
Abstract
Keywords
It has long been recognised that those who meet criteria for clinical diagnosis of mental disorder in population surveys, those who self-identify as having a mental health problem in such surveys and those who use primary or specialist mental health services, comprise three different subgroups of the community. There is only partial overlap between them. Various writers, having explored the overlap and mismatch between these three groups in different countries, have hypothesised reasons for this weak relationship between existence of mental disorder and utilisation of mental health services [1–6].
In the following analysis, this issue is considered from the perspective of the behavioural model developed by Andersen and Newman [7] which identified three categories of predictor variables considered likely to be associated with patterns of health service utilisation: need, predisposing and enabling variables.
Need factors
From a mental health services perspective, Andersen and Newman's need predictor variables cover an individual's self-assessment of having mental health problems, and clinical diagnosis of the individual having such problems. Other relevant health factors would include the individual's level of psychological distress [8]. Zola [9] and Galbaud du Fort et al. [10] have proposed that individuals can accommodate many symptoms of psychological distress for some time without seeking help. It is only when they encounter the added stress of other factors, for example, in work or personal life, that they decide to seek professional help [11]. It has also been reported that increased age is related to higher need for mental health services, although this may result primarily in greater use of general medical services [12,13].
Predisposing factors
Predisposing variables relate to the individual's propensity to use mental health services and attitudes towards receiving mental health care. An individual's propensity to use formal health services for mental health problems is likely to be related to that person's willingness to adopt the sick role and help-seeking behaviour [14,15]. Analyses of general help-seeking behaviour indicate that women are more willing to undertake such help-seeking actions [12]. Those with fewer psychosocial assets or with existing physical health problems are also more likely to seek mental health help from the formal health-care system [11,12], as are those with previous experience of formal mental health care [15]. Others may use mental health services to enable them to achieve greater human potential [16,17].
Individual attitudes towards receiving formal mental health care are likely to be related to views concerning whether such treatment is required, the value of such treatment and whether the individual may be stigmatised as a result [18,19]. Some with mental disorders may consider their symptoms to be normal experiences [20], while others may rate various self-help and coping strategies as more useful than professional help for such problems [21,22].
Enabling factors
These factors include organisational factors affecting the affordability and availability of mental health services. Cost of services to the individual will be reduced should they have health insurance [3,23]. In Australia, individuals are reimbursed for general practitioner and psychiatrist visits under the universal health insurance scheme, Medicare, whereas services provided by privately practising psychologists and counsellors are not covered by this system. Services from such practitioners as social workers or drug counsellors are likely to be provided by professionals in community-funded positions at no cost to the individual.
Equitable provision of health care in all regions, metropolitan, rural and remote, is a difficult task for governments in Australia and various other countries [13]. Individuals will also perceive barriers to use of mental health services if those services are not provided in a culturally appropriate manner or in the individual's usual language [5]. Other relevant enabling factors include the individual's awareness that such services exist and understanding of the assistance such services might provide. These factors may relate both to the individual's level of education and the extent of their social networks [2,5].
Inequalities in the use of mental health services in Australia
Various writers who have explored the applicability of Andersen's behavioural model to mental health care utilisation have found that need factors override predisposing and enabling factors in explaining levels and patterns of utilisation of mental health services [24,25]. Inequalities in the availability and affordability of such services across different population groups are indicated when sociodemographic factors are found to be related to utilisation levels over and above the prevalence of mental disorder in those groups. In a fair, equitable health-care system, rates of service utilisation by different population groups should be determined only by the morbidity levels of those groups.
In Australia, it has been difficult to estimate levels of utilisation of mental health services and to identify sociodemographic factors related to levels of utilisation while controlling, at the same time, for mental disorder prevalence levels. To date, few reports have addressed this issue [26]. This shortfall has now been partly addressed by the completion of the National Survey of Mental Health and Wellbeing. This survey of a representative sample of Australians aged 18 and over, living in the community, was conducted in 1997 by the Australian Bureau of Statistics (ABS). Information collected included sociodemographic, physical and psychological health measurements, levels of utilisation of general and specialist medical services for treatment of mental health problems and satisfaction with such services. Access to this data has allowed us to explore sociodemographic and psychological factors associated with using different types of health services for treatment of mental health problems in the Australian setting. In this paper, factors associated with utilisation levels are considered both separately and in combination, allowing us to identify sociodemographic factors contributing to utilisation levels, while controlling for mental health status. The results of these analyses are reported in this paper.
Methods
The National Survey
The National Survey was conducted throughout Australia in 1997. The survey sample comprised residents of private dwellings and participation was voluntary [27]. Approximately 13 600 dwellings were approached with one person aged 18 years or over in each dwelling randomly chosen to participate. In total, 10 641 persons completed the survey interview giving a response rate of 78%.
Sociodemographic details collected from each participant included age, sex, marital status, household structure, languages used, level of education attained and labour force details. General measures of mental health and wellbeing included the 12-item General Health Questionnaire (GHQ) [28] and the Neuroticism scale of the short form of the Revised Eysenck Personality Questionnaire (EPQ-R) [29]. The reliability and validity of these instruments have been previously confirmed [30]. Participants were asked about their having any of 12 chronic physical conditions. Self-reported levels of disability associated with mental health problems were also collected.
