
Abstract

Oral contraceptives (OCs) and hormone replacement therapy (HRT) are popular efficacious therapies that are widely used. Soon after OCs were introduced however, they were found to be associated with an increased risk of venous and arterial thrombosis. Consequently, women with a history of thrombosis have been excluded from various contraceptive trials. HRT was shown to have a protective cardiovascular effect, with no increased risk of venous thromboembolism being shown until 1996, when independent studies demonstrated that some formulations might cause thrombosis. HRT may modify coagulation and fibrinolysis and this may play a part in thrombosis. In this study we will review the modifications of haemostasis that are associated with venous and arterial thromboses. Then we will focus on thrombosis and haemostasis modification during OC and HR treatment.
Haemostasis and thrombosis
Normal haemostasis is the result of an equilibrium between coagulation, the formation of the fibrin clot that is responsible for the arrest of bleeding after vessel injury and the elimination of fibrin that forms in the circulation (fibrinolysis) (Fig. 1). Coagulation depends on platelets and on plasma clotting factors (such as fibrinogen, factors II, V, VII, VIII) and is controlled by physiological inhibitors (antithrombin, protein C, and protein S). Fibrinolysis depends on plasminogen, the precursor of the fibrinolytic enzyme plasmin, and its activators (tissue-plasminogen activator (t-PA) and urokinase-type plasminogen activator (u-PA)). It is controlled by physiological inhibitors (plasminogen activator inhibitor (PAI-1), α2 plasmin inhibitor, and thrombin activatable fibrinolysis inhibitor (TAFI)).

Normal haemoetasis. AT, Antithrombin, PC, protein C, PS, protein S, PAI, plasminogen activator inhibitor, TAFI, thrombin activatable fibrinolysis inhibitor.
Thrombosis may be caused by an imbalance between coagulation and fibrinolysis. The mechanisms that may be involved include: increased coagulation due to an increase in the number or functional activity of platelets, an increase in coagulation plasma factors, or a decrease in inhibitors. This corresponds to a procoagulant effect. Decreased fibrinolysis may be due to an alteration of the plasminogen system: a defect in plasminogen or fibrinolysis activators, or an increase in fibrinolysis inhibitors. This corresponds to hypofibrinolysis.
Venous and arterial thrombosis are not associated with the same haemostasis modifications (Table 1). Venous thromboembolism has been shown to be increased in patients who have a congenital deficiency in antithrombin (AT), protein C (PC), protein S (PS); abnormal activated PC resistance related to the factor V Leiden mutation; or the prothrombin 20210A variant. Arterial thrombosis (myocardial infarction, cerebrovascular accident) depends on platelets, fibrinogen, and decreased fibrinolysis due to increased PAI-1 levels. t-PA (measured by immunological methods (t-PA antigen)) is also a risk indicator of myocardial infarction, since it reflects the amount of complex t-PA/PAI-1 (1–3). Increased factor VII levels were previously considered a risk factor, but recent studies have not confirmed these findings.
