
Abstract
The objective of the study was to assess whether a family history of vascular disorders is more common in children and adolescents with migraine than in the general population. Family history of stroke, arterial hypertension, myocardial infarction and diabetes was investigated by history taking in relatives of ambulatory children and young adults with migraine and in a control group. The odds ratios (ORs) with 95% confidence intervals (95% CI) were used as a risk measure. Using univariate and multivariate (logistic regression) analysis, family history was assessed in the whole sample and in subgroups by sex and age, degree of relationship (parents and grandparents vs. relatives), disease type (migraine with and without aura), and type of vascular disorder. The sample included 143 cases (migraine with aura 35, migraine without aura 108) and 164 controls aged 324 years (mean 12 ± 3.8 years). Patients with migraine were at increased risk of vascular disorders in parents and grandparents but not in all relatives. Multivariate analysis indicated family history of stroke as most common only in boys. In conclusion, our study provides some clues to the assumption that migraine and vascular disorders have common pathogenic mechanisms and that genetic susceptibility plays a role in increasing the risk of migraine in the offspring of families with one or more cerebrovascular or cardiovascular conditions.
Introduction
The relationship between migraine and vascular disorders in adults has been repeatedly investigated. The cardiovascular risk profile of patients with migraine has been found to be comparable to that of the general population, if arterial hypertension is excluded (1, 2). By contrast, there is a body of evidence supporting a correlation between migraine and stroke. First, migraine itself may present with stroke-like episodes or may even be an underlying cause of stroke, as shown in patients with migrainous infarction (3, 4). Second, epidemiological studies have consistently shown that migraine is a risk factor for stroke (5–12). Migraine with aura (MA), in particular, has been shown to be an independent risk factor for stroke, especially in young women (5). A strong correlation between migraine and stroke has, after making adjustments for oral contraceptive use, smoking and the presence of anti-cardiolipin antibodies (9), been found in women under 35 years of age. Third, migraine and stroke are typical manifestations of some genetic disorders, including cerebral autosomal dominant arteriopathy with subcortical infarctions and leucoencephalopathy (CADASIL) (13) and mitochondrial encephalopathy with lactic acidosis and stroke-like episodes (MELAS) (14).
What is less clear, however, is whether all migraine varieties are associated with stroke or whether the association is restricted to MA (9, 10). Moreover, there is still no convincing evidence concerning the mechanisms that would be implicated (in particular, the role of vascular genetic factors) or the groups of migraineurs really at risk of ischaemic stroke (15–17). In addition, virtually no studies have been carried out to investigate the association between migraine and stroke in children and adolescents. Finally, there are no published reports on the genetic susceptibility to vascular disorders of patients with migraine compared with the general population. For these reasons, we performed a case–control study to investigate the presence of selected conditions – acute vascular disorders (stroke, myocardial infarction) and/or selected risk factors for cerebrovascular and cardiovascular disorders (arterial hypertension, diabetes) – in the families of children, adolescents and young adults with migraine and in the families of a control population.
Methods
The study was conducted at the Department of Child Neurology and Psychiatry of the University of Pavia. The cases were patients with newly diagnosed migraine, with or without aura, consecutively admitted to our out-patient unit during the period November 2000 to December 2001. Migraine was diagnosed in accordance with the International Headache Society criteria, modified for paediatric patients (18–22). The control group was made up of patients with a variety of clinical conditions, including psychiatric disorders, epilepsy, and specific language and/or learning disorders.
All patients with migraine received a careful clinical assessment and, if indicated, a neuroradiological investigation (computed tomography or magnetic resonance imaging) to exclude secondary headache. The controls were assessed to exclude migraine in their personal history.
Both parents of the cases and the controls were interviewed in person and, after giving their informed consent to the study, were administered a semistructured questionnaire designed to collect relevant demographic data and to record the presence, in any first-degree and second-degree relatives, of any of the conditions under consideration (stroke, myocardial infarction, arterial hypertension, diabetes). For each condition, the interviewee was required to give the answer ‘Yes’, ‘No’ or ‘Don’t know’. To prevent heterogeneity of answers due to misinterpretation of differently formulated questions, the interviewer (I.A.) always phrased the questions in exactly the same way. To increase the validity and reliability of the answers, each condition was given a practical definition. Stroke was defined as the occurrence of acute focal neurological dysfunction persisting for ≥ 24 h and requiring hospitalization. Myocardial infarction was defined as the presence of chest pain requiring hospital admission. The presence of arterial hypertension and diabetes was established on the basis of the use of specific treatments and, where known, the need for regular blood pressure and blood sugar monitoring.
Family history of stroke, myocardial infarction, arterial hypertension and diabetes (the conditions) was defined as the presence of at least one affected member among all first-degree and second-degree relatives. To provide more conservative estimates of the prevalence of the four conditions, the answers ‘No’ and ‘Don’t know’ were pooled. Several subgroup analyses were performed to assess family history of the conditions in parents and grandparents, family history of each condition considered separately, the number of affected parents and grandparents, the family history of the conditions in MA and migraine without aura (MO) patients considered separately, and family history of the conditions in males and females considered separately. Data were analysed using the statistical package SPSS for PC. Risks were expressed as odds ratios (ORs) with 95% confidence intervals (95% CIs). Univariate analysis (using χ2 for categorical variables and Student's t-test for continuous variables) and multivariate (logistic regression) analysis were performed as appropriate.