Detailed information on the mental health of each individual was obtained using the Composite International Diagnostic Interview (CIDI), a computerised version of which, including diagnostic algorithms, was developed for this survey. Numerous studies have examined the reliability and validity of the CIDI [31], while others have raised concerns about the potential for this instrument to provide overestimates of the prevalence of mental disorders in the community [32]. After completing the CIDI, participants were asked to identify the self-reported health problem that troubled them the most, allowing identification of those whose main self-identified health problem was a mental health problem. Finally, participants were asked about their use of health services.
For those self-identifying as having mental health problems (for example, months of worry or periods of sadness), information on types and levels of health services obtained for any mental health problem was collected. Other writers have found self-report of using or not using medical services to be a valid measure, although frequency of use in a short period may be less valid [Marshall RP: unpublished data]. This is not of concern in this analysis since the principal statistical tool used was logistic regression, with the dependent variable being whether or not the participant reported any utilisation of different types of health service.
Our main foci for self-diagnosed mental disorder, CIDI-diagnosed mental disorders and health service utilisation, were the common mental disorders of affective disorder, anxiety and substance abuse. Participants were classified as having clinically diagnosed affective, anxiety or substance abuse disorders if they were given one or more of the relevant ICD-10 codes. These broad categories of mental disorder were selected over more specific diagnoses since many of the latter have low prevalence rates and high comorbidity with other diagnoses in the same category, thereby limiting their usefulness in analyses of community-based surveys. Finally, each participant's survey information included weighting factors provided by the ABS. These factors gave survey estimates conforming to independent estimation of the Australian population during the time of the survey and allowed reliable, population-level estimates of variables to be calculated.
Statistical analysis
Preliminary statistical analysis gave levels of self-identified mental health problems, CIDI diagnoses and health service utilisation. The four categories of mental health services considered were those provided by: general practitioners, psychiatrists, psychologists, other health service professionals, and a fifth category, services provided by any of these practitioners. The category of ‘other health professionals’ covered drug and alcohol counsellors, other counsellors, nurses, mental health teams, chemists and ambulances.
