
Abstract
The Australian National Mental Health Policy has highlighted the impact of society's attitudes to mental health on those with mental disorders [1]. In response to consumers’ concerns about community attitudes, the Commonwealth Government funded a National Community Awareness Program which began in 1995. This program aimed ‘to increase community awareness about mental illness and reduce stigma and discrimination experienced by people with a mental illness and their family and carers’ [2]. More recently, the Commonwealth Government funded a project on attitudes of health professionals in response to ‘the concerns of consumers, carers, and their representatives who identify as an important issue the stigmatising attitudes of some health professionals towards people with mental illness’ [2]. This project has identified a number of areas where the attitudes of health professionals diverge from those of consumers and carers [3]. There have also been efforts to change attitudes from within the health professions. The STIGMA Study Group was founded by mental health professionals and has been active in this area since the early 1990s [4].
While a lot of research has been carried out overseas on public and professional attitudes towards people with mental disorders (e.g. [5, 6, 7, 5–8]), comparatively little has been done in Australia. Apart from two small studies carried out a decade or two ago [9, 10]], the only research consists of unpublished surveys by the Commonwealth government [11, 11, 12]] and the Schizophrenia Australia Foundation [13]. In 1993, the Commonwealth commissioned a study to assess community attitudes [11]. This research entailed a two-stage process: an initial qualitative study involving focus groups and a second quantitative study involving telephone interviews of the general public. The main conclusions of the study were: understanding of mental illness is limited; stress is viewed as the primary cause of mental illness; the incidence of mental illness is seen to be rising, but the personal risk is considered to be minimal; experience of mental illness is reasonably common; perceptions of the outcome of mental illness are bleak; there is interest in learning more about mental illness; and attitudes toward mental illness are reasonably tolerant, but employer attitudes are generally negative. Unfortunately, the methodology of this survey had some major weaknesses. Although the survey involved a national sample, the response rate was only 38%, making any generalisation of the results to the general population hazardous. Another limitation is that the survey asked about ‘mental illness’ as a generic category when it really encompasses great diversity. In 1995, a repeat version of this telephone survey was commissioned and the results were reported to be similar [12]. A national survey was also carried out by the Schizophrenia Australia Foundation in 1991 [13]. This survey examined awareness of schizophrenia; knowledge of the disorder, its symptoms and causes; and attitudes and shame associated with schizophrenia. This survey found a high apparent acceptance and low level of shame associated with schizophrenia, but the authors noted that pressures of social desirability might have affected the responses.
Independently of the work on attitudes emanating from the National Mental Health Policy, we carried out a household survey of public knowledge and attitudes regarding mental disorders in 1995 [14] and a postal survey of health professionals the following year [15, 15, 16]]. It was found that public and professional beliefs about treatment are very different. The responses to the attitude questions form the basis of the present paper.
Method
A household survey was carried out with a nationally representative sample of 2031 Australian adults aged 18–74 in August 1995 [14]. This sample represented a response rate of 85%. Because it was not feasible to do personal interviews with the health professionals, the interview was modified to make a questionnaire for self-completion and mailed out during May/June 1996 [15, 15, 16]]. The survey was posted to all psychiatrists in Australia, a sample of general practitioners (GPs) listed on the national register of medical practitioners (the Medicare Provider File), and all members of the College of Clinical Psychologists. These three professions were chosen for initial study because of the availability of suitable sampling frames. Replies were received from 1128 psychiatrists (75% response rate), 454 clinical psychologists (65%) and 872 GPs (61%).
The questionnaire was based on a vignette of a person suffering from a mental disorder. Half of each group was given a vignette describing a person who met ICD-10 [17] and DSM-IV [18] diagnostic criteria for major depression and the other half were given a vignette of a person who met criteria for schizophrenia. So that responses would be based on the behaviours described rather than on the diagnostic label, the terms ‘depression’ and ‘schizophrenia’ were not mentioned. The sex of the person described was randomly assigned to be either male (‘John') or female (‘Mary').
The depression vignette was: ‘John is 30 years old. He has been feeling unusually sad and miserable for the last few weeks. Even though he is tired all the time, he has trouble sleeping nearly every night. John doesn't feel like eating and has lost weight. He can't keep his mind on his work and puts off making decisions. Even day-to-day tasks seem too much for him. This has come to the attention of John's boss who is concerned about his lowered productivity.'
