
Abstract
Introduction
Following Cade's original work 50 years ago supporting the role of lithium in the treatment of ‘psychotic excitement’, now recognized as Bipolar Affective Disorder (BAD) [1], lithium carbonate has become a widely used pharmaceutical. However, despite Cade's original observations of the risks of toxicity due to therapeutic lithium, and half a century of clinical experience and research providing us with an increasingly detailed understanding of the pharmacokinetics of lithium, patients are still suffering toxicity. As lithium is a widely used drug, estimated by some studies to be administered to 1.5%% of some populations, the potential burden of illness due to lithium poisoning is great [2].
When considering the severity of lithium toxicity, most texts refer to neurological, gastrointestinal, cardiac, and renal manifestations as well as the serum lithium concentration, although there is little to document a relationship between any of these and any objective measure of morbidity. While some authors have suggested that serum lithium correlates closely to severity of toxicity at least in chronic poisoning, most accept that the relationship is not close and that lithium levels have a very limited role in the assessment of a poisoned patient [3]. We proposed that the severity of neurotoxicity most strongly reflects the burden of illness, and that severity of neurotoxicity would correlate to objective measures of morbidity such as length of hospital stay.
In considering the factors contributing to the development of lithium toxicity, recent therapeutic guidelines state: ‘The most important causes of lithium toxicity are interactions with thiazide and loop diuretics, nonsteroidal anti-inflammatory drugs or angiotensin converting enzyme inhibitors, and reduced fluid intake, fluid loss from vomiting, diarrhoea or excessive sweating. Toxicity may also be caused by deliberate or inadvertent overdose.’ [4]
Some authors also consider renal impairment and chronic conditions associated with salt depletion and volume contraction as potential risk factors [5]. We know of no objective assessment of the relative contribution of any of these factors to the development of toxicity or to the burden of illness due to lithium toxicity. Furthermore, the relative dangers of various modes of poisoning with lithium (i.e. acute overdose, chronic ‘therapeutic’ intoxication) have not been adequately explored, and many basic texts appear to consider them as posing roughly equivalent risk for the development of serious toxicity [6].
We proposed that chronic poisoning was far more likely to result in severe lithium toxicity, reflected as severe neurotoxicity. We further proposed that the presence of identifiable factors known or expected to impair lithium excretion would be associated with an increased risk of chronic poisoning.
Methods
Data collection
Case records for all cases presenting to a regional poisons centre from 1987 until June 2000 were identified using the clinical database described in previous papers [7]. The database was searched for cases presenting following acute overdosage of lithium or with lithium toxicity. Each chart was then individually reviewed.
Classification of mode of poisoning and severity of toxicity
Cases were classified as acute poisoning (acute ingestion of lithium in a patient not currently taking lithium), acute on chronic poisoning (acute ingestion of lithium in excess of prescribed dose in a patient currently receiving chronic lithium therapy), or chronic poisoning (no acute ingestion, patient presenting with signs and symptoms of lithium toxicity in the context of chronic therapeutic administration of lithium).
Severity of neurotoxicity was based on information in the clinical record, and was rated as nil, mild, moderate or severe, based on the rating scale described in Hansen and Amdisen's original article [8]. In practice, patients were classified as severe if they were delirious, or were physically incapacitated by neurological symptoms attributable to lithium toxicity.
Risk factors for severe neurotoxicity
In addition to factors traditionally thought to result in severe toxicity such as serum lithium concentration, the dose in an acute ingestion, concurrent use of drugs impairing lithium excretion and serum creatinine, we recorded other parameters we considered likely to predispose an individual to severe toxicity through reducing lithium clearance (Fig. 1). The effect of mode of poisoning as a specific risk factor was evaluated.
