
Abstract
This paper presents data on clinical and financial outcomes of five years use of clozapine in an entire cohort of (32) psychiatric patients in a community (the Australian Capital Territory). Such information could assist psychiatrists in community practice in deciding about the use of clozapine in the treatment of persons with treatment-resistant schizophrenia [1]. Currently there is little relevant research data available.
Clozapine became generally available for use in treatment-resistant schizophrenia following the 1988 study by Kane et al. [1]. Since then the use of other atypical antipsychotics may have reduced the incidence of treatment-resistant schizophrenia and limited the role for clozapine. This study does not address such issues.
Most of the evidence for concluding that ‘clozapine is convincingly more effective than typical antipsychotic drugs in reducing symptoms of schizophrenia’ [2–4] relates to hospitalized patients but the future use of clozapine will be, predominantly, community based. Cochrane reviewers [2] concluded that ‘large randomised, community-based trials… are required’. To date, there are very few reports of (even uncontrolled) community studies extending for two years or more [5–10].
Clozapine has numerous common and troublesome, but also some relatively rare and dangerous, side-effects [11–13]. Regular blood monitoring is required for its continued use. Informed consent for its use is essential. Hence, clozapine will only be used in community practice if it is seen to have significant clinical value.
Singh et al. [14] recommend including economic evaluations in clinical outcome studies so that results will influence system-wide policies. Revicki has reviewed pharmacoeconomic studies of clozapine [15]. Yet the evidence is not conclusive. In fact, it is very difficult to produce such evidence on this complex issue [16–18].
An opportunity to collect data concerning the clinical value and economic cost of the long-term use of clozapine in community practice presented itself in the Australian Capital Territory (ACT) and surrounding region (population of about 400 000 people). This is a relatively closed community with a long tradition of community based management of patients (the ACT has never had a long-stay hospital). In 1993 almost all patients suffering from treatment-resistant schizophrenia were managed in the community. When clozapine became available a clozapine coordinator was appointed, which allowed detailed records of, and personal contact with, patients on clozapine to be maintained, thereby providing data and facilitating access to subjects for follow-up.
Method
This study employed the same methodology as the 3 year follow-up study previously reported. A more detailed description of our methodology is available in that report [7]. Data from that study have been used in compiling results for this study.
Subjects
Participants were all patients who commenced clozapine in the ACT before 1 July 1994, with a clinical diagnosis of schizophrenia or schizoaffective disorder, and whose psychiatric history was known.
Design
This was an open-label, retrospective study of community-based clinical practice. Information concerning each year for the first five years after clozapine was prescribed was compared with data from the preceding two years. Preclozapine demographic, clinical characteristics and history were collected.
The cohort (intent to treat) was divided into two groups (continuers and discontinuers). Continuers were on clozapine three years after commencing clozapine (YEAR3) and remained on clozapine for the next two years (YEAR5) without having 12 weeks or more off clozapine in that period. Data were processed for three groups – the cohort (all subjects), the continuers and the discontinuers – either for each year of the study or at baseline, YEAR3 and YEAR5, depending on the outcome measure employed.
Data were obtained from the ACT hospital and community health system records, the Clozapine Patient Monitoring System (CPMS), and from other sources when appropriate. Every effort was made to examine all relevant data sources and to document progress for all subjects.
Outcome measures
Outcome measures were changes in clinical state and occurrence of side-effects, living circumstances and employment status at YEAR3 and YEAR5 compared with baseline, and changes in hospital admissions, occupied bed days (including hostel beds) and costs of treatment in each of the five years after clozapine was prescribed (YEAR1, YEAR2, YEAR3, YEAR4 and YEAR5) compared with the two years preceding clozapine use (2 YRS PRE and 1 YR PRE), and dose of clozapine.
Brief Psychiatric Rating Scale and Life Skills Profile
Where possible, Brief Psychiatric Rating Scale scores (18 items; 1–7 scale) [19] and Life Skills Profile scores [20] were collected preclozapine and approximately 5 years after commencing clozapine.