Modifications of haemostasis during oral contraceptives (Ocs) and hormone replacement therapy (HRT)
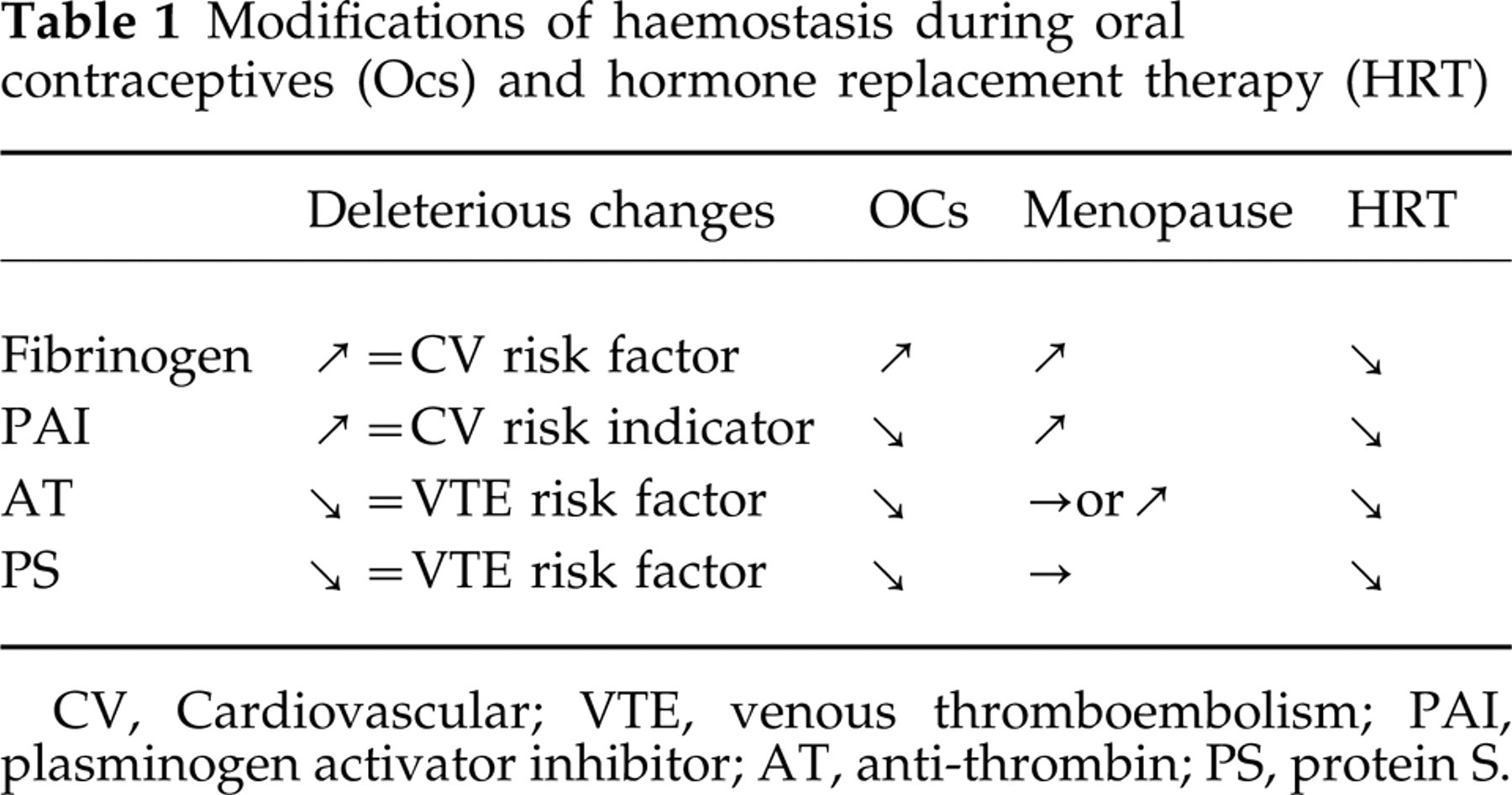
CV, Cardiovascular; VTE, venous thromboembolism; PAI, plasminogen activator inhibitor; AT, anti-thrombin; PS, protein S.
Activation markers may reflect an imbalance between coagulation and fibrinolysis. Fibrinopeptide A (FPA) and thrombin–antithrombin complexes are markers of coagulation activation. Their use is restricted to special-ized laboratories and to relatively small series of patients because preanalytical conditions are crucial (blood sampling, storage and methodology). Prothrombin fragment 1 + 2 (F1 + 2) and D-dimers (indirect markers of coagulation activation) are reliable and feasible.
Oral contraceptives and haemostasis
Combined oestro-progestogens that contain ethinyl estradiol and a progestogen are the most commonly used OCs, but progestogen-only contraception may also be used.
Combined OCs
Venous thromboembolism
Since 1961, when pulmonary embolism was first reported in association with OC use, many epidemiological studies have addressed the potential thrombotic risk of OCs. Many of these studies demonstrated an increased risk of venous thrombosis (see (4) for review). It was primarily associated with the oestrogen content of the contraceptives (5). As a result, ethinyl-estradiol (EE) dosage was decreased from more than 100 μg to 20 μg. Simultaneously, different progestogens were used with EE to decrease the deleterious androgenic metabolic effects. Newer OCs containing the third generation progestogens were considered safer.