Factors impairing renal lithium excretion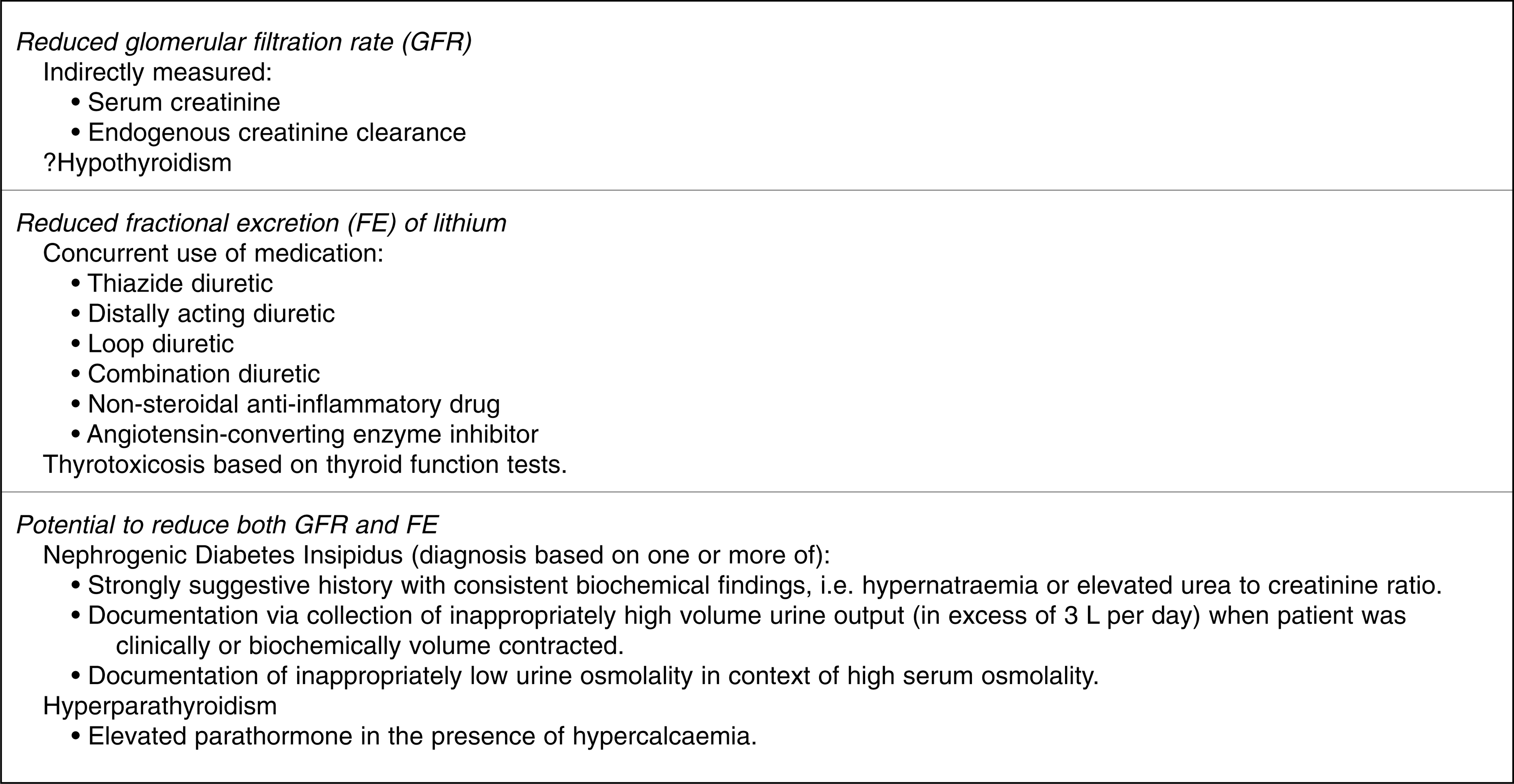
Endogenous creatinine clearance (ECC) in mL/min was calculated using the Cockroft-Gault formula [9]. A worst and best ECC were calculated for each case, according to peak and lowest recorded serum creatinine. The latter value was considered to represent a measure of the patient's baseline renal function in the absence of a serum creatinine from the previous 12 months.
Abnormalities of thyroid function were assessed according to disturbances of thyroid function tests if these were available. Thus a biochemical diagnosis of hypothyroidism or hyperthyroidism was made, rather than a clinical diagnosis.
Nephrogenic diabetes insipidus (NDI) was considered present if a case had strong clinical and biochemical evidence of this diagnosis (Fig. 1).
Although hyperparathyroidism was not prospectively identified as a potentially important factor, its presence was noted in a number of patients. We defined this condition on biochemical findings of elevated parathormone in the context of elevated serum ionized calcium (i.e. biochemical criteria for primary or tertiary hyperparathyroidism).
Outcomes
Duration of stay in hospital and the intensive care unit were recorded in days and hours, respectively. Death and the use of haemodialysis were the other outcomes recorded.
Analysis
Median length of stay and peak serum lithium concentration for severe neurotoxicity and other neurotoxicity groups combined were compared using the Mann-Whitney test; two-tailed P-values were obtained. The association between severe neurotoxicity and each mode of poisoning was assessed using an unadjusted odds ratio with 95%% confidence interval.
