
Abstract
Our purpose was to examine the association between personality traits, depression and migraine in the long term. In 56 women with migraine a psychological assessment was carried out to assess the presence of major depression, and the Minnesota Multiphasic Personality Inventory (MMPI) and the State and Trait Anxiety Inventory (STAI) were administered at baseline (T0) and after 6-7 years (T2). Frequency, severity and duration of migraine were recorded at T0, after treatment (T1) and at T2, and their relation to the prevalence of depression and to the MMPI and STAI data was examined (ANOVA, Student's t-test, X 2 analysis, and multiple regression analysis). Pain parameters improved in all patients in T0-T1, but at T2 were higher in patients with depression at T0. The patients whose migraine improved at T2 had, at T0 and T2, significantly lower MMPI and STAI scores. Multiple regression analysis showed a correlation of the MMPI depression score and STAI 1,2 scores at T0 with headache frequency at T2. We conclude that the co-occurrence of migraine, personality changes and depression in women does not appear to influence the results of treatment at short-term, but it seems to be influential on headache history in the long term.
Introduction
Several studies have been performed to explore the association between personality traits, depression and migraine; however, the mechanisms that link these variables and the natural history of their co-occurrence remains controversial.
Personality traits in migraine patients were assessed by several authors by means of the Minnesota Multiphasic Personality Inventory (MMPI) (1–10). Some of them found normal profiles or, at least, a lower scale elevation than in patients with chronic tension-type headache or with migraine and tension-type headache superimposed (1, 4), while others found that some scales were elevated, and, in women, a typical ‘V configuration’ of the neurotic triad (with elevation of hypochondria and hysteria, and depression being somewhat lower) (5, 6).
Other authors investigated the association between migraine and psychiatric disorders (11–24). In epidemiological studies an association was observed between migraine and depression (11, 14, 16, 18, 20, 21, 23). This was confirmed by prospective studies (15, 22). Breslau et al. (22) performed a longitudinal study on a random sample of 1007 young adults to estimate the relative risk for major depression associated with prior migraine and the relative risk for migraine associated with prior major depression. They concluded that the previously observed cross-sectional association between migraine and major depression can result from bidirectional influences, with each disorder increasing the risk for first onset of the other.
A further question is whether distinctive personality profiles or the presence of depression before treatment might predict treatment outcome. Some authors (3) found that, in headache patients, an elevation of the MMPI depression and social introversion scales correlated positively with the biofeedback treatment outcome. Other authors concluded that MMPI findings before treatment have no prognostic value of treatment outcome in patients with migraine (5, 9). However, these investigations were conducted after relatively short follow-up periods.
The purpose of this study was to examine the association between personality traits and depression in women with migraine and the evolution of pain pathology in the long term.
Methods
Eighty-two women with migraine with aura (n = 6) or migraine without aura (n = 76) (mean age ± SD 37.07 ± 11.69 years) consecutively sent in 1993 to the Headache and Facial Pain Unit, Department for Clinical Pathophysiology, University of Turin, were enrolled. The diagnoses were made according to the guidelines of the International Headache Society (25). Inclusion criterion was the presence of migraine for at least 1 year; exclusion criteria were the presence of drug abuse or of a concurrent relevant medical condition, such as endocrine, immune, blood, nervous or circulatory disorders.
Every patient underwent a systematic record of medical history and a general and neurological examination. In the history, a record was taken of the headache characteristics, improvement or aggravating factors and associated symptoms. The same senior neurologist examined the patients and carried out a psychological assessment on the Axis 1 (Anxiety-, Mood- and Somatoform-Disorders) of the DSM-III-R with a structured interview (26). The presence of major depression was evaluated according to the criteria of the DSM-III-R, which defines this disorder as a condition characterized by the presence of at least five from a list of nine depressive symptoms occurring within the same 2-week period, with at least one of the symptoms pertaining to a depressed mood or loss of interest or pleasure. The following symptom groups are listed in the DSM-III-R definition of major depression: depressed mood, loss of interest or pleasure, weight loss or weight gain, insomnia or hypersomnia, psychomotor agitation or retardation, fatigue, feelings of worthlessness or excessive guilt, concentration problems, suicidal ideations or attempts,
All patients were given a diary in which to record, on a daily basis, occurrence, severity (score 1–5), and duration of the headache episodes. The Italian MMPI and the State and Trait Anxiety Inventory (STAI, X1,2 Italian version) were then administered to all patients. After 1 month (T0), during which the patients were asked to refrain from taking drugs as much as possible, treatment was performed for a period ranging between 2 and 6 months. At the end of treatment (T1) the data relative to the pain parameters were further collected through the pain diaries for 3 months. At this time, if improvement was significant and steady, the patients were instructed to reduce or suspend drug intake. The patients were re-examined after a period ranging between 6 and 7 years (T2). A psychological assessment was carried out again according to the DSM-IV, whose criteria for major depression are the same as in the DSM-III-R, and the MMPI-2, STAI Y1,2 were administered. If headache was still present, the patients were given the headache diary for 3 months. Twenty-two patients could not be retrieved, one was deceased and three refused to continue the programme, leaving a total of 56 patients (68.3%) who completed the study.
Two criteria were employed to assess the patients: presence or absence of major depression at baseline (T0), and improvement or no improvement of migraine at T2. Improved patients were those in whom pain parameters at T2 were lower, with a reduction of the headache frequency of at least 50%. Pain parameters in the three periods considered and MMPI and STAI data at T0 and T2 were examined statistically according to these two criteria (
Results
Data relative to patient age and pain of the patients who concluded the study and of the dropouts are reported in Table 1. There was no significant difference between the two categories.
Data relative to age and headache attacks of continued patients and dropouts

