
Abstract
Objective:
To assess the beliefs of general practitioners (GPs), psychiatrists and clinical psychologists about the helpfulness of different interventions for mental disorders, and to examine change in beliefs over time.
Methods:
A questionnaire was mailed to 6848 GPs, psychiatrists and clinical psychologists registered with Medicare Australia. The questionnaire was based around one of six vignettes describing a person with a mental disorder: depression, depression with suicidal thoughts, early schizophrenia, chronic schizophrenia, social phobia and post-traumatic stress disorder. The depression and early schizophrenia vignettes were identical to those used in a similar survey of health professionals conducted in 1996. A range of interventions were rated for their likely helpfulness for each disorder, and consensus was defined as at least 66% of each profession rating an intervention as helpful.
Results:
Responses were received from 1536 health professionals. A broader array of interventions were endorsed for depression than in 1996, including GPs, psychiatrists, psychologists, becoming more physically active, reading about people with similar problems and how they have dealt with them, psychotherapy, and cognitive behaviour therapy. For the schizophrenia vignettes, GPs, psychiatrists and antipsychotics were thought to be helpful by a majority of professionals. A variety of professionals, psychological treatments and lifestyle activities were endorsed for the anxiety disorders. Differences between professions were noted in beliefs about the helpfulness of antidepressants and counsellors for anxiety disorders and depression, as well as cognitive behaviour therapy for schizophrenia.
Conclusion:
Consensus across professions was reached on the helpfulness of a variety of interventions for each mental disorder, although there were some notable differences in beliefs. The study gives an updated overview of treatment beliefs for mental disorders by Australian health professionals, which can be used as a benchmark with which to compare the beliefs of the Australian public.
Introduction
In 1996, Jorm and colleagues conducted surveys of Australian general practitioners (GPs), psychiatrists and clinical psychologists on their beliefs about interventions and outcomes for depression and schizophrenia (Jorm et al., 1997a). This survey complemented a matching nationally representative survey of the Australian public (Jorm et al., 1997b) and was carried out to evaluate whether the public held similar views to professionals about interventions for mental disorders. Although there were some significant differences between members of the public and professionals with regard to beliefs about which types of interventions are likely to be helpful (Jorm et al., 1997c), some differences between professions were also identified. Professionals tended to endorse treatments they specialised in, with psychiatrists less likely to believe that psychological and lifestyle interventions would be helpful, and clinical psychologists were more likely to believe in the helpfulness of cognitive behaviour therapy but less likely to believe in electroconvulsive therapy. There was also evidence that age was a factor associated with helpfulness beliefs, as younger professionals tended to endorse a broader range of interventions as helpful, rather than a narrow range specific to their profession.
Since the original survey of the Australian adult public in 1995, additional national mental health literacy surveys have been conducted with the public in 2003/2004 and 2011 to see whether there have been changes in recognition of mental disorders and beliefs about treatments (Reavley and Jorm, 2012). However, an updated survey of Australian health professionals had until recently not been carried out. In 2012, we conducted an updated survey of Australian health professionals so that areas in which public beliefs diverge from those of professionals can be identified and targeted. A new survey of professionals was necessary because professional beliefs may have changed since 1996 with the emergence of new evidence. In addition to the depression and schizophrenia vignettes used in the original 1996 survey, the 2012 survey included two anxiety disorder vignettes (social phobia and post-traumatic stress disorder), as well as a vignette describing depression with suicidal thoughts and one describing chronic, longstanding schizophrenia.
This paper reports the results from the survey of professionals and focuses on beliefs about the helpfulness of a wide range of interventions for mental disorders. The overall aim of the study was to evaluate whether GPs, psychiatrists and clinical psychologists have similar beliefs about the helpfulness of different interventions for mental disorders. We were interested in describing the views of professionals on the additional mental disorders not included in the previous survey. Furthermore, owing to developments in the evidence base and changes in the composition of each professional workforce over the intervening 16 years, we explored whether beliefs about interventions for depression and early schizophrenia had changed over time.