The schizophrenia vignette was: ‘John is 24 and lives at home with his parents. He has had a few temporary jobs since finishing school but is now unemployed. Over the last 6 months he has stopped seeing his friends and has begun locking himself in his bedroom and refusing to eat with the family or to have a bath. His parents also hear him walking about his bedroom at night while they are in bed. Even though they know he is alone, they have heard him shouting and arguing as if someone else is there. When they try to encourage him to do more things, he whispers that he won't leave home because he is being spied upon by the neighbour. They realise he is not taking drugs because he never sees anyone or goes anywhere.'
Respondents were asked questions about the diagnosis of the person described, the helpfulness of various interventions, prognosis with and without professional help, the person's long-term functioning in various social roles compared to other people, and the likelihood of the person being discriminated against. The respondents were also asked to report their own characteristics. For the public, these questions included age, sex, education and contact with people such as the one described in the vignette. For the professionals, there were questions on age, sex, work setting and how often they deal with problems such as the one described.
In framing attitude questions, we thought it was important to distinguish between attitudes towards the person currently experiencing a mental disorder, and attitudes towards such persons in the long term after they have received treatment. We decided to focus on the latter by asking questions which covered a number of long-term outcomes. The specific attitude questions asked of respondents were: ‘Suppose that John had the sort of help you think is most appropriate for his health problems. How do you think he would be in the long term compared to other people in the community?’ They were then given 10 outcomes, 5 negative and 5 positive, which they had to rate as ‘More likely’, ‘Just as likely’ or ‘Less likely’. The outcomes were: ‘To be violent, To drink too much, To take illegal drugs, To have poor friendships, To attempt suicide, To be understanding of other people's feelings, To have a good marriage, To be a caring parent, To be a productive worker, To be creative or artistic’. Responses of ‘More likely’ were coded as 1, ‘Just as likely’ as 0, and ‘Less likely’ as −1, while more complex responses were coded as missing.
A problem in assessing attitudes using questions of this sort is that some responses might be seen as more socially desirable. In light of this possibility, we also asked a question about whether the person described in the vignette would experience discrimination by others in the community. The question was: ‘Do you think that John would be discriminated against by others in the community if they knew about the problems he has had?’ The possible responses allowed were ‘Yes’ and ‘No’.
Principal components analysis was used to reduce the attitude items to scales. A screen plot was used to determine the number of factors to be subjected to varimax rotation. Differences in mean scores between groups on the attitude items were evaluated using one-way analysis of variance, followed by post hoc Scheffe tests. Differences between groups in frequencies were evaluated using Chi-squared tests. The p < 0.01 level was used for statistical significance.
Results
The sex of the person described in the vignette made no difference to attitudes, so this variable is ignored in the presentation of the results. Mean ratings for various long-term outcomes are shown in Table 1. There were statistically significant differences between the groups for each outcome. Rather than carry out post hoc tests for each of these ratings, we developed summary rating scales as described below.
A principal components analysis was carried out on each of the 10 outcome ratings for each group separately. For the public and for each professional group, two factors emerged: one with high loadings for the five positive outcomes and the other with high loadings for the five negative outcomes. Accordingly, the ratings on the positive and negative items were summed to make separate scales, each having scores in the range −5 to 5, where −5 indicates the outcomes were all rated as less likely and 5 indicates they were all rated as more likely. The correlation between the scales (pooling data from the two vignettes) varied from −0.45 to −0.69 over the four groups.
The means on these attitude scales were calculated for each group and are shown in Fig. 1. There were statistically significant differences between groups on both scales for both vignettes. For the depression vignette, the public rated positive outcomes as more likely and negative outcomes as less likely than did the GPs and the psychiatrists. The clinical psychologists also rated positive outcomes as more likely and negative outcomes as less likely than did the GPs, and they rated negative outcomes as less likely than did the psychiatrists. For the schizophrenia vignette, the public rated positive outcomes as more likely and negative outcomes as less likely than did all three professional groups. Furthermore, the clinical psychologists rated positive outcomes as more likely and negative outcomes as less likely than did the psychiatrists, and the GPs rated positive outcomes as more likely than did the psychiatrists.
Mean ratings for various long-term outcomes for the person described in the vignette
Figure 2 shows the percentage of each group who believed that the person in the vignette would be discriminated against. There were statistically significant differences between the groups. It can be seen that, for the depression vignette, the public and the clinical psychologists were less likely to believe there would be discrimination. For the schizophrenia vignette, the public were less likely to believe there would be discrimination than all three professional groups. There was general agreement that discrimination was more likely for the person described in the schizophrenia vignette than for the one described in the depression vignette.
