associated with low A–D–E factor scores, and together these can be taken to indicate the prevalence of pragmatic thought processing and a certain lack of imagination.
The two extremes of factor C are ‘low ego strength’ (C−) and ‘high ego strength’ (C+). In our headache population, the scores obtained from those under 9 years old and those in the 9–13 age group did not differ significantly from normal values, while a significantly positive trend (P < 0.05) emerged in the group of subjects over the age of 14 years. This also proved to be a discriminating factor between the different headache types. The scores obtained from the migraine with aura patients were, especially in relation to the migraine without aura patients, significantly higher than expected (P < 0.05). This suggests that a high degree of somatization occurring in migraine with aura may be correlated with increased emotional stability. This finding corresponds to other reports in the literature (28–30).
Other authors maintain that, in relation to migraine without aura or tension-type headache patients, subjects with migraine with aura show a higher prevalence of associated psychiatric disorders (especially depression, anxiety and forms of compulsive obsessive behaviour) (31–33).
The two extremes of factor G are ‘low superego strength’ (G−) and ‘high superego strength’ (G+). Irrespective of their age, all the subjects included in our study gave high G factor scores. This result, as far as Cattell is concerned, can be seen as ‘empirical confirmation’ of the definition of the superego current in the field of psychoanalysis. This result is in accordance with the findings of Blaszczynski (9) and of Passchier (20), who suggested that headache patients are subject to aggressive feelings, which are checked by a rigid and regulatory superego.
The Cattell test includes two factors correlated with these aspects: factor O (tendency to feel guilty) and factor Q4 (high level of ergic tension, anxiety). As regards the first of these, all our subjects gave high scores (O+) which were statistically significant, irrespective of age. This factor, initially described as a ‘depressive tendency’ and ‘low self-esteem’, is positively correlated with factor G+, and both feature in neurotic personality profiles.
Finally, let us consider factor B, a scale which considers low intelligence (B−) as opposed to high intelligence (B+) and measures mental capacity in general, and more specifically, an individual's intuitive capacity and ability to deal with abstract problems. High B scores are, in part, correlated with good adaptive capacity and school performance.
Overall, our subjects were found to demonstrate good mental capacity, which reflects data published in the literature relating to the cognitive performances of headache sufferers (31, 32).
One aspect of factor B is worthy of further consideration here: while remaining within the normal range, the scores given by our migraine with aura patients on this scale were significantly lower than expected. Furthermore, the main concerns of these subjects, as revealed by TAI, were their school performance and their difficulty in applying themselves in some areas.
The results of the CDI highlighted the presence of depressive components in the subjects who underwent this test. Many authors have drawn attention to a strong association between headache and severe depression in adults (33, 34), and the possibility of a cross-reaction between the two pathologies has even been hypothesized (33). An association between headache and depression has also been highlighted in childhood and adolescence (25, 34–36). Some authors (37), using the CDI, have obtained results which reflect those emerging in our study.
If we consider the items individually, migraine with aura patients tend to highlight problems indirectly related to feelings of depression (difficulty with school work). This supports our earlier observation that migraine with aura patients have less introspective capacity and are less able to process conflicts on a mental level. In short, they adapt better to the demands of the environment and this, in turn, produces an apparently greater stability of their ego. The problems relating to this tendency may include inhibition of their intellectual processes and difficulty at school.
In conclusion, even though our age-dependent findings were more specific, our study nevertheless reveals that cephalalgic subjects do show common personality traits. In accordance with recent findings, certain traits, particularly depressive and anxiety-linked ones, tend to be more prevalent in migraine than in tension-type headache sufferers. Furthermore, contrary to that reported by other authors (26, 38), the lack of correlation with sociodemographic variables and with headache duration suggests that the personality traits detected in our sample can indeed be considered features peculiar to cephalalgic subjects.
Footnotes
Acknowledgements
We gratefully acknowledge Catherine Wrenn for the translation.