Clinical status
For each subject, the treating psychiatrist reported the change in clinical status which had occurred at YEAR3 and the change in clinical status which occurred between YEAR3 and YEAR5. Clinical status was measured using a seven-point rating scale from marked deterioration to marked improvement. The treating psychiatrist also reported the occurrence of side-effects.
Bed use
The number of hospital and hostel bed days and number of admissions, directly or indirectly attributable to a psychiatric illness, were recorded for each year of the study period for each subject. Being in hospital at the end of one year and the beginning of the next was counted as an admission in both years. Admissions to hospital to commence clozapine were counted as admissions in YEAR1. Hostel bed days included all days in a fully staffed hostel in the ACT or elsewhere.
Costs
Bed costs (the costs of hospital and hostel bed occupancy) and costs of treatment (bed costs plus the costs of clozapine tablets and blood monitoring and a proportion of the costs of employing the clozapine coordinator) were estimated for each subject for each year of the study. All costings were made at 1996–1997 values (Australian dollars) using figures supplied by the health department. No attempt was made to cost other medications or other community services or to assign a value on improvements in patients.
Living circumstances and employment
The living circumstances (whether or not the subject was in either a hospital or hostel at YEAR3 and YEAR5) were established from official records. Information concerning employment at YEAR3 and YEAR5 was supplied by the treating psychiatrist and by case managers.
Analyses
Data analysis was conducted using parametric and non-parametric procedures in the statistical package SPSS (SPSS Inc., Chicago, IL). Statistical comparisons of demographic and clinical characteristics between continuers and discontinuers were based on Fisher Exact probability tests and Mann–Whitney and t-tests. A separate variance t-test was used when Levene's test revealed a significant difference in variance for the two groups. Otherwise, a pooled variance t-test was used. The effect of clozapine on clinical status was analysed using Binomial tests to compare the proportions of patients who had improved or deteriorated. The effect of clozapine on admission to hospital (admitted or not) and on employment and living circumstances, was analysed using Cochran Q-tests followed by McNemar tests. The effect of clozapine on time spent in hospitals and hostels, treatment costs, and the number of hospital admissions was analysed using Friedman analyses followed by Wilcoxon tests where the former were statistically significant. Where data for the two years preclozapine did not differ significantly these were averaged before further analyses were undertaken (comparing preclozapine with postclozapine). Analyses were conducted separately for the cohort, continuing and discontinuing groups. Subsidiary analyses comparing outcomes for the continuers and discontinuers at 5 years postclozapine were conducted using Mann–Whitney and Fisher Exact probability tests.
Results
Characteristics of the sample
The effective sample size, on an intent to treat basis, was 32. Although 42 subjects met the requirements of entry to the study, 10 were excluded from consideration. Two subjects died from causes unrelated to either their psychiatric illness or their psychiatric treatment. Both had markedly improved while on clozapine (one was on clozapine for two years until she died, the other was withdrawn from clozapine after a year because of agranulocytosis and then remained improved, on olanzapine, until he died two years later). One subject ceased clozapine after only a few weeks because a pre-existing senile dementia progressed. Seven subjects moved out of the region, three of whom were on clozapine and clinically improved when they moved (one returned to her home, overseas). The other four discontinued clozapine within the first three years and had no further clozapine (according to CPMS records). At last contact, their clinical condition remained unchanged from baseline.
Of the remaining cohort of 32 subjects, 22 (69%) were continuers and 10 (31%) were discontinuers. Most subjects were aged between 20 and 45 and had little history of hospital based care. There were no statistically significant differences in clinical or demographic characteristics between the groups.
Of the 22 continuers, 20 took clozapine almost continuously for five years, and two discontinued clozapine in YEAR1 but recommenced it in YEAR3 and continued on it to the end of YEAR5. Among the continuers, there was little change in the mean dose between YEAR3 and YEAR5 (375 mg/day; range = 100–575, and 356 mg/day; range = 100–575, respectively).