Recent independent studies (6–12) have confirmed that the risk of thromboembolism is increased by OCs (Table 2). Odd ratios were 3–4 when all oral contraceptives were considered. OCs containing a third generation progestogen (mainly desogestrel and gestodene) were associated with a two-fold higher risk of thrombosis than those containing a second generation progestogen (levonorgestrel) (Tables 2 and 3). None of the studies was randomized and the rationale for prescribing second or third generation OCs was unknown. Confounding and bias (age, duration of exposure, family history of venous thromboembolism, prescription bias), have been suggested and analysed (13–15). Some factors may have influenced the results. Young women starting on OCs and women at higher risk were probably prescribed newer OCs, i.e. third generation, since third generation OCs were considered ‘safer’. Because of the effects on lipids, they were adequate for the arterial risk, but there was no clear evidence that they decreased the risk of venous thrombosis. When duration of exposure and age were taken into account, the increased risk of third generation OCs was no more significant than second generation OCs (9, 16, 17). Family history of venous thromboembolism is an important risk factor: OR 2.5 (95% CI 1.2–5.2) in a recent study (7), but it was not recorded in most studies. The proportion of women with a family history of venous thrombosis was higher in women who took third generation OCs (23%) than it was in women who took 2nd generation OCs (7%) (18). A slightly increased risk exists with 3rd generation progestogens, but neither of them is devoid of risk of thromboembolism.
Risk of venous thromboembolism and oral contraceptive use in recent studies

OCs, Oral contraceptives; DSG, desogestrel; GD, gestodene; LNG, levonogestrel.
Venous thromboembolism in oral contraception comparison of third and second generation progestins

OR, Odds ratio; 95% CI, confidence interval; BMI, body mass index. Adjusted for:
BMI and other factors;
factor BMI and smoking;
for age;
for age, smoking, centre, BMI, duration ofexposure;
age, calendar time, family history, centre.
Even though the relative risk of third generation OCs is about twice that of second generation OCs, the absolute risk is small (8). Estimates of the incidence of venous thromboembolism in the general population is less than one event per 10 000 women per year, and it is increased to 3–4 in women taking all OCs. In comparison, the estimate is six during pregnancy.
Women with a congenital predisposition to venous thrombosis (thrombophilia related to deficiency in anti-thrombin, protein C, protein S, or factor V Leiden mutation) may be at higher risk (6, 19–21). The estimate risk is 8 per 10 000 women per year in factor V Leiden carriers who are not using OCs and 30 in carriers who are users. The risk of cerebral venous thrombosis associated with OCs is also increased in women with thrombophilia (22–26).
Haemostasis
Haemostatic changes seen in patients on OCs in the 1960s were due to elevated levels of coagulation factors, increased thrombin generation and decreased levels of antithrombin (27). This latter finding was considered very important since Egeberg published, in 1965, the first case of congenital antithrombin deficiency associated with venous thrombosis. Later, it became evident that OCs were associated with coagulation modifications that increased the risk of thrombosis, and changes in fibrinolysis, which were favourable (see (28) for review). The following are some of the observed changes:
Hypercoagulability associated with elevated levels of fibrinogen (factor I) and coagulation factors VII, VIII, and X, and decreased levels of physiological inhibitors (antithrombin AT and PS) and acquired activated protein C (APC) resistance.
Hyperfibrinolysis with increased levels of plasminogen (the precursor of the active fibrinolytic enzyme, plasmin) and decreased levels of PAI-1 (the physiological inhibitor of fibrinolysis).
Increased capacity of coagulation activation as evidenced by elevated levels of fibrinopeptide A and prothrombin fragment 1 + 2 and fibrinolytic markers: plasmin–anti-plasmin complexes and D-dimers. D-dimers are plasmin-induced fibrin degradation products, and their presence is a sign of excessive fibrin formation (fibrinogen is converted to fibrin, cross-linked by factor XIII and lysed by plasmin).