To see whether public attitudes varied as a function of age group, sex, level of education and contact with mental disorders, the positive and negative outcome scales were compared in various subgroups of the sample. No age group differences were found. Females were more likely to rate positive outcomes for the person in the depression vignette, but there were no other sex differences. There were significant education group differences in ratings of negative outcomes for the person in the schizophrenia vignette, with the better educated rating worse outcomes, although the post hoc Scheffe tests found no differences between pairs of education groups at the p < 0.01 level. If the respondents reported themselves having had a problem such as described in the depression vignette, they rated positive outcomes as more likely. Similarly, if the respondent reported problems such as described in the schizophrenia vignette, they rated positive outcomes as more likely and negative outcomes as less likely. Having family or friends with a problem like that described in the vignette was not associated with attitudes in either direction.
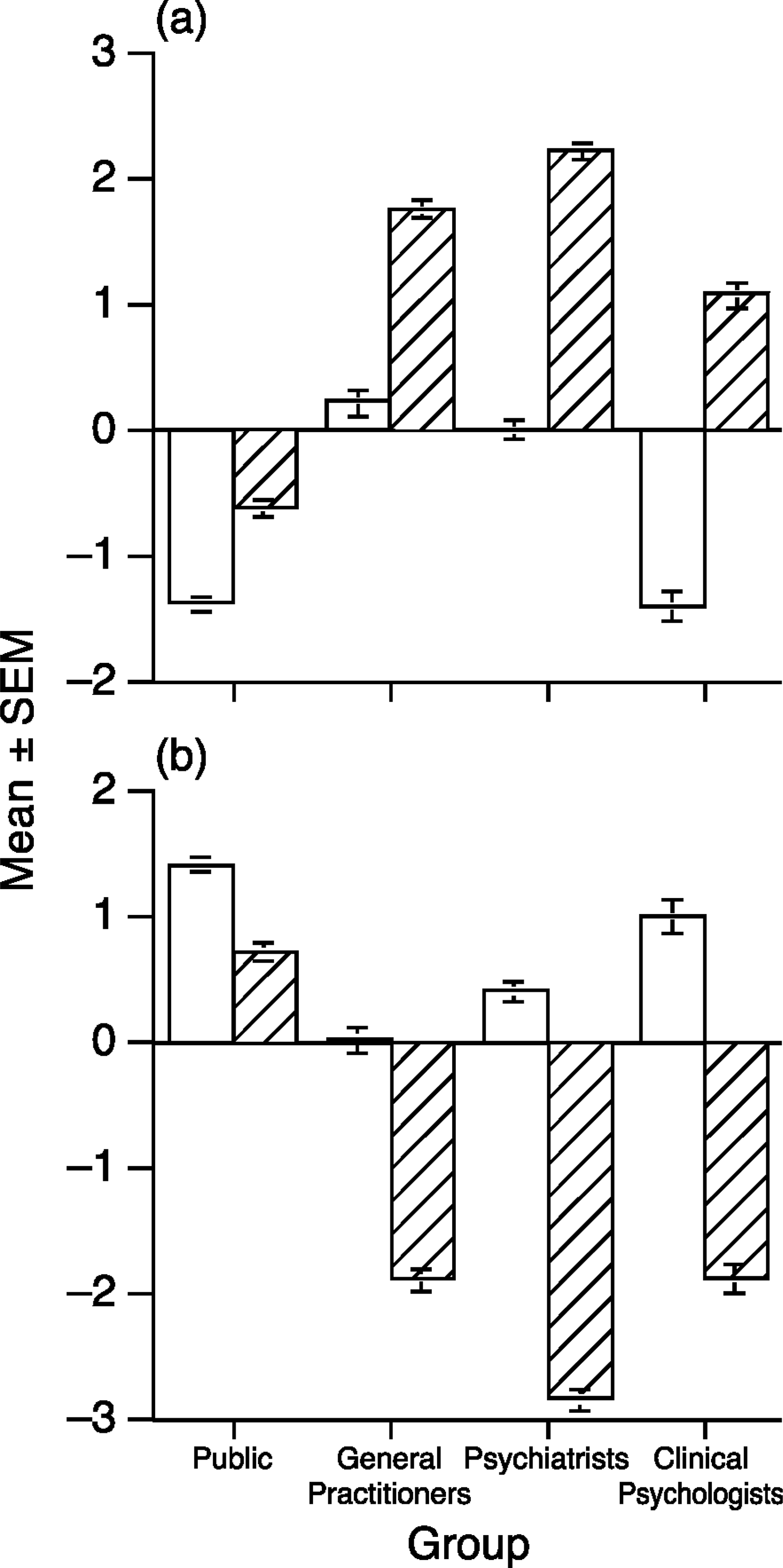
Mean scores on the (a) negative and (b) positive outcomes scales. Scores range from −5 to 5, with a positive score indicating outcomes are rated as more likely and a negative score indicating they are rated as less likely, □ depression; ▪, schizophrenia. Vertical bars represent standard error
A similar set of analyses was undertaken for subgroups of the health professionals. The variables examined were age group, gender, main method of payment for services (private practice, salaried, mixed), and frequency of contact with problems such as the one described in the vignette (daily, weekly, monthly, less than monthly). For GPs, there was a significant effect of age group on ratings of negative outcomes for schizophrenia, with younger GPs making more negative ratings, although post hoc Scheffe tests found no differences between pairs of age groups at the p<0.01 level. Female GPs, who tended to be younger, also rated negative outcomes as more likely for schizophrenia. Similarly, younger psychiatrists rated negative outcomes as more likely for both depression and schizophrenia. There were no age and sex differences for clinical psychologists. Salaried psychiatrists rated negative outcomes as more likely for depression than did private practice psychiatrists. Clinical psychologists in mixed practice rated positive outcomes as more likely for depression than did salaried psychologists. Frequency of contact was not associated with attitudes in any group.
