
Abstract
A study was made of the personality profiles of a sample of 51 patients with chronic tension-type headache (CTH) employing the Minnesota Multiphasic Personality Inventory (MMPI). Two clusters were obtained by applying multivariate classification techniques: cluster 1 (with elevations on scales Hy, D and Hs only) and cluster 2 (exhibiting elevations on most scales except Pd, Mf and Si). Fifty subjects without chronic pain or known psychiatric disorders, and extracted from the same social setting as the patients, completed the MMPI as a control group. Fluoxetine treatment was started in the CTH group, with follow-up over a 1-year period. Chi-squared analysis correlating the clusters obtained to different pain-related variables and epidemiological parameters revealed a significant association to sex only. There were no differences in therapeutic response between the two clusters. However, the patients belonging to the less perturbed cluster who exhibited profiles analogous to those of the control population showed significant improvement with respect to the global sample and their own cluster.
The physiopathology of tension-type headache (TH) is unclear (1–3). Increased sensitivity to pain is thought to play a role in the pathogenesis of chronic tension-type headache (CTH). In this sense, disfunction of endogenous brainstem pain centres under the control of limbic structures, linked to psychological stress and somatization processes, have been supposed to play a pivotal role (4, 5).
Patients with TH suffer considerable psychological discomfort in comparison to the general population or migraineurs (6–8). In a subgroup of patients, persistent pain has been claimed to be related to underlying psychological pathology or personality disorders (9, 10). In this way, according to DSM-IIIR criteria, up to 65% of patients with CTH suffer mental disorders (11), including anxiety (6, 8, 11–13), neurosis (14, 15), depression (16–18), psychological stress (18–22), conversion (11) and, exceptionally, psychopathy (23).
It is generally accepted that the psychological disorders associated with headache are more marked when the pain becomes chronic or exhibits increased ‘density’, i.e. when the number of weekly days in pain increases. These observations are in turn independent of the diagnostic category involved (6, 24, 25).
Two tendencies currently exist when addressing the underlying cause of personality disorders in patients with TH. One hypothesis is of aetiologic significance and suggests that headache results from an original personality disorder that favours the appearance of headache in the event of certain types of conflict (6, 24, 25). In contrast, other authors consider the reactive and emotional syndrome to be a secondary phenomenon appearing as part of a behavioural strategy to cope with pain (6, 10, 25–28).
It is generally accepted that mental tests offer scant discriminating power as regards the organic or psychic origin of pain (29, 30). However, the psychological factors must be taken into consideration and treated in all patients with CTH. Psychological exploration is thus a necessary part of the evaluation of such patients (31).
In headache sufferers, an association between pain density and increased MMPI profile alteration has been observed (32–35) – the progression of psychopathological alteration forming a continuum. Thus, patients with vascular headache yielded more normal MMPI profiles than patients with TH and mixed headache (32, 36–40).
As in the case of other forms of chronic pain, the first three clinical scales of the MMPI best reflect the psychological problems of patients with headache (15, 29, 32, 35, 38, 39, 41–43). Moreover, the application of multivariate classification techniques known as cluster confirms the heterogeneity of the population by generating different subgroups.
In this study we have endeavoured to classify CTH patients in different clusters according to their MMPI profiles and to assess the putative predictive value of MMPI clusters with regard to the therapeutic response.
Patients and methods
Fifty-one consecutive patients (44 females and 6 males; mean age 37 years, range 19–62) with CTH according to the diagnostic criteria established by the Headache Classification Committee of the International Headache Society (44) were recruited from among patients seeking treatment at an outpatient general neurological clinic. Patients were required to complete the MMPI under psychologist supervision at the initial clinical visit. In the absence of contraindications or pregnancy, Fluoxetine treatment (20 mg) was started. The patients were allowed to take their usual analgesics. The subjects were requested to record their headache activity until the end of the study; they used a headache diary where a daily record was kept of all headaches experienced and the number and type of pills taken (45). At the follow-up visit, the diary was collected and analysed. Percentage headache frequency was calculated by dividing the number of days with headache by the total number of recorded days. Similar calculations regarding analgesic dosing, and the percentage of days that the patient suffered headache, were also determined. The patients were followed-up on a bimonthly basis for 1 year.
The patients were examined at the University Hospital (Badajoz, Spain). Referrals came from general practitioners. The neurological examination and CT scans of the head were normal in all patients. Fifty controls from the patients' personal environment and without headache, pain or psychiatric diseases were also required to complete the MMPI.
A hierarchical clustering procedure (Ward's method) was conducted using the K-corrected T-scores from the validity and standard clinical scales of the MMPI. Cluster analysis was initially applied to the patient sample, and posteriorly to the patient and control populations combined. Decisions regarding the optimal cluster solution were made based on the differences in root variance. The global patient group and cluster subgroup mean trait scores were compared by the t-test vs. the control population.
Chi-squared tests were performed to determine differences between clusters in reference to the MMPI scales, head pain parameters and demographic variables.