Using logistic regression analysis, 21 predictor variables (listed in Table 1) including sociodemographic measures, psychological measures, self-identified mental health problems and CIDI-diagnosed mental disorders were entered separately, and then simultaneously, to obtain measures of associations between these factors and use of the five different categories of formal mental health services. Logistic regressions were used when the dependent variable had only two values (for example, whether or not a mental health visit to a psychiatrist was reported). Simple logistic regression estimates the magnitude of association between that dependent variable and a single predictor variable (for example, education level), and multiple logistic regression provides estimates of associations between the dependent variable and each of a number of predictor variables. Simultaneous multiple regression allows us to measure the association between the dependent variable and sociodemographic variables, for example, education, while controlling for any differences in mental health status between those with different levels of education. Standard errors of prevalence estimates and confidence intervals around odds ratios were derived using the statistical package STATA Release 5 [33].
Use of formal health services for mental health problems: predictor variables in the regression analyses
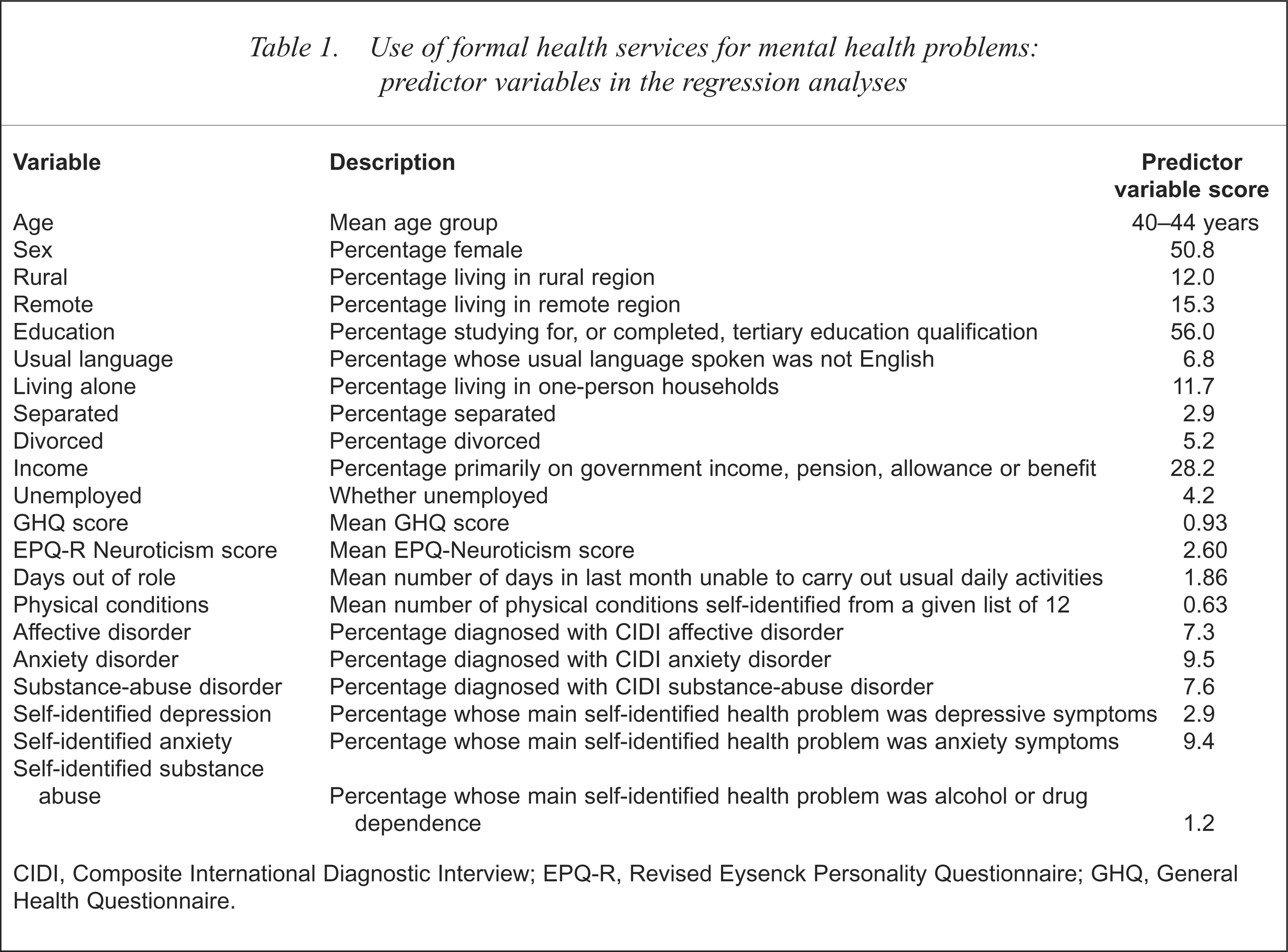
CIDI, Composite International Diagnostic Interview; EPQ-R, Revised Eysenck Personality Questionnaire; GHQ, General Health Questionnaire.
Results
Table 2 shows the percentages of those with self-diagnosed mental health problems and with CIDI-diagnosed mental disorders who reported using various categories of formal services for mental health reasons. General practitioners provided most mental health services, with 76% of those receiving any mental health care reporting obtaining services from this group. As expected, levels of service use for those with self-diagnosed mental health problems or with CIDI-diagnosed affective or anxiety disorders were considerably higher than for the population as a whole. Tables 3–7 give the results of the simple and simultaneous multiple logistic regressions. Tables 8 and 9 summarise the patterns of significant associations found from these analyses.
Percentage of those with self-diagnosed or CIDI-diagnosed mental disorders using formal health services by type of disorder
Odds ratios for associations between sociodemographic and psychological measures and reporting mental health-related visits to a general practitioner
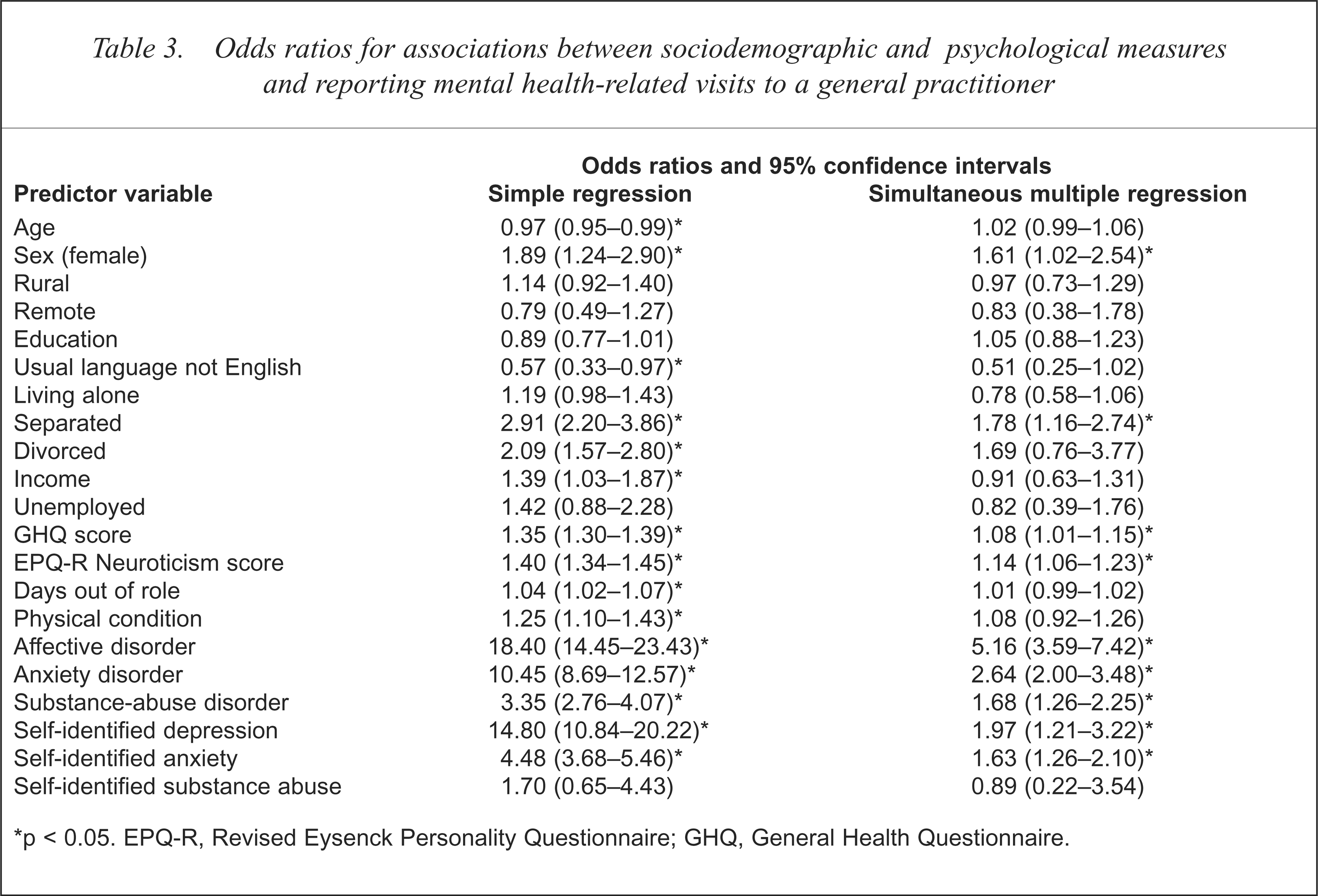
p < 0.05. EPQ-R, Revised Eysenck Personality Questionnaire; GHQ, General Health Questionnaire.