Results
The study population was made up of 143 cases and 164 controls aged 3–24 years (mean 12 ± 3.8 years). The cases included 108 patients with MO and 35 patients with MA.
The controls were affected mostly by psychiatric disorders (n = 85), epilepsy (n = 52) and language disorders (n = 14). The general characteristics of the sample are outlined in Table 1. The migraine patients (mean age 12.5 ± 3.1 years) were older than the controls (mean age 11.5 ± 4.2 years) (t = 2.3; P < 0.05) and there was a slight (non-significant) predominance of females in the control group.
General characteristics of the sample

∗The controls were affected by: psychiatric disorders (n = 85); epilepsy (n = 52); language disorders (n = 14); neuromuscular disorders (n = 7); learning disabilities (n = 3); cerebral palsy (n = 3).
†χ2 for trend 11.4; P < 0.005.
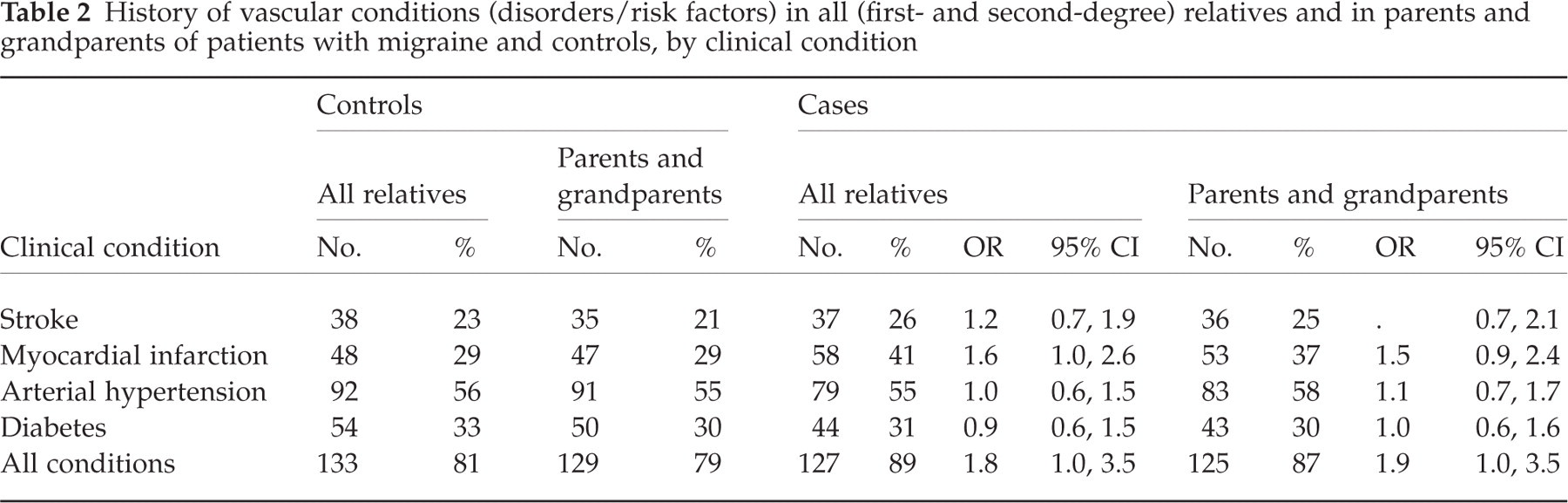
One hundred and twenty-seven cases (89%) and 133 controls (81%) reported vascular or related conditions (stroke, myocardial infarction, arterial hypertension, diabetes) in their families. These conditions were more prevalent in the families of the patients with migraine than in those of the controls when all conditions were included (OR 1.8; 95% CI 1.0, 3.5) (P < 0.05) and when the analysis was restricted to the parents and grandparents (OR 1.9; 95% CI 1.0, 3.5) (P < 0.05). With the exception of myocardial infarction, which constituted a risk factor of borderline statistical significance, the distribution of each condition was similar in the families of both cases and controls (Table 2). The number of affected relatives tended to increase significantly among the cases (Table 3). The OR of having one first- or second-degree relative with a vascular or related condition was 1.7, while the risk of having two to four, or five or more, affected relatives rose to 1.9 and 3.2, respectively. The corresponding ORs considering only parents and grandparents relatives were 1.4, 1.6, and 2.5.
History of vascular conditions (disorders/risk factors) in all (first- and second-degree) relatives and in parents and grandparents of patients with migraine and controls, by clinical condition
Number of affected relatives with vascular conditions (disorders/risk factors) in patients with migraine and controls

∗χ2 for trend 5.7; P < 0.02.