The evolution criteria were: percentage improvement of headache (days per week) and analgesic doses eliminated weekly. The following responses were considered: full improvement (up to 75% reduction in painful days), partial improvement (50–75% reduction) and without improvement (less than 50% reduction).
The Mann–Whitney U-test was used for the statistical evaluation of small samples.
Results
The mean MMPI scales values for the patient series vs. the controls are shown in Table 1.
Mean MMPI T-scores (K corrected) for the patients vs. controls

A two-cluster solution was considered to best represent the data obtained. The MMPI cluster profiles for patients vs. controls are shown in Fig. 1. The two clusters obtained are similar to those previously reported in the headache literature, and moreover resemble the MMPI clusters described in previous studies of chronic pain patients. The mean MMPI sub-scale scores for each cluster group are shown in Table 2. Cluster 1 subjects (n = 16) displayed significant elevations on the hypochondria (Hs), depression (D) and hysteria (Hy) scales, the highest increase corresponding to the Hs scale. In turn, cluster 2 headache sufferers (n = 35) constituted the most ‘psychopathological’ group, with significant elevations on scales Hs, D, Hy, psychopathia (Pd), paranoia (Pa), psychasthenia (Pt), schizophrenia (Sc), mania (Ma) and social introversion (Si).
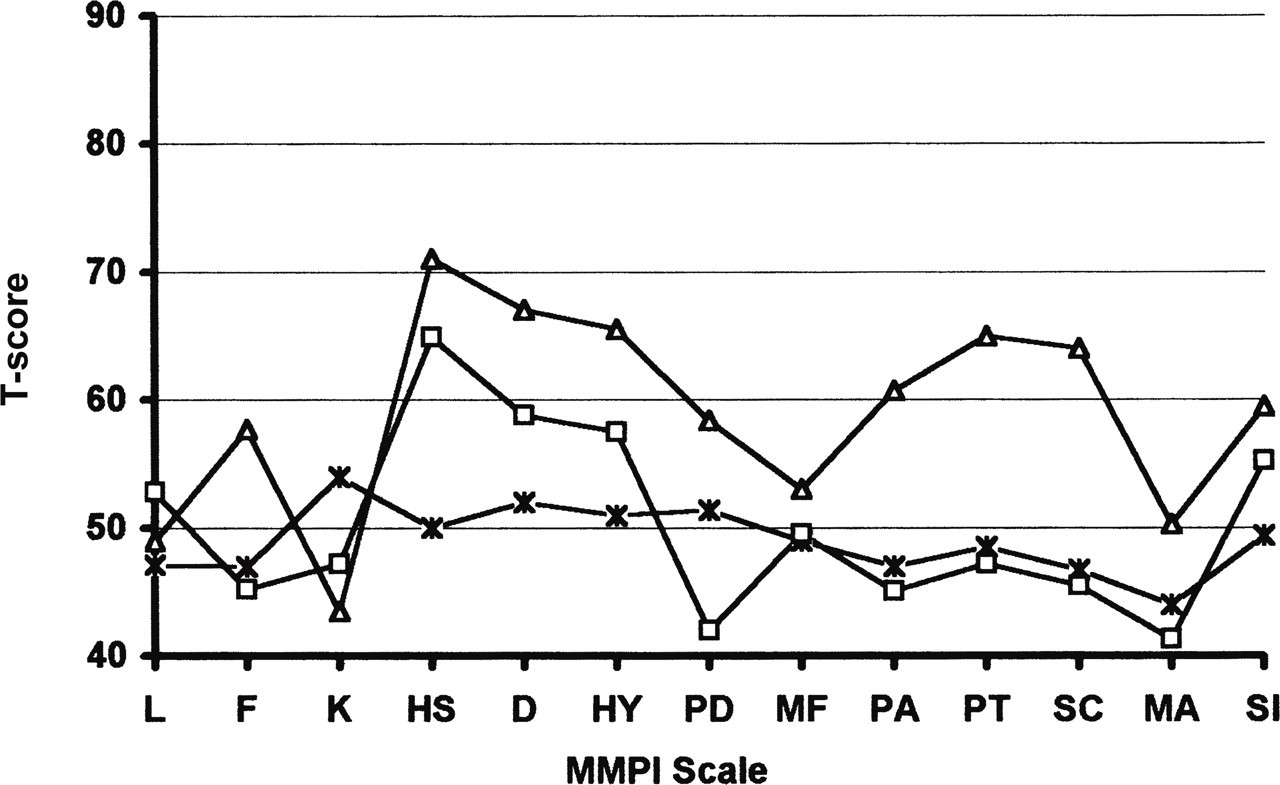
This figure shows the mean MMPI profiles for each cluster group. X = control; □ = cluster 1; Δ = cluster 2.
Analysis of differences between means values (K-corrected) of MMPI T-score for each cluster vs. control group (Student's t-test). Right column: F value of each variable between evolution groups by analyses of variance (*not significant)

The mean values of the scales of the two clusters were compared with the control population by means of the Student t-test. Cluster 1 exhibited statistical significance for Hs, D, Hy and Pd, while cluster 2 showed significance for scales Hs, D, Hy, Pd, Pa, Pt, Sc, Ma and Si (Table 2).