Methods
Sample
The questionnaire was mailed to 6848 health professionals registered with Medicare Australia in June 2012. The sample of professionals consisted of a random sample of 3000 GPs who had provided more than 50 services in the past year, a random sample of 1800 registered clinical psychologists, and all active psychiatrists (2048). We aimed for an achieved sample of 100 for each profession and each vignette, which would give 95% confidence intervals of around ± 9%. We conservatively assumed response rates of 20% for GPs and 33% for clinical psychologists and psychiatrists, based on response rates for the previous professional survey on youth mental health literacy (Jorm et al., 2008b). The study received ethical approval from the Human Research Ethics Committee at The University of Melbourne. It was also approved by the External Requests Evaluation Committee at the Department of Human Services (DHS), which conducted the mail-out on our behalf to comply with privacy legislation. Follow-up of non-responders was not permitted by the DHS.
Questionnaire
The questionnaire was based around a vignette of a person with a mental disorder: depression, depression with suicidal thoughts, early schizophrenia, chronic schizophrenia, social phobia, and post-traumatic stress disorder (PTSD). Participants were randomly sent one of the six vignettes, stratified by profession type. Vignettes were identical to those used in telephone surveys of the Australian public, except that all referred to a male ‘John’ in the vignettes (Reavley and Jorm, 2011). The depression vignette and the early schizophrenia vignette were identical to those used in the 1996 survey of health professionals. All vignettes were written to satisfy diagnostic criteria according to the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) and International Classification of Diseases (ICD)-10. Based on the written vignette, participants were asked what, if anything, is wrong with John, followed by a series of questions on the likely helpfulness of a range of interventions. These included different (1) people: a typical family GP or doctor; a typical chemist (pharmacist); a counsellor; a social worker; telephone counselling service, e.g. Lifeline; a psychiatrist; a psychologist; help from his close family; help from some close friends; a naturopath or a herbalist; the clergy, a minister or a priest; John tries to deal with his problems on his own; (2) medications: vitamins and minerals, tonics or herbal medicines; analgesics; antidepressants; antibiotics; sedatives / hypnotics; antipsychotics; tranquilisers such as valium; and (3) activities: becoming more physically active; reading about people with similar problems and how they have dealt with them; getting out and about more; courses on relaxation, stress management, meditation or yoga; cutting out alcohol altogether; psychotherapy; cognitive behaviour therapy (CBT); hypnosis; admission to a psychiatric ward of a hospital; electroconvulsive therapy (ECT); having an occasional alcoholic drink to relax; a special diet or avoiding certain foods; consulting a website that gives information about his problem; consulting an expert using email or the web about his problem; consulting a book that gives information about his health problem; receiving information about his problem from a health educator. The response scale was helpful, harmful, neither, depends, don’t know. This differs from the survey conducted in 1996, which only allowed responses of helpful, harmful or neither. The questionnaire also asked questions on beliefs about prognosis with and without treatment, beliefs about stigma and discrimination, and respondent characteristics (not reported here).
Statistical analysis
Chi-squared tests were used to evaluate whether there were differences between professions in ratings of helpfulness of interventions. Owing to the large number of statistical tests carried out, we used the more conservative p < 0.01 as the significance level. We also report Cramer’s V as a measure of the strength of the association. Cramer’s V varies from 0 to 1, with small, medium and large effect sizes represented by 0.1, 0.3 and 0.5, respectively. In the 1996 professional survey, consensus on intervention helpfulness was defined as occurring when at least 66% of each profession rated an intervention as helpful. We have followed the same convention in this paper to allow for comparison across time.
Results
We received 1536 returned surveys from 518 GPs, 506 psychiatrists and 498 clinical psychologists (14 respondents did not indicate a profession). Response rates were 17.3%, 24.7% and 27.7%, respectively. Responses for each of the six vignette types were: depression (280), depression with suicidal thoughts (261), early schizophrenia (237), chronic schizophrenia (259), social phobia (242) and PTSD (257).