Patients with chronic poisoning were compared to patients with acute or acute on chronic poisoning. Unadjusted Odds Ratios (OR) with 95%% confidence intervals (CI), chi-square and P-values were determined for the following nine variables; gender, age, weight, creatinine at baseline, creatinine clearance at baseline, peak serum lithium, presence of drugs affecting lithium clearance, presence of biochemical thyroid dysfunction and presence of diabetes insipidus.
A logistic regression model was developed initially using six univariate significant independent variables and using chronic poisoning as the response variable. The initial independent variables were; age, creatinine at baseline, creatinine clearance at baseline, presence of drugs affecting lithium clearance, presence of thyroid dysfunction and presence of nephrogenic diabetes insipidus. A forward stepwise logistic regression model was used. Odds ratios were calculated using parameter estimates from logistic models and removal of nonsignificant variables from the multivariate models was based on P-values < 0.05. There was no examination of possible interaction effects.
Data analyses were done using SPSS release 10.0.0 (24 September 1999 SPSS inc. Chicago, Illinois).
Results
One hundred and eight cases were identified in the database. 11 cases were excluded from analysis; records of four cases revealed no evidence of any exposure to lithium, and seven case files were not located. None of the seven cases had a length of stay greater than 2 days. No deaths related to lithium were recorded.
Validity of severity of neurotoxicity as a measure of burden of illness
Median length of stay for cases rated as ‘severe neurotoxicity’ was 12 days (range 3–34 days), significantly different to the median length of stay for cases not suffering severe neurotoxicty (2 days, 1–17) (P < 0.001). If admitted to the intensive care unit, cases with severe neurotoxicity had a much longer length of stay (135 h, range 8–382) than those without (35 h, range 14–124) (P = 0.02). It is noteworthy that for all cases who developed severe neurotoxicity at any time, the severity of neurotoxicity was apparent on initial assessment of the patient. As no cases died, and only seven received haemodialysis, no statistical analyses were performed on these outcomes. Of the seven cases who were dialysed, five presented with chronic poisoning and two with acute on chronic poisoning. All five chronic cases receiving dialysis suffered severe neurotoxicity, compared to only one of the acute on chronic cases. The remaining case dialysed for acute on chronic poisoning developed only mild neurotoxicity, despite a serum lithium of 7.48 mmol/L.
Risk of severe neurotoxicity
Chronic poisoning was the factor most strongly associated with the development of severe neurotoxicity, with an odds ratio of 136.5 (95%% CI 23–1300). Conversely, both acute (OR < 0.01, 95%% CI 0.00–0.58), and acute on chronic poisoning (OR 0.03, 95%% CI 0.01–0.16), were negatively associated with severe neurotoxicity.
Of the 28 cases of severe neurotoxicity, 26 occurred in the context of chronic poisoning. The remaining two cases suffered acute on chronic poisoning: one was a 75-year-old man with nephrogenic diabetes insipidus and a best ECC of 27 mL/min; the other was a 49-year-old woman who was taking a NSAID, and had a markedly elevated creatinine on arrival. They presented at 72 and 48 h post ingestion, respectively.
Peak serum lithium concentration was significantly higher in those with severe neurotoxicity compared to those not suffering severe neurotoxicity (2.3 vs. 1.6 mmol/L, P = 0.01).
Risk of developing chronic poisoning
See Table 1. For univariate analyses there was no significant association with chronic poisoning for gender, weight, or peak serum lithium concentration when compared to any other mode of poisoning.
Unadjusted and Adjusted Odds ratios for variables associated with Chronic Lithium Poisoning
When unadjusted odds ratios were calculated, older age, all measures indicating impaired renal function, presence of NDI, abnormalities of thyroid function and recent coadministration of drugs affecting lithium clearance were all significantly associated with chronic poisoning (Table 1).
A logistic regression model showed a three factor solution, independently associated with the development of chronic poisoning. These factors were NDI, age over 50 years and thyroid dysfunction. Abnormal baseline creatinine clearance was significant at the P = 0.05 level (Table 1).
Three patients suffering chronic poisoning were noted to have hyperparathyroidism causing significant hypercalcaemia.
Discussion
Our results support the assertion that severe lithium induced neurotoxicity almost invariably develops in the context of chronic therapeutic administration of lithium, and rarely results from an acute overdose. This mode of poisoning occurs due to the presence of identifiable risk factors known to impair lithium excretion.