Four discontinuers used clozapine continuously for three years after which one (moderately improved at YEAR3) changed to risperidone at her request and maintained her improvement; one (moderately improved at YEAR3) became non-compliant and clozapine was ceased with a subsequent slight deterioration in his condition at YEAR5; and one with moderate improvement and one with marked improvement at YEAR3 both developed cardiac problems during YEAR4 and clozapine was withdrawn after which they relapsed to their previous status. (These subjects are Patients A and B see Outcomes). Of the other 6 discontinuers, 4 used clozapine for only a few weeks, one used clozapine for long periods with a number of breaks and finally ceased using clozapine early in YEAR4, and one (Patient C, see discontinuers) used clozapine for a year without benefit and clozapine was stopped but it was recommenced early in YEAR5.
Outcomes: cohort and continuers
Brief Psychiatric Rating Scale and Life Skills Profile
Brief Psychiatric Rating Scale (BPRS) data were available both preand postclozapine for 13 subjects (10 continuers and 3 discontinuers). BPRS scores did not improve significantly over time either for the cohort (p = 0.27) or for the continuers (p = 0.07).
Life Skills Profile (LSP) data were available for both pre- and postclozapine for 11 subjects (8 continuers and 3 discontinuers). Life skills improved significantly over time both for the cohort (p < 0.01) and for the continuers (p < 0.05)
Insufficient BPRS and LSP scores were available to analyse outcomes for discontinuers.
Clinical status
Clinical status data was not available for two discontinuers at YEAR5. At YEAR3, there was a significant improvement in clinical status for both the cohort and the continuers (p < 0.001); 94% (n = 30) of the cohort and all of the continuers showed moderate or marked improvement and no patient deteriorated. The clinical status of the cohort and the continuers improved further between YEARS 3 and 5 (p < 0.01). Sixty per cent (n = 18) of the cohort and 64% (n = 14) of the continuers reportedly improved after YEAR3 while 13% (n = 4) of the cohort and 4.5% (n = 1) of the continuers deteriorated. The remainder were unchanged.
Hospital and hostel use
The mean number of admissions to hospital per subject per year and the percentage of subjects admitted to hospital for at least 1 day in each year of the study (p < 0.001) (see Table 1) changed significantly over time for both the cohort and the continuers. Significantly fewer of the cohort were admitted to hospital in YEARS 2, 3, 4 and 5, p < 0.05; p = 0.001; p = 0.001; p = 0.001, respectively, than 1 year preclozapine (1 YR PRE). Similarly, significantly fewer of the cohort were admitted to hospital in YEARS 3, 4 and 5 (p < 0.01) than 2 years preclozapine (2 YRS PRE). Significantly fewer continuers were admitted to hospital in YEARS 3, 4 and 5 than in the two years preclozapine (p < 0.01 in each case). There were similar findings for average number of hospital admissions but the lower hospital use for the continuers was statistically significant in YEARS 2–5.
Bed use for psyc hiatric reasons by the cohort, continuers and discontinuers. Percentage (number) of subjects admitted to hospital in each year.
Time spent in hospital (see Table 2) also changed significantly over time for the cohort and continuers (p < 0.001). The cohort spent significantly less time in hospital in YEARS 2, 3 and 4 than in the two years preclozapine, p < 0.05, p < 0.05, p < 0.01, respectively. Also, the cohort showed a non-significant trend towards a shorter stay in hospital in YEAR5 compared to preclozapine (p = 0.067). The continuers spent significantly less time in hospital in YEARS 2, 3, 4, and 5 compared to preclozapine (p < 0.01). There was no significant change in time spent in hospital in YEARS 4 or 5 compared to YEARS 2 and 3, nor in hospitalization time between YEARS 4 and 5 for either the cohort or the continuers.