The mental disorders described in the vignettes were correctly identified by the majority of professionals, supporting the validity of the vignettes. Depression was identified by 95% of professionals in both depression vignettes, and 12% also identified suicidal thoughts in the depression with suicidal thoughts vignette. Ninety-five percent of professionals identified psychosis, a psychotic disorder, or schizophrenia in the early and chronic schizophrenia vignettes, 90% of professionals identified post-traumatic stress disorder in the PTSD vignette, and 86% identified social phobia or social anxiety in the social phobia vignette.
Depression vignettes
Table 1 shows the percentage of health professionals who rated each intervention as helpful for John in the depression and depression with suicidal thoughts vignettes. Only interventions with a rating of at least 66% from one profession group are reported. Ratings across the two vignettes are broadly similar, but with some notable differences. Interventions endorsed by a majority of all three professions for both vignettes were: GPs, psychiatrists, psychologists, becoming more physically active, reading about people with similar problems and how they have dealt with them, psychotherapy, and CBT. Antidepressants were not endorsed for the depression vignette, as 34.9% of clinical psychologists said it depends. However, all three profession groups endorsed antidepressants for the depression with suicidal thoughts vignette. Likewise, cutting out alcohol was endorsed by all three groups in the depression with suicidal thoughts vignette, but not for the depression vignette. Counsellors were rated as helpful more frequently by GPs than by psychiatrists or clinical psychologists in both vignettes. Where there was a significant association between profession group and intervention rating, effect sizes were small to medium in size, with no large associations found. The biggest effect sizes were for ECT (Cramer’s V = 0.35 in the depression vignette, Cramer’s V = 0.30 in the depression with suicidal thoughts vignette; not shown in Table 1). Although ECT was not rated as helpful by a majority of any group, there were clear differences in ratings across groups. For example, it was rated as helpful for depression by 10% of GPs, 37% of psychiatrists and 1% of clinical psychologists; and harmful by 28% of GPs, 8% of psychiatrists and 45% of clinical psychologists.