Clinical severity of neurotoxicity as a measure of burden of illness
Whilst lithium has been considered to cause toxic effects on a variety of organ systems including the heart, gut and kidney [2], [4], central nervous system (CNS) effects consistently cause the most significant morbidity. This toxicity can be permanent [10–12] and may occur even when serum lithium remains in the therapeutic range [13–15].
In our experience, all cases of severe neurotoxicity were evident at the time of admission, and no cases appeared to deteriorate significantly during the course of treatment. The correlation between severity of neurotoxicity on arrival and length of stay provides validity for this as an index of the burden of illness. Cases of severe neurotoxicity had higher peak serum lithium concentrations; this is in agreement with most major texts and current clinical thinking. However there was substantial overlap in the range of peak serum levels for the two groups and so no clinically obvious serum level was apparent that would safely distinguish groups.
Chronic poisoning as the principal cause severe neurotoxicity
Hansen and Amdisen's original article in 1978 [8] noted that cases of chronic poisoning appeared more likely to suffer severe and protracted illness due to lithium poisoning, and other authors have noted a higher risk of toxicity in those cases suffering ‘therapeutic intoxication’ [16]. Chronically elevated concentrations of lithium should be more likely to cause neurotoxicity than transient elevations, as lithium distributes slowly into the CNS [17]. From our data it would appear that acute overdose of lithium in individuals without impaired clearance of the drug appears relatively safe, at least as far as neurotoxicity is concerned. As noted in the results section, both cases who developed severe neurotoxicity due to acute on chronic poisoning appeared to be at high risk due to the presence of factors reducing lithium clearance. Since the majority of severe cases occurred in the absence of an overdose of lithium, the development of such high levels would appear to reflect a failure of therapeutic monitoring. A recent report has suggested that standards of monitoring lithium are generally poor [18].
Risk factors for chronic poisoning
Lithium excretion has been well characterized since 1968 [19]. Essentially, lithium is freely filtered at the glomerulus and avidly reabsorbed in the proximal convoluted tubule, such that the clearance is usually 20–30 mL/min. Thus lithium clearance is proportional to glomerular filtration rate (GFR), and may be expressed as a percentage of the GFR (normally 25%%) sometimes referred to as the Fractional Excretion of lithium (FE Li). Factors decreasing either GFR or FE Li, will reduce lithium clearance; if both are affected the reduction will be compounded.
Serum creatinine and ECC
Whilst it is debated whether or not lithium induces any permanent decrement in GFR [2], [20], decrements in GFR from any cause affect lithium excretion. From our results it appears any decrement in creatinine clearance represents a significant risk for that individual developing chronic poisoning, but that the link between elevated serum creatinine and risk is less certain. Creatinine production is related to lean body mass, which is related to age, weight and gender, such that older, thinner individuals may have substantial decrements in GFR whilst their serum creatinine is only marginally elevated, or at the upper limits of normal. This imprecise link between GFR and serum creatinine reasonably accounts for the stronger association of calculated ECC than serum creatinine with risk of chronic toxicity, and must be considered when assessing an individual patient's risk.
Nephrogenic diabetes insipidus
Nephrogenic diabetes insipidus (NDI) occurs in the context of chronic lithium therapy in an estimated 10%% of cases [21]. To our knowledge it has not been previously considered as a factor contributing to the risk of toxicity, however, NDI has the potential to precipitate rapid and profound volume depletion, with subsequent decrements in both GFR and FE Li. Our data suggest that the presence of NDI poses a considerable risk to patients receiving lithium. NDI may not be readily recognized by medical practitioners in otherwise stable patients.
Effect of thyroid function
Lithium is widely known to affect thyroid function. Whilst it is generally accepted that lithium induces hypothyroidism [22], at least one case series documents a higher than expected incidence of hyperthyroidism in lithium treated patients [23]. Alterations in thyroid function impact significantly on lithium excretion [24]. Hyperthyroidism induces avid tubular resorption of lithium, and subsequently results in a significant reduction in lithium clearance [25]. Interestingly, lithium may alter thyroid hormone receptor binding and potentially mask the signs of thyroid hormone excess [26], such that biochemical markers of thyroid function may be a better indicator of thyroid status than clinical examination.
To our knowledge, hypothyroidism has not been shown to reduce lithium clearance. However hypothyroidism induces a decrement in GFR of around 30%% [27], and this could reasonably be expected to lead to an increased risk of chronic lithium poisoning.