There is no statistically significant difference (Student's t-test).
At T0, 31 patients (55.4%) had major depression and 25 had not (44.6%). Of the dropouts, 14 (54%) had depression and 12 (46%) had not. The two groups had no significant difference in age or in the time elapsed since the onset of migraine. The pain parameters in the three periods considered are shown in Table 2 and Fig. 1. All parameters improved significantly in both groups from T0 to T1. In the not depressed group they improved further at T2, although not significantly so. In the depressed group pain parameters worsened again at T2, significantly for severity. There was no significant intergroup difference at T0 and T1, while at T2 frequency and severity of headache attacks were significantly higher in the patients who had major depression at T0 (Table 2).
Mean values (± SD) of the pain parameters in the three periods considered in patients with depression (D) and without depression (ND) at baseline (T0)


Pain parameters at baseline (T0), after treatment (T1), and after 6–7 years (T2) of the patients with depression (n = 31) and without depression (n = 25) at T0. □, Not depressed; ▪, depressed.
At T2, 32 patients had improved and 24 patients had not. The two groups had at T0 similar pain parameters (Table 3 and Fig. 2). In the group improved at T2 pain parameters improved significantly from T0 to T1 and further improved from T1 and T2, although not significantly so. In the group not improved at T2 there was a significant improvement of all pain parameters from T0 and T1, while at T2 the scores worsened again. There was no intergroup significant difference in the pain parameters at T0 and T1, while at T2 the difference was highly significant for frequency and severity of the headache attacks (Table 3). At T0 major depression was present in 37.5% of the patients improved at T2, and in 79.1% of those not improved; at T2 12.4% of the improved patients and 45.8% of the not improved patients had major depression. In both cases the difference was significant (Tables 4 and 5). Treatment modalities were essentially the same in the two groups, except for antidepressants that were more frequently prescribed in the unimproved group (Table 6).
Mean values (± SD) of the pain parameters in the three periods considered in patients improved (I) and not improved (NI) at T2

Prevalence of major depression at baseline in patients improved (I) and not improved (NI) at T2

The prevalence was significantly lower in the improved patients (P < 0.01, χ2 analysis).
Prevalence of major depression at T2 in patients improved (I) and not improved (NI) at T2

The prevalence was significantly lower in the improved patients (P < 0.01, χ2 analysis).
Percent frequency of drug prescription at T0 of improved (I) and not improved (NI) patients

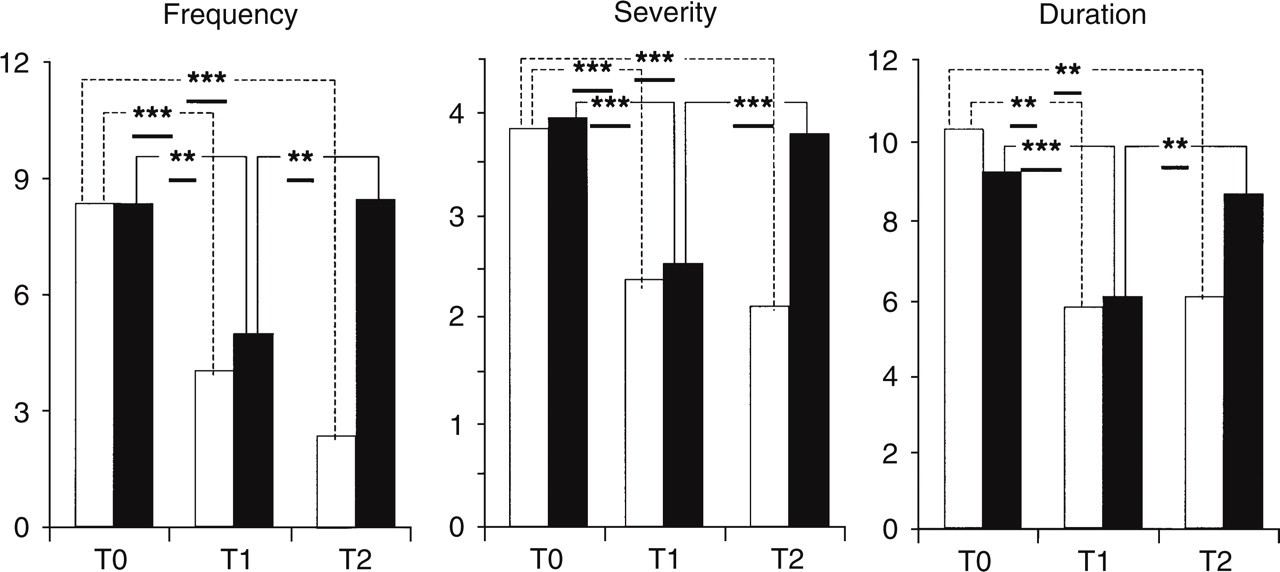
Pain parameters of the patients improved (□, n = 32) and not improved (▪, n = 24) at T2.
In the patients improved at T2 all MMPI scales (except hypomania) and STAI scores were lower at T0 than those of the not improved patients: this was significant for depression, psychopathic deviation, paranoia, psychasthenia, schizophrenia and social introversion. In these patients hypochondria and hysteria scored highest and a tendency to a ‘V configuration’ (so-called ‘conversive V’) of the three scales of the neurotic triad (hypochondria, depression and hysteria) was observed. In the patients not improved at T2, depression had the highest score (Fig. 3).