Odds ratios for associations between sociodemographic and psychological measures and reporting mental health-related visits to a psychiatrist
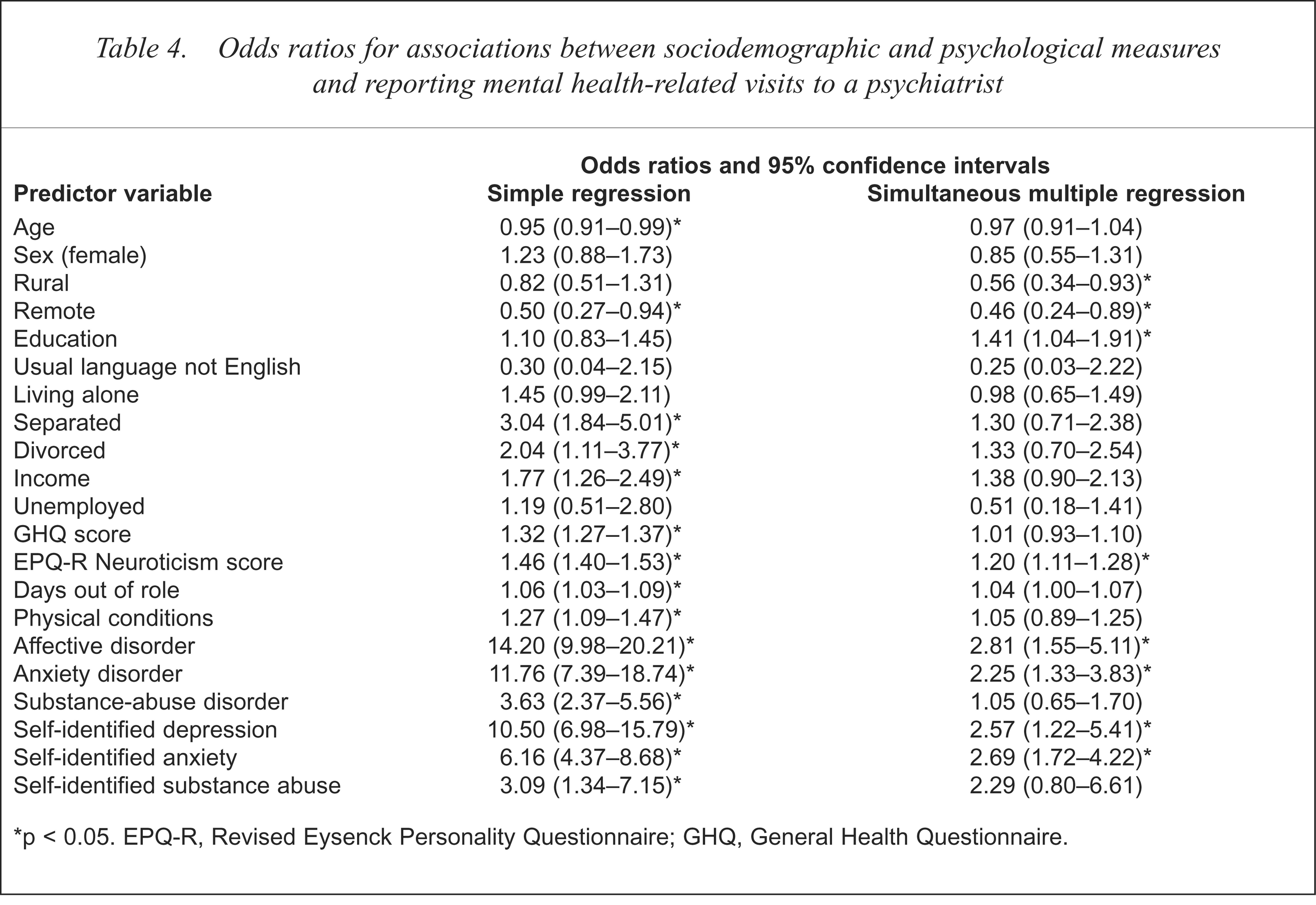
p < 0.05. EPQ-R, Revised Eysenck Personality Questionnaire; GHQ, General Health Questionnaire.