Hostel use (Table 3) did not change significantly over time for the cohort (p = 0.07). There was a significant change in bed use in the continuers (p < 0.05). They showed a trend towards reduced time in hostels at YEAR5 compared to preclozapine (p = 0.059). The time they spent in hostels was significantly less in YEAR5 than in YEARS 1, 2, 3 and 4 (p < 0.05, p < 0.01 and p < 0.05) but was significantly longer in YEAR 2 (p < 0.05) than preclozapine.
Bed use for psyc hiatric reasons by the cohort, continuers and discontinuers. Median and thir d quartile hospital bed days for each year.
Bed use for psyc hiatric reasons by the cohort, continuers and discontinuers. Percentage of subjects admitted to hostel for at least 6 months in each year.
Treatment costs
Bed costs and costs of treatment are shown in Figure 1. Bed costs changed significantly over time for the cohort and the continuers (p < 0.001) with a significant decrease in bed costs between preclozapine and YEARS 2, 3, 4 and 5 for the continuers (p < 0.05, p < 0.05,(p < 0.05 in each case) and a trend towards decreased bed costs in YEAR3 (p = 0.063) for the cohort. The continuers showed a significant reduction in bed costs in YEAR5 compared with each of YEARS 1, 2, 3 and 4, and bed costs in YEAR4 were significantly less than in YEARS 1 and 2.
Estimated cost (median values; A$’000s) of psychiatric treatment for the cohort, continuers and discontinuers for each year of the study. (a) treatment costs = sum of bed and clozapine use costs; (b) bed costs = sum of hospital and hostel bed costs. ♦, cohort; ▪, continuers; ▴, discontinuers.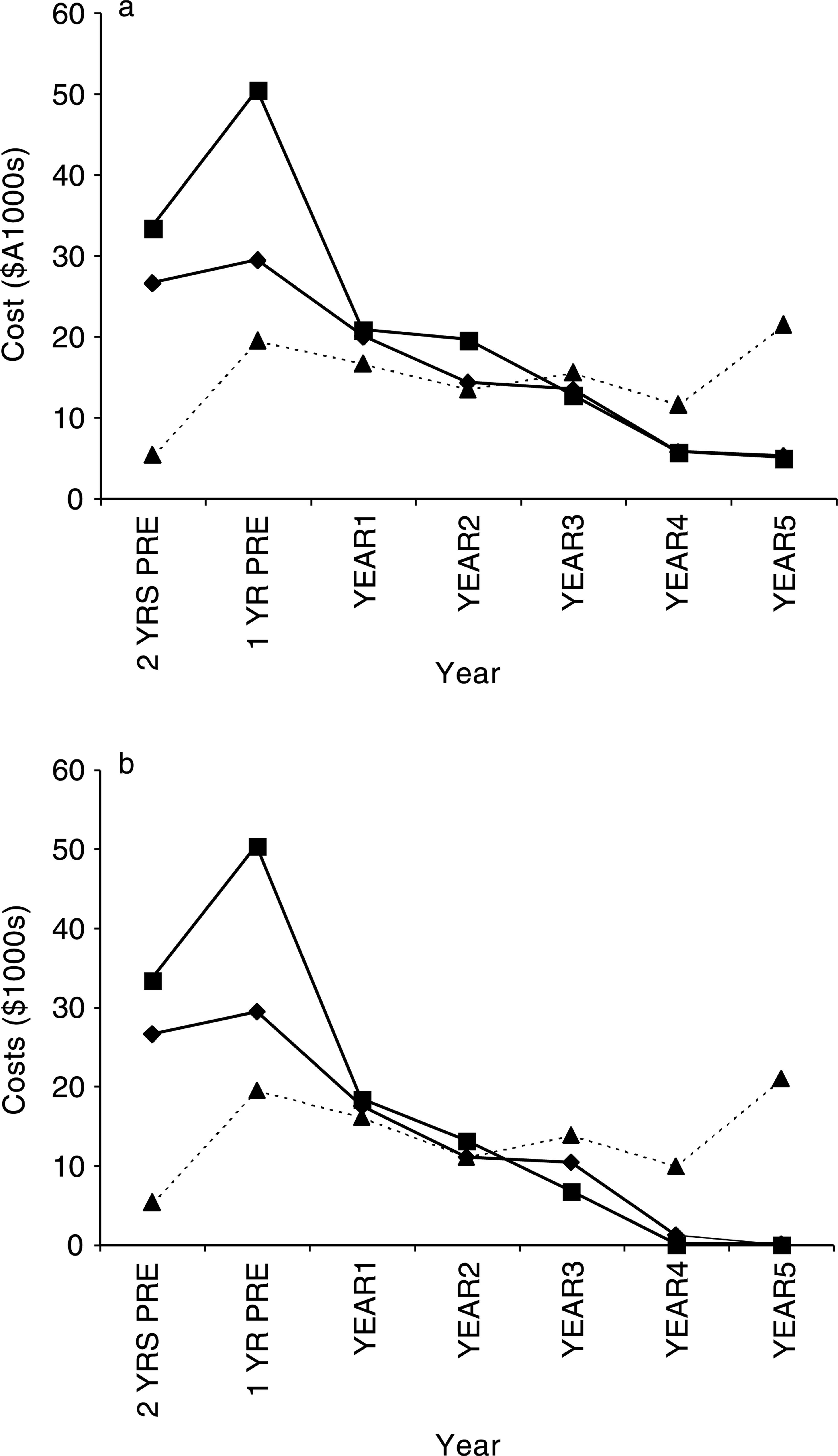
Compared with preclozapine, treatment costs decreased in YEAR5 for the cohort (p = 0.052). The median of the difference between the annual preclozapine treatment costs and the YEAR5 postclozapine costs for the cohort was $10 250 (35% of median preclozapine combined costs for the cohort). Also, the treatment costs for the cohort were significantly lower in YEAR5 than in each of the YEARS 1, 2 and 3 (p < 0.01, p < 0.05, p < 0.05). The treatment costs for the continuers in YEAR5 were significantly less than preclozapine (p < 0.01), and for YEARS 1, 2 and 3 (p < 0.001, p = 0.01, p < 0.001). The median of the difference between the annual preclozapine combined costs and the YEAR5 costs for the continuers was $11 845 (36% of median preclozapine treatment costs for the continuers).