MMPI and STAI at baseline (T0) of the patients improved (□) and not improved (▪) at T2.
At T2 all MMPI scales (except hypomania), and STAI scores were significantly lower in the improved patients. In these patients the MMPI scales were within the normal range; however, the tendency to a ‘V configuration’ of the neurotic triad was even more pronounced than at T 0 (Fig. 4).

MMPI and STAI at T2 of the patients improved (□) and not improved (▪) at T2.
After multiple regression analysis, headache frequency at T2 correlated with the MMPI depression score and with STAI 1, 2 scores at T0 (P < 0.05 in all cases).
Discussion
Two reasons suggested limiting our investigation to female patients. The first was that, in our files, women patients were overwhelmingly more frequent: this is due to a higher prevalence of migraine in women, but may also be partially related to a higher tendency of women to seek treatment in a specialty centre. The second reason was related to the different significance that the MMPI data may have between males and females.
The relatively limited number of patients suggests caution in interpreting the data; however, the results at hand seem to confirm the co-occurrence of chronic migraine, personality changes and depression, and that these conditions may reciprocally influence each other.
The majority of our patients who still suffered from frequent migraine attacks 6 or 7 years after the first examination had consistent elevations of MMPI and STAI scales and a high prevalence of major depression. These findings are in agreement with previous studies, where the MMPI was applied to patients suffering from chronic daily headache (27). In the majority of these patients an ‘emotionally overwhelmed’ profile (with elevation of depression and of several other scales), or a conversive profile (with elevation of hypochondria and hysteria, depression being somewhat lower) were found. After treatment, a score decrease of many scales was observed. However, patients with a conversive V configuration before treatment still showed this configuration after treatment, though at a lower level, while several patients with a depressive MMPI profile showed a conversive V after treatment (27). In the present study a V configuration, at normal score level, was indeed observed in the patients improved at T2 (Fig. 4). Holm et al. (28), after administering the Beck Depression Inventory (BDI) in recurrent headache sufferers, found consistent relationships between the somatic symptoms and headache activity, but not between the cognitive/affective items and headache activity. The authors suggest that the somatic items in these patients may be related to pain rather than to depression. Since several somatic items are used to construct the first three MMPI scales, the V configuration in our patients might reflect pain-related symptoms rather than personality characteristics. However, the fact that this configuration was observed in the improved patients and not in the unimproved (Fig. 4) also suggests that hysterical traits may be typical of a number of migraine patients and may be unmasked after treatment.
In their study on a sample of young adults, Breslau et al. (22) found in females at age 33 a cumulative incidence of 25.9% of migraine and of 27.87% of major depression. The high prevalence of major depression we found at T0 may be explained by the fact that most of our patients were women seeking treatment for a severe type of migraine they had been suffering from for many years (Table 1). While the presence of major depression at T0 does not seem to be a factor conditioning the response to treatment in the short term, it does seem to influence the history of the pain pathology over a long period of time (Table 2 and Fig. 1). Moreover, when the headache frequency at T2 was taken as a discriminative factor, the not improved patients were found to have a significantly higher prevalence of major depression both at T0 and at T2 (Tables 4 and 5). Moreover, these patients had at T0 and T2 significantly higher scores of several MMPI scales, and depression in particular (Fig. 3). This was again independent of the pain characteristics at T0: in fact, at this time all pain parameters did not differ significantly between improved and not improved patients at T2 (Table 3 and Fig. 2).
In conclusion, while the data at T2 might suggest a causal relationship between pain frequency and severity and depression in migraine patients, a comparative analysis of the data in the three periods considered seems to indicate that such a relationship is bi-directional. The co-occurrence of depression and personality changes in women with migraine does not appear to influence the results of treatment in the short term, but it seems to be influential on headache history in the long term.