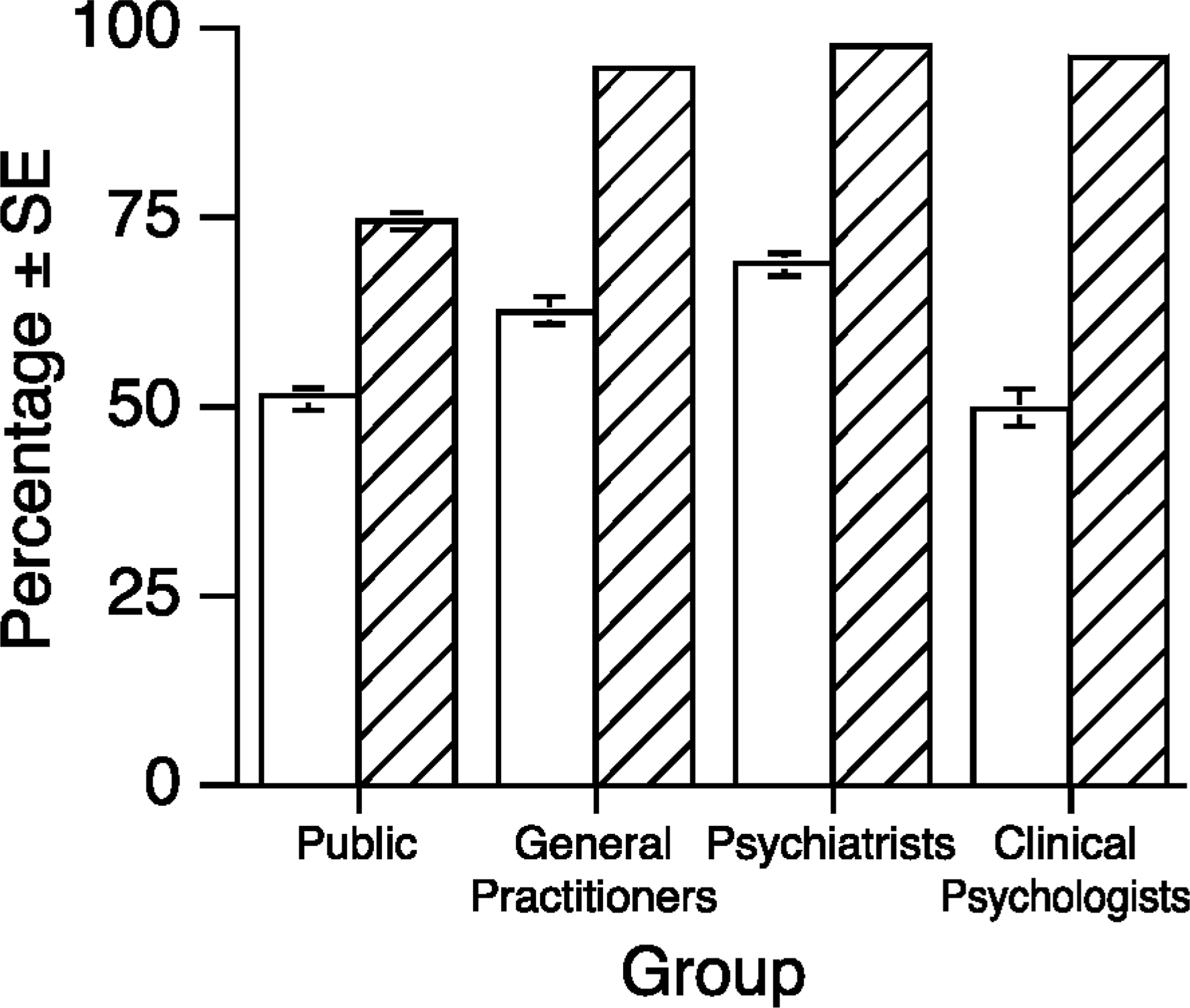
Percentage of each group who believed that the person described in the vignette would be discriminated against. □, depression; ▪, schizophrenia. Vertical bars represent standard error
Discussion
The main finding of this study is that health professionals rate long-term outcomes more negatively than do the public, and they believe discrimination is more likely. The finding is consistent with other results from the same survey which showed that the public are more optimistic than the professionals about the long-term prognosis after treatment [15].