Living circumstances and employment status
Significantly fewer continuers were institutionalized after 5 years of clozapine use than prior to commencing clozapine (p < 0.05), but there was no significant effect on institutionalization for the cohort. Significantly more of the cohort and the continuers were employed or studying at YEAR3 than preclozapine but at YEAR5 employment status had declined to baseline levels.
Side-effects
Four subjects were withdrawn from clozapine because of severe side-effects and six subjects became non-compliant predominantly because of side-effects. There were no fatalities from side-effects or toxicity, and there were no suicides.
Outcomes: discontinuers
Three discontinuers spent long periods in hospital. Patient A improved for almost 4 years, he then developed cardiomyopathy; clozapine was withdrawn and his psychiatric condition deteriorated. He did not respond to other treatments. Patient B improved markedly while on clozapine for almost 4 years. He then developed a cardiac arrhythmia, clozapine was withdrawn and he relapsed to his prior state. He did not respond to other treatments. However, after YEAR5, with close cardiac monitoring, he recommenced clozapine with moderate improvement. Patient C stopped clozapine after a year without benefit but did not respond to other treatments. He showed moderate improvement during YEAR5 after clozapine was recommenced.
The clinical status in 50% of the (8) discontinuers for whom data was available was reported to have improved slightly or moderately between YEARS 3 and 5. This was not statistically significant.
For discontinuers there was no significant change in the mean number of admissions to hospital each year as time progressed. Neither hospital nor hostel bed use changed significantly across time. There was no significant change in bed costs, treatment costs (the median of the difference between preclozapine total costs and post clozapine costs was −$1325), employment status or living circumstances over time.