Odds ratios for associations between sociodemographic and psychological measures and reporting mental health-related visits to a psychologist
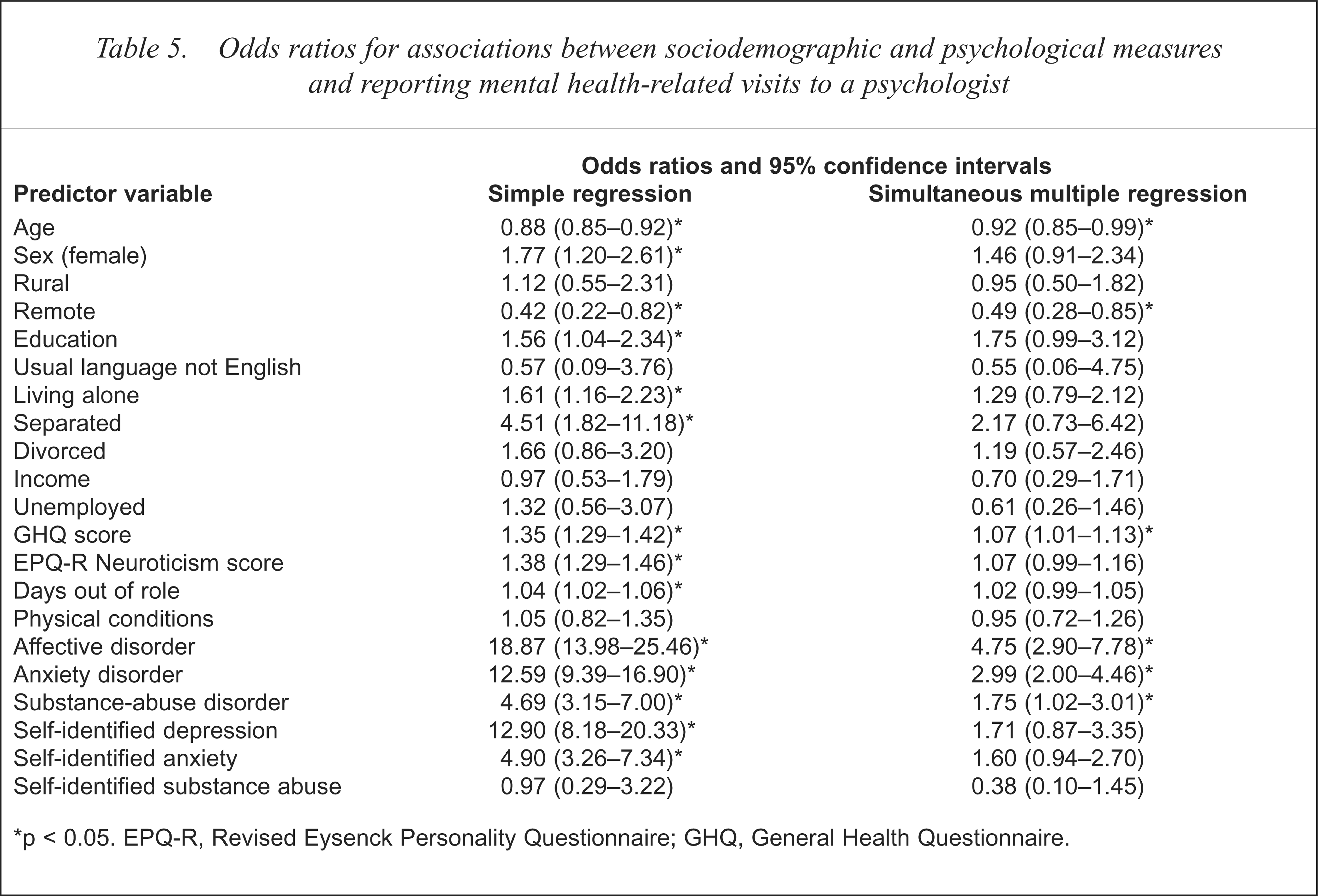
p < 0.05. EPQ-R, Revised Eysenck Personality Questionnaire; GHQ, General Health Questionnaire.