†χ2 for trend 4.4; P < 0.05.
Subgroup analyses showed a family history of stroke to be most common among the parents and grandparents of male patients with migraine (31% vs. 20%; χ2 4.0; P < 0.05; OR 2.1; 95% CI 1.0, 4.4). None of the other conditions presented a significant OR distribution. No differences were found when assessing MA and MO separately. Multivariate analysis confirmed that, following adjustments for age, sex, and interactions between sex and the conditions, a family history of acute vascular disorders and risk factors for cerebrovascular and cardiovascular disorders is more common among all relatives (OR 2.5; 95% CI 1.2, 5.1) and among parents and grandparents of patients with migraine (OR 2.6; 95% CI 1.3, 5.1).
Discussion
Our study showed that the families of children, adolescents and young adults with migraine are at higher risk of acute vascular disorders and risk factors for cerebrovascular and cardiovascular disorders than the general population. The association between family history of vascular risk factors and migraine seems to be fairly strong and consistent, as shown by the number of affected relatives and by the increase of the risk when confounding variables and interactions are controlled by multivariate analysis. However, the clinical significance of the association is at best modest, if we consider each condition separately and we focus on parents and grandparents, for whom the information is more reliable (Table 2). The increased risk of myocardial infarction in the relatives of patients with migraine is worth noting and has been documented in the elderly (12). However, the possibility of a chance finding cannot be excluded here, given the high number of comparisons and the loss of statistical significance in the multivariate analysis models. By contrast, the increased risk of stroke in the families of male patients with migraine seems more significant, since it persisted when multivariate analysis was performed only in males and since an interaction was found between sex and the four conditions under consideration (data not shown). Although this latter finding is partly in keeping with other reports showing an association between migraine and stroke and the role of family history as a risk factor for both conditions (23–25), the excess risk shown in males is not easy to explain and requires confirmation.
Our study has several limitations. First, the cases and controls were not age- or sex-matched. The migraine patients were slightly older than the controls. However, this difference is not likely to have affected significantly the quality and completeness of the data obtained through interview, as the accuracy of the answers regarding parents and grandparents is unaffected by patient age and there is no reason to think that the number of second-degree family members might be significantly different in cases and controls. Second, the small size of the sample might explain the lack of statistically significant findings when each clinical condition was assessed separately, even in the presence of similar trends. However, this study is a pilot investigation and a confirmatory survey on a larger study population is required. Third, we did not calculate the size of the family of each case and control. One might speculate that the cases had, overall, more relatives than the controls, thus increasing the probability of finding affected individuals. This assumption may be true for second-degree relatives, but does not explain the higher risk of acute vascular disorders and risk factors for cerebrovascular and cardiovascular disorders among parents and grandparents. Fourth, the definitions used to identify the conditions under consideration could be disputed, as their validity and reliability are currently unknown. However, this bias is likely to affect cases and controls to the same extent. Recall bias can also be excluded in this study, since our population was made up of newly diagnosed individuals, not old referrals.
Our study also provides some clues with regard to the assumption that migraine and vascular disorders/risk factors have common pathogenic mechanisms and that genetic susceptibility plays a role in increasing the risk of migraine in the offspring of families with one or more cerebrovascular or cardiovascular condition. Given the complex and largely unknown mechanisms underlying the pathophysiology of migraine, one cannot, in a clinical series like ours, exclude the involvement of different biological factors. Current theories indicate that changes in the blood vessels within pain-producing intracranial meningeal structures may constitute the primary dysfunction in migraine. Abnormalities of haemostasis (platelets, anti-phospholipid antibodies and congenital thrombophilia) leading to an increased thrombotic risk have been suggested (26). Altered platelet aggregation or coagulation in genetically susceptible individuals can be thus postulated to explain the correlation between migraine and vascular disorders/risk factors. However, no unequivocal experimental findings are as yet available to support this hypothesis (27–29).
Our study may be interesting from the perspective of the so-called ‘phenotypical heterochronia’ of migraine (a term denoting the fact that the clinical expression of the disease and its association with other clinical disorders tend to vary with age and over time) (30). From this perspective, the increased vascular risk in the families of patients with migraine may reflect a changing age-related phenotype of common genetic origin.
Greater insight into these as yet unknown mechanisms might be obtained after a more careful assessment of each condition and its interaction with sex and age.
In view of the above speculations, this study is to be followed by a larger survey in which additional risk factors (e.g. atrial fibrillation) and confounding variables (oral contraceptives, smoking) will be investigated and tension-type headache will also be assessed to verify the specificity of the association between migraine and vascular co-morbidity.
Footnotes
Acknowledgements
The study was supported by a grant from the Fondazione Pierfranco e Luisa Mariani ONLUS (Milan) and Italian Ministry of Health. The study was, in part, presented at the 6th Headache Congress of the European Headache Federation, Istanbul, 26–30 June 2002 (Termine C, Rossi M, Ferrari Ginevra O, D’Arrigo S, Amica I, Beghi E et al. Cephalalgia 2002; 22 (Suppl. 1):12).