Comparisons between discontinuers and continuers
There was no evidence that discontinuers were more impaired, or spent more time than continuers in hospital or in hostels in the two years prior to clozapine. However, in YEAR5 a smaller percentage of continuers than discontinuers were admitted to hospital (p < 0.01), and continuers were admitted to hospital less frequently (p < 0.05) and spent significantly less time in hospital than discontinuers (p < 0.05). There was a tendency (p = 0.058) for bed costs to be higher for discontinuers than continuers. There was no statistical difference between continuers and discontinuers in other outcome measures at YEAR5 (clinical status, hostel bed days, treatment costs, employment status and living circumstances). Other than greater clinical improvement and a smaller percentage of hospital admissions in YEAR3 in continuers, there were no significant differences between continuers and discontinuers in YEARS 1–4.
Discussion
The characteristics of our sample and the level of improvement reported, are comparable with those reported in other short-term and long-term studies of clozapine [2, 5, 6, 8, 9].
Over three-quarters (32) of all the patients who were prescribed clozapine for treatment-resistant schizophrenia (eligible for inclusion in the study) were followed up for five years and at the end of five years, over two-thirds continued taking clozapine and had clinical improvement, improved life skills, reduced hospital admissions and time in hospital, a trend towards lower hostel use, and savings in bed and treatment costs. Patients on clozapine showed clinical improvement and a reduction in bed costs, and decreased treatment costs, between the third and fifth years after commencing clozapine. Compared to the preclozapine period, the whole (intent to treat) cohort demonstrated improved or a trend towards improved clinical status and life skills, reduced hospital admissions and length of stay, and bed and treatment cost savings with evidence of clinical improvement, and reduced treatment costs, between the third and fifth year post clozapine. As a group, discontinuers showed no cost savings or improvement in outcome measures, although there was a trend toward some clinical improvement.
These results suggest that there is both continuing clinical benefit and a cost benefit (approximately onethird, $12 000 per annum per patient, of the median preclozapine costs) associated with the long-term use of clozapine. Notably, during YEAR4 and YEAR5 over half of the hostel beds in the ACT were closed. It is not possible to determine whether the reduction in available hostel beds led to less use of them by the continuers or whether improvement in the continuers led to bed closures. There were no suicides in any subject in the cohort. This is consistent with the suicide saving property attributed to clozapine by others [21–23], but see 24.
As noted previously [7], and see [16–18], it is difficult to gain useful information about the clinical value and economic impact of long-term clozapine use in community practice. Arguably, long-term double-blind trials of clozapine in community practice are both impractical and unethical, and if obtained, the direct relevance of their results to usual clinical practice would be questionable. The best approach may be to combine the results from a multiplicity of sources [25].
General and specific problems associated with the methodology of this study (failure to make any assessment of community treatment costs, reliance on subjective retrospective judgements by treating psychiatrists and the absence of an appropriate control group) are acknowledged. Nevertheless, we believe our findings contribute to the understanding of the outcomes of long-term clozapine use and merit consideration by persons making clinical judgements about the use of clozapine. The fact that our results are consistent with those of briefer, better controlled studies gives them added credibility.
Conclusion
This study is one of only a few documenting outcomes of the long-term use of clozapine in clinical practice in the community. The results suggest that clozapine is a valuable treatment option for community practice with long-term clinical and cost benefits, some of which may increase for up to 5 years. However, we acknowledge that the evidence is subject to criticism and other longterm prospective studies (with a comprehensive range of outcome measures) of the use of clozapine are urgently needed.
Footnotes
Acknowledgements
We thank Keith Dear of the Centre for Mental Health Research for statistical advice and the Canberra Hospital Private Practice Fund for support of the 3 year follow-up component of the study.
Declaration of interest: Novartis Pharmaceuticals Australia covered costs ($500) associated with data collection by the first author.