Odds ratios for associations between sociodemographic and psychological measures and reporting mental health-related visits to any other health professional
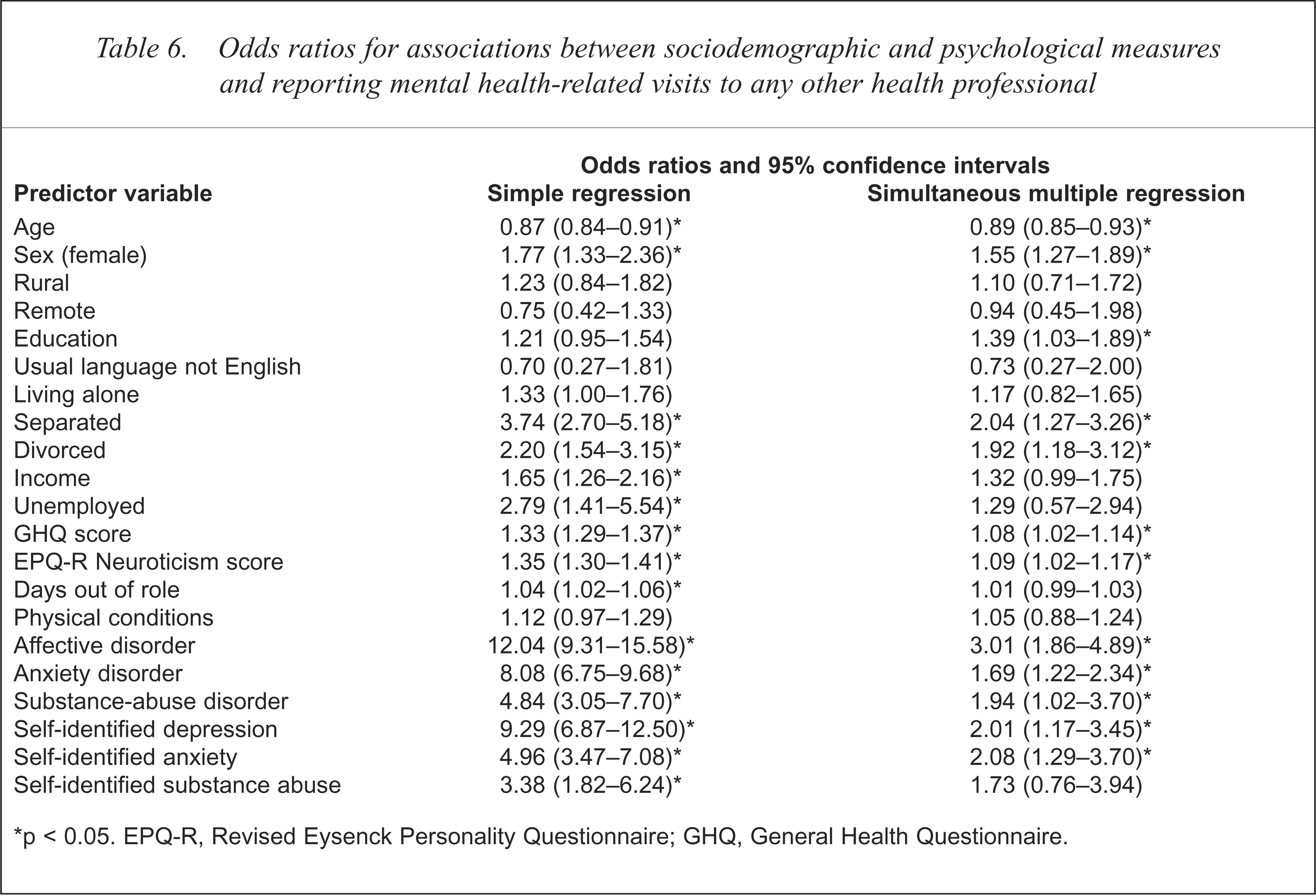
p < 0.05. EPQ-R, Revised Eysenck Personality Questionnaire; GHQ, General Health Questionnaire.
Odds ratios for associations between sociodemographic and psychological measures and reporting mental health-related visits to any health professional
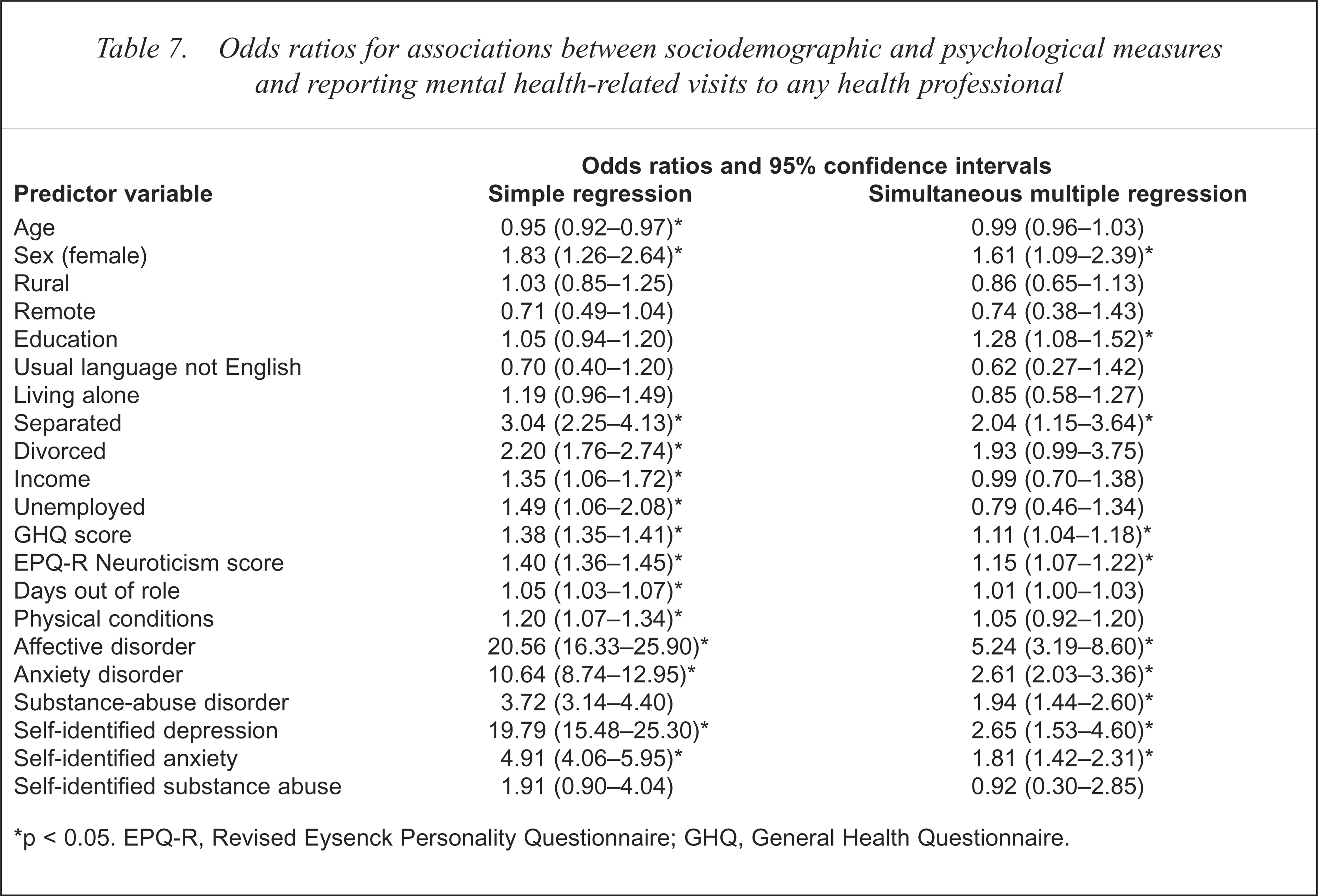
p < 0.05. EPQ-R, Revised Eysenck Personality Questionnaire; GHQ, General Health Questionnaire.
Significant associations resulting from simple logistic regressions between sociodemographic and psychological measures, and reporting mental-health related visits to each category of health practitioner
Associations common for all types of services
From the simple logistic regressions, it was found that nine predictor variables were positively associated with use of each of the five categories of mental health services: being separated, GHQ and EPQ-R Neuroticism scores, days out of role, having CIDI-diagnosed affective, anxiety or substance-abuse disorders and self-identifying as having depression or anxiety. A tenth variable, age group, was negatively associated with use of each category of service.
From the simultaneous multiple regressions, only two predictor variables, having CIDI-diagnosed depression or anxiety, were significantly associated with receiving each type of mental health service. In the remainder of this section, we report the significant associations found in these analyses that were not common to all categories of mental health services.
General practitioner services
With simple logistic regression, four more variables were found to be significantly associated with visiting a general practitioner for mental health reasons: being female, having English as usual language, being divorced or on government pension. When controlling for measures of mental disorder and psychological distress, two sociodemographic variables were significant predictors of mental health visits to general practitioners: being female and being separated. As well as CIDI-diagnosed affective and anxiety disorders (identified as common to all types of services), variables positively associated with reporting general practitioner visits were CIDI-diagnosed substance-abuse disorder, self-identified depression and anxiety and two psychological measures, the GHQ and EPQ-R Neuroticism scores.
Significant associations resulting from simultaneous multiple logistic regressions between sociodemographic and psychological measures, and reporting mental health-related visits to each category of health practitioner