The above modifications are generally deleterious for the venous risk (decrease in AT and PS, APC resistance, increased factor VIII) and beneficial on the arterial risk (increased fibrinolysis), except that fibrinogen is increased. Consequently, haemostasis seems important on the venous side, and other risk factors (lipids, arterial blood pressure, smoking) are probably more important for the arterial risk.
The magnitude of the changes is generally modest and most results remain in the normal range, except for the decrease in protein S. The hyperfibrinolysis may counterbalance the hypercoagulability in most women and may explain the relatively low absolute risk of thrombosis in the general population.
The risk of thromboembolism was initially related to the ethinylestradiol content of OCs, but the dose-dependent effect on haemostasis has not been clearly demonstrated. It was suggested for factor VII (29) and in a model reflecting fibrin deposition on the subendothelium of rabbit aorta (30). At lower concentrations, i.e. 20 μg, minor changes were still present but did not reach statistical significance for most parameters (30, 31).
The biological plausibility for the increased risk of venous thrombosis during treatments with third generation progestogens was seldom studied. Different progestogens with different anti-oestrogenic and androgenic activities, have been combined with ethinyl estradiol. The first generation progestogens, such as norethisterone, had androgenic effects that might increase the risk of atherosclerosis; they were suspected to metabolize to oestrogenic compounds. Second generation progestogens, such as norgestrel or levonorgestrel, are the most frequently used, less androgenic third generation progestogens, desogestrel, gestodene, norgestimate.
Few studies have compared the haemostasis changes of different progestogens combined with the same dose of ethinyl estradiol. No clear difference in levels of fibrinogen and coagulation factors II, VIII or X, or anti-thrombin and fibrinolytic activity has been observed (32–36). However, a tendency to lower levels of anti-thrombin and higher levels of coagulation factors was seen with the third generation progestogens (Table 4). Recently, a decreased sensitivity to activated protein C resulting in an acquired APC resistance was observed in OC users (37). The lack of protein C activation of protein C was more pronounced in women taking third generation progestogens than in women taking second generation progestogens. Similar modifications were found in heterozygous carriers of factor V Leiden mutation who were not treated with OCs. These findings could represent a biological plausibility for the epi-demiological observation of a higher risk of venous thrombosis in OC users, especially those using third generation progestogens. However, the selection bias that existed in the epidemiological studies of third generation progestogens might also exist in this study. Groups were not randomized and prescription bias could also play a role. The same selection bias may exist in Rosing's study, which looked at thrombin generation in the presence of activated protein C (37).
Third and second generation oral contraceptives (OCs) and haemostasis

LNG, Levonorgestrel; DSG, desogestrel; GD, gestodene; AT, anti-thrombin; PC, protein C; PS, protein S; ELT, euglobulin lysistime; WBCT, whole blood clotting time; PG, progestogen; tPA, tissue plasminogen activator; PAI, plasminogen activator inhibitor.
Progestogen-only contraception
Progestogens may be used for oral contraception either at low doses administered continuously (levonorgestrel) or at higher doses for 21 days followed by an interruption of 7 days (chlormadinone acetate). When administered on this schedule alone, they do not significantly increase the risk of venous thromboembolism. With the exception of lynestrenol, which was associated with a reduction of antithrombin (38), low-dose progestogens are not associated with marked changes in coagulation or fibrinolysis variables (39–42). Their use has been proposed for women who are at risk of venous thromboembolism (43).
Hormone replacement therapy, thrombosis and haemostasis
Menopause
Although menopause is associated with the loss of the cardiovascular protection observed in fertile women, the risk of venous thromboembolism does not increase.
Menopause is associated with an increase in factor VII, fibrinogen and PAI levels leading to hypofibrinolysis (which has a deleterious effect on the cardiovascular) (44). It may reflect an imbalance and a prothrombotic effect of menopause. Some conditions may influence these modifications. Physical exercise induces an increase in fibrinolysis that has been confirmed in physically active menopausal women (45). In addition, a factor VII polymorphism (Arg353Gln), which is present in a small proportion of women, is not associated with the expected increase in factor VII after menopause (46).