The number of subjects pertaining to each cluster, and the corresponding mean age and headache frequency data are provided in Table 3, with application of the chi-squared test. The subjects in each cluster did not differ significantly on any of the headache frequency variables. Likewise, the clusters were not significantly different in terms of age, pain severity or demographic parameters. Only gender exhibited a significant association, since five of the six males were in cluster 1.
Demographic and headache parameters between cluster 1 and cluster 2 by χ2 analysis (*significant)

On applying the same multivariate classification techniques to the combined population of patients and controls, both groups were found to overlap – with the exception of some subjects pertaining to the more perturbed cluster.
At the end of follow-up, one-way
Discussion
On comparing the CTH patients with the controls (i.e. subjects without pain or known psychiatric disorders and extracted from the same social setting as the patient group), statistically significant differences (P < 0.01) were detected for the following clinical scales: Hs, D, Hy, Pa, Pt, Sc and Si.
Of the few studies that have employed cluster techniques to study the classification of headaches, Ward's hierarchical method is the most widely adopted in psychosocial and biomedical science (46, 47). Prior to application of the method, however, it is important to differentiate primary headache categories and the episodic or chronic variants of TH (35, 40).
The classification attempts described in the literature involve solutions of between two and six clusters – the most widely adopted solution being four clusters (35, 40, 48, 49). In our series of patients with CTH, the two-cluster solution was found to sufficiently delimit the two populations in terms of psychological profile. These two differential patterns were:
• Cluster 1 (n = 16) reflected clinically significant elevations on MMPI scales Hy, D and Hs, i.e. it represented a psychologically well-adjusted subgroup with increased neurotic traits. Significant elevations were observed in relation to the following scales: Hs, D, Hy and Pd. This was the group closest to normal. A total of 16 patients belonged to this cluster – a proportion (30%) lower than expected (35, 50). It comprised the classical group of individuals with an increased neurotic triad (35, 43) and patients exhibiting a normal profile but with a hypochondriac tendency (35, 51, 52). In our study five cases belonged to this latter population. Although this profile is generally attributed to young females (35), in our sample all ages and five of the six males were represented.
• Cluster 2 (n = 35) in turn showed a profile of psychopathological appearance, with slightly higher elevations on MMPI scales Hy, D and Hs than in cluster 1 – though with a predominant and significant increase in psychotic scales (Pa, Pt, Sc, Ma and Si). This pattern has been mainly described in females, and corresponds to the psychologically most affected subgroup where even anti-psychotic drugs are advocated (35, 51, 53).
Both clusters exhibited a highly perturbed psychological profile significantly distinct to that of the control group.
The overlapping of controls and patients was observed in cluster 1 (eight cases) and in the less severe profiles of cluster 2 (11 cases). The patients with CTH exhibited a personality profile that formed a continuum of increasing severity, where the maximum alteration corresponded to psychologically very perturbed individuals.
These controls reflected the personality profiles described in patients with pain or chronic headache. The sample also contained patients with normal personality profiles.
The global response of this population to anti-depressive medication was poor. Only 20% showed healing criteria, including the five patients with personality profiles closest to the controls. This subgroup derived statistically significant therapeutic benefit vs. its own cluster and the global samples – suggesting that therapeutic response improves with increasing normality of the personality profile (54). There were no differences in therapeutic response between the two clusters.
Unlike in the context of chronic pain of other locations (51, 54–58), we were unable to confirm an improved prognosis in the group with an elevated D scale – probably because of the contribution made by the rest of the psychopathological variables.
In our sample the male:female proportion was 1:8, i.e. higher than expected (48). We found no relationship between MMPI clusters and age. Although there were few males, their grouping within the less perturbed cluster is an interesting finding not previously reported.
Given the lack of a relation to the severity of headache, these cluster types seem to more likely reflect different levels of personality disorders (59).
Under adequate environmental circumstances, a pain-prone psychological profile (14, 54) may evolve from an organic acute episode towards a chronic disorder (60). Consequently, in order for the therapy of patients with chronic headache to be successful, the corresponding personality profiles should be known, and detailed insight must be gained into those environmental mechanisms capable of contributing to the development and maintenance of chronicity (14, 32, 35).
The predictive capacity of the MMPI as regards the therapeutic response of headache patients is a useful tool (30, 61–63). As in the case of other studies (63, 64), we recommend a two-cluster solution to classify CTH patients. In this context, a cluster 1 subgroup closer to normality would imply a better prognosis.
Pharmacological treatment has not been found to be superior to behavioural therapeutic interventions, or vice versa, in the management of chronic pain. The low improvement rate of TH may be due to the existence of a perturbed personality profile. A proportion of highly altered patients with long-term psychosocial problems, who gain little from an improved health status, are unlikely to respond to any form of treatment – since such individuals achieve their best psychic balance by maintaining their patient role (65).
Footnotes
Acknowledgements
This work was supported by a grant from the Caja de Badajoz.