Psychiatrist services
With simple logistic regression, five non-common results were found. Reporting mental health visits to a psychiatrist was positively associated with being divorced or on a government pension, number of physical conditions and having self-identified substance abuse. It was also negatively associated with being in a remote location. Using multiple logistic regression analysis, four non-common variables were positively associated with using these services: higher education, EPQ-R Neuroticism Score, and self-identified depression and anxiety, while two variables were negatively associated: living in a rural or remote location.
Psychologist services
Simple logistic regression indicated that three non-common variables were positively associated with using psychologist services: being female, having or undertaking higher education and living alone. Living in a remote area, however, was negatively associated with using these services. Using multiple logistic regression, two variables were positively associated with using these services: GHQ score and self-identifying as having CIDI-diagnosed substance-abuse disorder. Two sociodemographic variables were negatively associated with using such services: being older and living in a remote location.
Other health professionals' services
With simple logistic regression, five non-common variables were associated with use of any other health professional: being female, divorced, on a government pension, or unemployed and self-identifying as having substance abuse. With multiple logistic regression, nine further variables were significantly, positively associated with use of these services: being female, having or undertaking higher education, being separated or divorced, GHQ and EPQ-R Neuroticism scores, CIDI-diagnosed substance abuse disorder and self-identified depression and anxiety.
Any mental health services
Finally, using simple logistic regressions, five predictors not common to all types of services were positively associated with using any health professional for mental health reasons: being female, being divorced, on a government pension or unemployed and number of physical conditions. Using multiple logistic regression, eight further variables were associated with use of any mental health services: being female, having or undertaking higher education, being separated, GHQ and EPQ-R Neuroticism scores, self-identified depression or anxiety and CIDI-diagnosed substance abuse disorder.