Hormone replacement therapy
Hormone replacement therapy has been shown to be cardioprotective in women who do not have a history of coronaropathy. In contrast, observational studies suggest that HRT increases the risk of venous thromboembolism (47–50). Odds ratio of 2.1–3.6 were reported (Table 5) (see (51) for review).
Venous thromboembolism and hormone replacement therapy (HRT)

In a recent randomized study, Heart and Estrogen/progestin Replacement Study (HERS), HRT or placebo was administered to post-menopausal women with coronary artery disease (52). No difference was observed in the primary outcome of the study, namely non-fatal myocardial infarction or death due to coronary heart disease. This unexpected result was associated with a significant increase in the risk of venous thromboembolism. The women included in the HERS trial were older than those in previous studies, suggesting that advancing age and other conditions, such as hypertension, diabetes, and smoking, may account for these results.
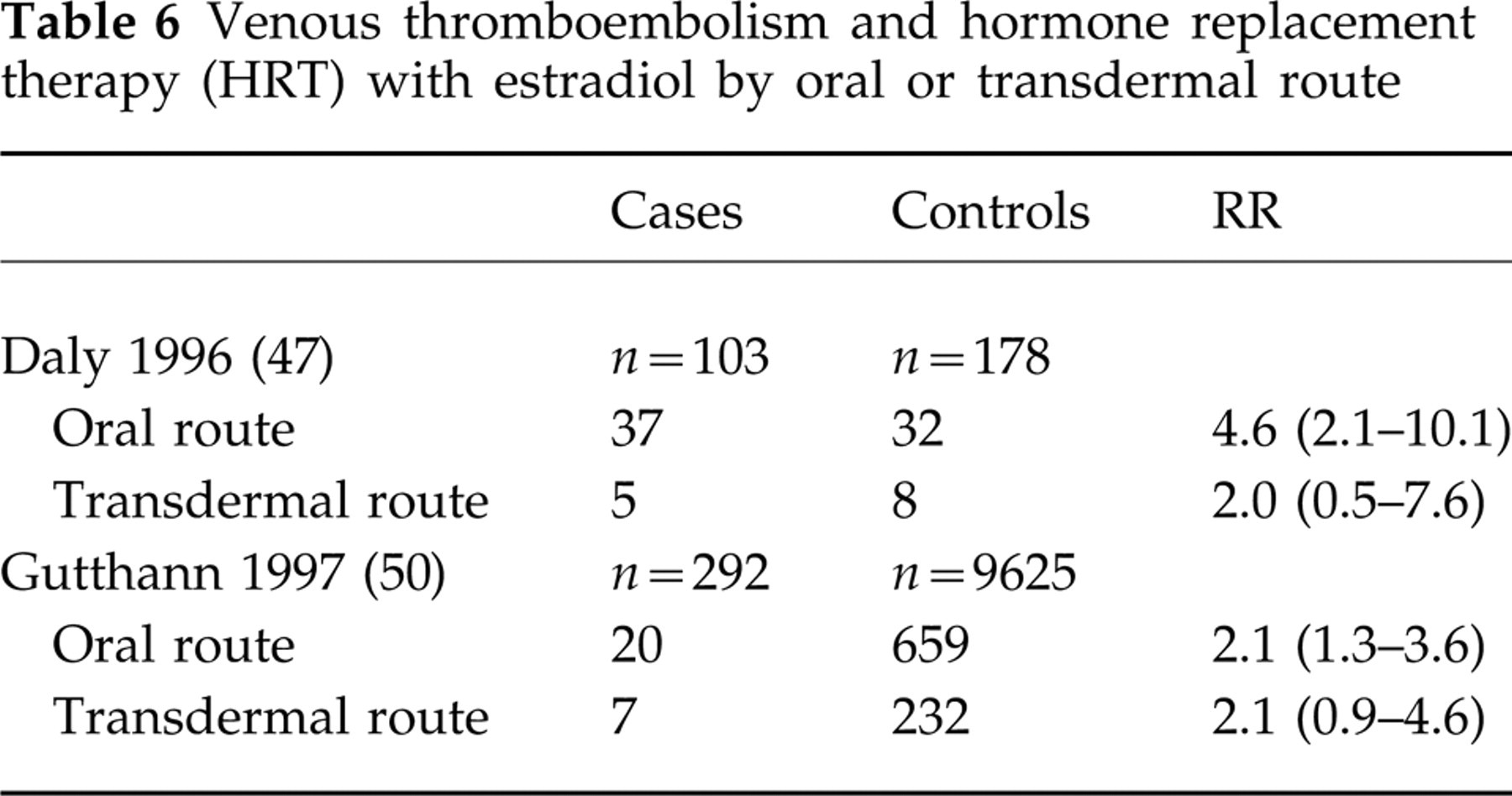
In all the published epidemiological studies, the oestrogens that were used were mainly conjugated equine oestrogens, sometimes oral 17β estradiol, rarely transdermal 17β estradiol. No significant difference was observed between the transdermal route and other routes, but the number of women treated was too small to draw definite conclusions (47, 50) (Table 6).