Age
Age over 65 has previously been described as increasing the risk of moderate to severe complications of lithium therapy [28], although other authors contradict this suggestion [13]. The predilection for older patients to develop clinical signs of lithium toxicity is twofold; they are likely to have increased susceptibility to delirium when subjected to the added insult of a neuroactive drug; and they may have impaired excretion of the drug. Comorbidities such as underlying dementia, volume depletion and polypharmacy are more common in the aged, and may additionally increase their risk of delirium [29], [30]. Age remained significantly associated with chronic poisoning when adjusted for the presence of factors reducing lithium clearance, implying that greater CNS susceptibility to the effects of lithium may contribute to this increased risk. Older patients should be considered to be at greater risk of developing chronic lithium poisoning and subsequent severe neurotoxicity. Also, ageing patients, despite being stable on lithium for many years, will become increasingly susceptible to its toxic effects, and need to be monitored more closely than younger patients.
Coadministration of drugs
The interaction between various drugs and lithium excretion is well documented. Most drugs known to impair lithium clearance do so through reducing the FE Li. Thiazide diuretics, predominantly through inducing sodium depletion, induce a decrease in lithium clearance of around 25%% after a week of therapy [31]. Whilst other diuretics have been implicated in cases of lithium toxicity [32–34], there is less evidence that they consistently reduce FE Li [35]. Nonsteroidal Anti-Inflammatory Drugs (NSAIDs) [36], [37] and Angiotensin Converting Enzyme inhibitors (ACEI's) [38] also reduce lithium excretion by around 25%%. Coadministration of drugs known to impair lithium excretion appeared to contribute to the development of chronic poisoning in only a small number of our patients, and did not contribute significantly in the regression model when other factors were controlled. Nevertheless these drugs should only be coadministered to patients taking lithium when there is no reasonable therapeutic alternative, and only then with frequent monitoring of serum lithium levels and the patient's clinical status.
Parathyroid disease
Hyperparathyroidism has been described in association with lithium therapy [39], with an incidence of around three per cent, similar to that observed in our series. Although the risk due to hyperparathyroidism could not be assessed because of small cell sizes, this condition is theoretically likely to contribute to the development of chronic poisoning in a few patients. Hypercalcaemia due to hyperparathyroidism induces an osmotic diuresis, which may then lead to volume depletion and renal salt retention, and thus reduced GFR and FE Li.
Study strengths and weaknesses
Our study has a number of weaknesses to be considered. It is retrospective by design and therefore we compared groups that were not matched for age and other confounders. Nevertheless neither gender nor weight was significantly different in the two groups in univariate analyses, and neither baseline creatinine nor drugs affecting lithium clearance, nor peak serum levels remained significant in the multivariate analyses. Age was a significant independent variable and so matching for this would have eliminated its usefulness as a study variable. There may be other confounders of interest that were not entered into the regression model.
Hypotheses were prospectively generated, whilst the data were retrospectively collected. Many factors were subject to significant measurement bias. Baseline ECC was most often calculated from the lowest recorded serum creatinine during hospital stay, which in some cases may have remained elevated from the effects of the acute illness. The presence of NDI and thyroid disorders was more likely to become apparent during a lengthy hospital stay, especially as few patients appeared to have had any recent thyroid function tests available.
However all the cases included in our study were treated at one regional referral unit comprising only a small number of staff. This conferred a degree of uniformity upon patient assessment and treatment. Finally, no prior study has considered chronic, pre-existent medical conditions as relevant to the development of lithium neurotoxicity, or attempted to attribute weighting to associated factors.
Conclusion
The problem of severe lithium toxicity is iatrogenic, is usually the result of chronic poisoning rather than acute overdose of lithium, and occurs in patients with identifiable risk factors. Close attention to individual susceptibility as reflected by older age, renal impairment, presence of nephrogenic diabetes insipidus and thyroid disease will help to identify those at risk. Hyperparathyroidism, the use of drugs known to impair renal lithium excretion, and other acute illnesses associated with the development of lithium toxicity might be considered as disclosing events that precipitate lithium toxicity in susceptible individuals.
We would suggest that six monthly monitoring of serum lithium, renal and thyroid function must be supplemented with careful clinical assessment of those patients at risk, including specific questioning for symptoms of nephrogenic diabetes insipidus. The possible utility of annual serum parathormone and serum calcium levels should also be considered. Review of existing therapeutic guidelines may be warranted. Finally, it must be remembered that even for patients who have been stable for many years on lithium, their susceptibility will increase as they age.