Discussion
In these analyses, we set out to identify factors associated with Australians' use of formal health services for mental health reasons, first through simple logistic regression and then controlling at the same time for measures of psychological distress and mental disorders. Various conclusions can be drawn from these results.
Levels of utilisation of services by those with CIDI-diagnosed or self-identified affective or anxiety disorder are encouraging. As shown in Table 2, over 60% of those with CIDI-diagnosed affective disorder had obtained services from the formal mental health-care system in the past year. The corresponding figure for those with CIDI-diagnosed anxiety disorder was approximately 45%. These results would appear to rate well against similar measures reported from other countries [34,35].
While our results may be taken as an indication of the level of met need for mental health services, they are necessarily limited by our using categorical measures by which an individual either does or does not meet criteria for clinical diagnosis of mental disorder. Those with subclinical levels of depression, for example, may have functional impairment and could benefit from formal treatment [36]. Potential needs of this group are not considered when categorical measures of mental disorder are applied. Differences in severity of disorders are also not considered for those meeting diagnostic criteria for mental disorder. The additional predictive value of GHQ and EPQ-R Neuroticism scores after mental disorder has been taken into account confirms that the CIDI categorical measures of mental disorder do not indicate all mental health service needs. As noted earlier, a further limitation of our analysis is the potential overestimation of mental disorder that could result from using the CIDI-diagnostic instrument. We also appreciate that our findings on factors associated with using mental health services relate only to services provided for those with the common mental disorders. Use of mental health services by those with psychotic disorders was not assessed in this survey.
Need factors related to use of mental health services
Although simple logistic regression indicated that numerous sociodemographic variables were associated with use of mental health services, multiple logistic regression presented a quite different picture. Only two variables were significantly associated with utilisation of all five categories of mental health service: CIDI-diagnosed affective and anxiety disorders. The odds of those with CIDI-diagnosed affective disorder using any mental health service were over five times greater than those without that diagnosis. Similarly, controlling for sociodemographic and other health measures, those meeting criteria for CIDI-diagnosed anxiety disorder had over two and a half times the odds of consulting any health practitioner about mental health problems, compared with those not meeting these criteria. The conclusion that can be drawn from our analyses is that the main predictors of individuals' using mental health services are their having CIDI-diagnosed mental disorders or self-identifying as having mental health problems.
Predisposing and enabling factors
From the multiple regression analyses, three sociodemographic variables were found to be significantly, positively associated with making mental health visits to any health practitioner. These were being female, being separated and having a higher education. It should be noted, however, that none of these predictors was significantly associated with use of each category of mental health services.
The propensity of females to seek help has already been noted. Reasons put forward to explain this trend include females' increased likelihood of adopting the help-seeking role or of self-identifying as having a mental health problem [24,37]. Being female was associated with use of general practitioner services, the largest subgroup of mental health services. Females were significantly more likely than males to use services provided by ‘other health professionals’, but not services provided by psychiatrists and psychologists. Leaf and Bruce [38] similarly found women to be more likely to consult general practitioners, but not psychiatrists or psychologists, and noted that gender differences in utilisation were accounted for by differing attitudes towards such care, and not gender per se.
Being separated was significantly associated with use of any mental health service, as well as those provided by general practitioners and other health professionals, but not by psychologists or psychiatrists. This result is compatible with earlier findings that additional psychological distress, such as that which might result from relationship breakdown, is the factor that pushes individuals to seek this type of help [9,10]. It may also be that those dealing with this type of significant life event obtain sufficient counselling from general practitioners without needing specialist mental health care.
Finally, having or undertaking higher education has quite different effects across type of service provider. Those with higher education were not significantly more likely to use general practitioner services for mental health reasons, but were more likely to use psychiatrists, psychologists and other health professionals. Similar reports elsewhere have suggested that those with higher education define their health more broadly and have higher self-fulfilment needs [16,39], or view the use of such services more positively [40].
The previous paragraphs explored predictor variables significantly related to use of mental health services. It is also important to note the sociodemographic factors found to be not significantly associated with use of such services when multiple regression analysis was undertaken. Most Australians who obtain mental health services received them from general practitioners. Various sociodemographic variables that might have been expected to influence patterns of utilisation of general practitioner services, have not been found to do so when measures of mental disorder and psychological distress were taken into account. In our analysis, living in a rural or remote location, having or undertaking higher education, having a usual language other than English, being unemployed and being on government pension, allowance or benefit, were not significantly related to utilisation of general practitioner-provided mental health services. Similarly, living alone and number of physical conditions reported were not associated with level of use of this type of service. With respect to general practitioner-provided mental health services, it could thus be reasonably concluded that use of such services is not significantly affected by geographical location, education level and other broad measures of financial resources. Those in remote locations, however, do have lower levels of utilisation of specialist mental health services, while older Australians are less likely to use services provided by psychologists and other health professionals.
Conclusions
Overall, the major finding of this analysis is that the factors most strongly related to use of mental health services for the common mental disorders in Australia are having a CIDI-diagnosed affective, anxiety or substance abuse disorder and self-identifying as having mental health problems of depression and anxiety. This should be seen as a heartening result for those funding and providing Australia's mental health services given that these are the subsets of the community to whom such services are primarily targeted.