Venous thromboembolism and hormone replacement therapy (HRT) with estradiol by oral or transdermal route
Some modifications of haemostasis observed during HRT counteract the effect of menopause and are beneficial for the cardiovascular risk (profibrinolytic effect with decrease in fibrinogen and PAI) (51, 53, 54). Others (i.e. decrease in AT, PS, abnormal APC resistance) induce a procoagulant effect and are deleterious for the venous risk. In addition, activation coagulation markers (fibrinopeptide A, prothrombin fragment 1 + 2, D-dimers) are also increased with HRT (55).
Modifications of factor VII are not homogeneous: increased, as well as decreased, levels have been reported with HRT. Factor VII polymorphism may, in part, explain these discrepancies (46).
Conjugated equine oestrogens have been studied more frequently than 17β estradiol (53, 55, 56). Oral and transdermal routes of administration have been compared in an open study (41) and a randomized controlled trial (57). The modifications seen with the oral route were similar to those seen with conjugated equine oestrogens; in contrast, there was no significant modification with the transdermal route. This may mean that the transdermal route does not have a deleterious effect on the venous risk, but the cardiovascular protection may be lacking if fibrinogen and fibrinolysis parameters are surrogate end-points.
Conclusion
The oestrogens and progestogens that are used in OCs are different than those used in HRT. The synthetic oestrogens that are used for oral contraception and the oral conjugated equine oestrogens that are used for HRT are associated with an increased risk of venous thrombosis. We need more information concerning 17β estradiol by the oral and even more by the transdermal route. Although slightly higher risk is likely with OCs containing third generation progestogens, there is still a significant risk with second generation progestogens.
OCs induce deleterious effects on coagulation (decrease in AT and PS, APC resistance) that may favour venous thrombosis. This may explain the increased risk in women with pre-existing risk factors (i.e. history of venous thromboembolism and/or congenital thrombophilia). Effects on fibrinogen and fibrinolysis (decrease in PAI, increase in plasminogen) are beneficial and theoretically could prevent cardiovascular disease.
HRT with conjugated equine oestrogens and oral estradiol induce similar changes with the exception of the fibrinogen, which is not increased but decreased. HRT using the transdermal route does not induce any significant change in haemostasis. This could be a good reason for using this treatment in women who are at high risk of venous thrombosis (who have a history of venous thromboembolism and/or congenital thrombophilia) and even though it may not have the expected cardioprotective potential. These assessments presuppose that haemostasis markers are good surrogate end-points, but this has not been clearly demonstrated.
Progestogens, associated with oestrogens or administered alone, have been less studied. Much attention has been given to third generation progestogens combined with ethinylestradiol for contraception; the effects of progestogen-only contraception or progestogens associated with estradiol for HRT have been incompletely studied.
Finally, it is well known that thrombosis is multicausal and it is now recognized that it may be plurigenic. The risk of thrombosis related to OCs and HRT is probably low in the general population, but we should direct our efforts to detecting women who are at risk for venous or arterial thrombosis in order to give them the most appropriate treatments. In addition, some conditions such as physical exercise or genetic conditions may counterbalance abnormalities induced by menopause. Their influence on the cardiovascular risk of menopause may be important and further studies are needed to establish this.