The finding of more negative attitudes of health professionals supports consumers’ and carers’ concerns about this issue [2]. However, in interpreting the findings, we must consider whether the more negative attitudes of health professionals have a basis in reality. Health professionals have much greater contact with mental disorders than the public and might be more realistic in their assessment of long-term outcomes and social discrimination. Indeed, the public responses on long-term outcomes seem rather optimistic in that they tend to rate the persons described in the vignettes as more likely than other people to experience positive outcomes (such as being a productive worker) and less likely to experience negative outcomes (such as abusing alcohol or committing suicide). In contrast, health professionals tend to have greater contact with individuals who have chronic or recurrent problems and this may lead to overly negative attitudes. Whatever the case, health practitioners need to be aware that their attitudes may be more negative than those of the public and to be careful about what expectations they convey to patients and their families. There is evidence that patients who perceive devaluation or rejection by society have a worse outcome [19].
The clinical psychologists had more favourable attitudes than the GPs and psychiatrists, particularly towards the person with depression. We have previously reported that clinical psychologists were also more optimiztic about the prognosis of treated depression [15]. The reason for this difference between the professions is unclear. One possibility is that clinical psychologists have contact with less severely afflicted patients. However, the questionnaire asked about attitudes in relation to a specific vignette rather than about depressed patients in general. Another possible reason is the clinical psychologists’ greater belief in the helpfulness of cognitive-behavioural therapy [16], with its emphasis on changing the patient's life in the long term.
Attitudes are not only individual characteristics, but are also influenced by the culture within healthcare systems. Unfortunately, we collected little data on the health practitioners’ work settings. However, we did find that psychiatrists and clinical psychologists in salaried positions tend to have more favourable attitudes about the outcome of depression. It is impossible to say whether this is because they see more severe patients or is a reflection of the culture in their work setting. It may have been more relevant to collect data on hospital versus community-based work settings rather than on method of payment.
It is relevant to consider possible implications of these findings for efforts to change attitudes. Several findings indicate that greater exposure to people with mental disorders and greater public education may not necessarily lead to more positive attitudes: the professionals were found to have more negative attitudes than the public, having family or friends with a mental disorder was not associated with attitudes in either direction, while a higher level of education was associated with more negative attitudes towards schizophrenia. The effect of age group is also relevant. For the public, there were no age group differences, while with GPs and psychiatrists younger age was associated with more negative attitudes. It is conceivable that this is due to the much greater time accorded to psychiatry and the behavioural sciences in the medical undergraduate curriculum. The one variable associated with more favourable public attitudes was having personally experienced a mental disorder.
The limitations of the findings must be acknowledged. The responses given may have been affected by social desirability, particularly with the public who had to give their responses to an interviewer. Because of such influences, the relative attitude rankings may be more meaningful than the absolute values. For example, attitudes towards the schizophrenia vignette were more negative than towards the depression vignette, showing that the items provide an ordinal ranking. Another limitation was that the questionnaire was designed for the general public and was less suited to professionals because of the small amount of information in the vignettes and the restricted choice of responses allowed. Furthermore, the study did not cover all relevant health professions, notably mental health nurses.
The administrative significance of this study is the unexpected finding that the public view depressive disorder and schizophrenia as considerably more benign conditions than do health professionals. Much, therefore, remains to be done towards having the public appreciate the gravity of both depressive disorder and schizophrenia. For health professionals, and for psychiatrists in particular, their awareness of the adverse prognosis may be realistic. It may nevertheless need to be tempered lest it hamper their own clinical performance.
This study is part of an ongoing program of research. Current work is assessing attitudes in other professional and community groups, and examining the effects of a person's attitudes on the outcome if they have a mental disorder.
Footnotes
Acknowledgements
We thank the Commonwealth Department of Health and Family Services and the Australian Psychological Society for providing the files of professional names and addresses. Mike Bird, Penelope Pollitt and Bryan Rodgers provided helpful advice on the survey. Karen Maxwell assisted with the management of the postal surveys.