Percentage of health professionals rating an intervention as helpful for depression or depression with suicidal thoughts.
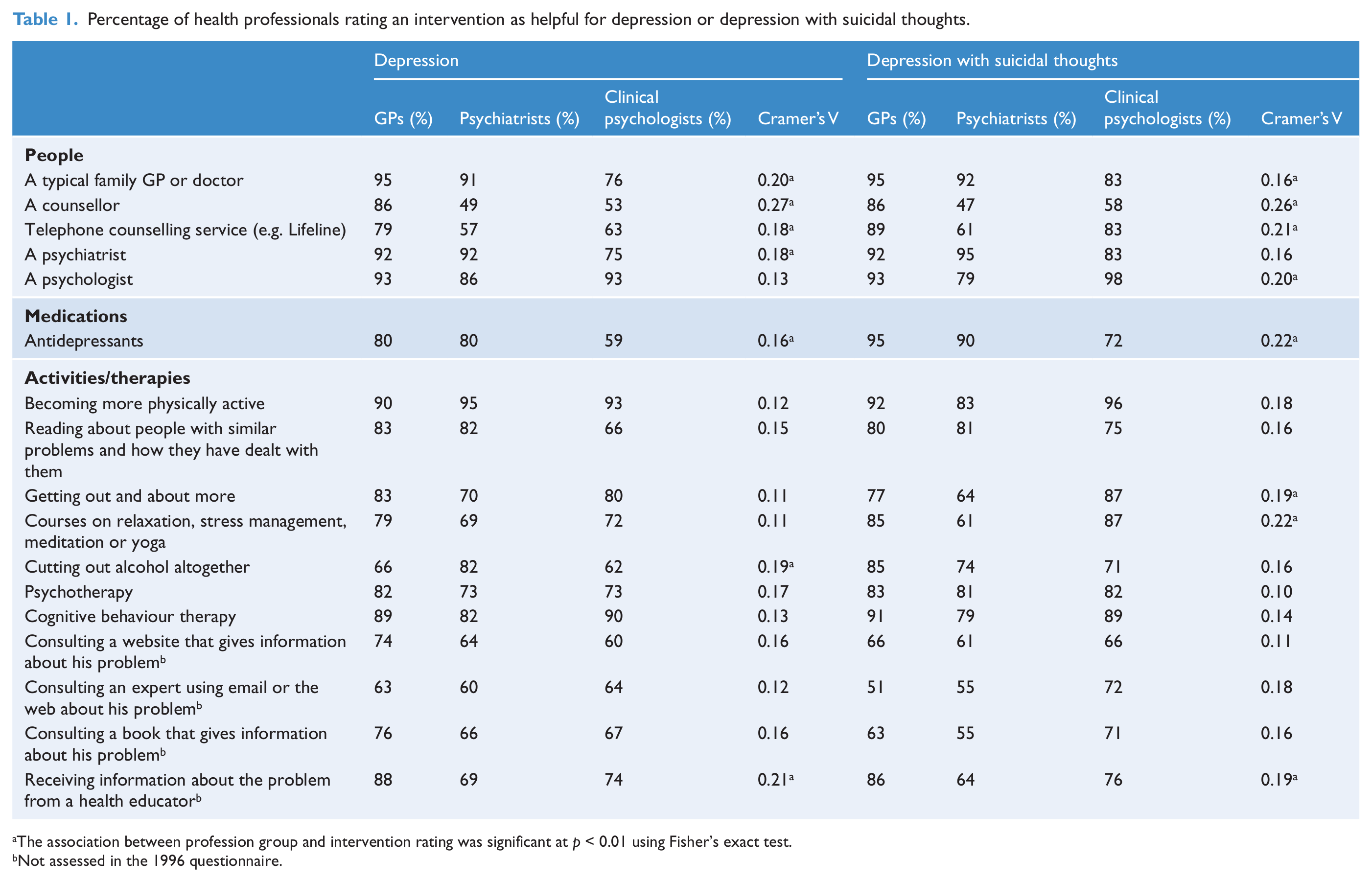
The association between profession group and intervention rating was significant at p < 0.01 using Fisher’s exact test.
Not assessed in the 1996 questionnaire.
Change over time
In 1996, interventions endorsed as helpful for John in the depression vignette were GPs, psychiatrists, clinical psychologists, antidepressants, counselling and CBT (Jorm et al., 1997a). Sixteen years later, a greater number of self-help activities were endorsed by all three professions, including becoming more physically active, reading about other people with similar problems and how they have dealt with them, getting out and about more and courses on relaxation, stress management, meditation or yoga. These changes were largely a function of psychiatrists increasing their helpfulness ratings to be more in line with those of GPs and clinical psychologists.
Harmfulness
Only one intervention was rated as harmful by a majority of all three professional groups. ‘John tries to deal with his problems on his own’ was rated as harmful by over 50% of all three professions for the depression with suicidal thoughts vignette (GPs 72%, psychiatrists 66%, clinical psychologists 50%), but not for the depression vignette (GPs 54%, psychiatrists 62%, clinical psychologists 41%).
Schizophrenia vignettes
Table 2 shows the percentage of helpfulness ratings for interventions that were endorsed by at least 66% of any professional group for the early and chronic schizophrenia vignettes. A majority of health professionals endorsed consulting with GPs and psychiatrists and using antipsychotics as helpful for early schizophrenia and chronic schizophrenia. Cutting out alcohol altogether was also endorsed for early schizophrenia but not for chronic schizophrenia. Significant associations between profession and intervention rating were small to medium in size. Particularly noteworthy was the association between CBT ratings and profession group. In both vignettes, a substantial majority of clinical psychologists rated it as helpful, compared with less than half of the GPs or psychiatrists.
Percentage of health professionals rating an intervention as helpful for early schizophrenia or chronic schizophrenia.
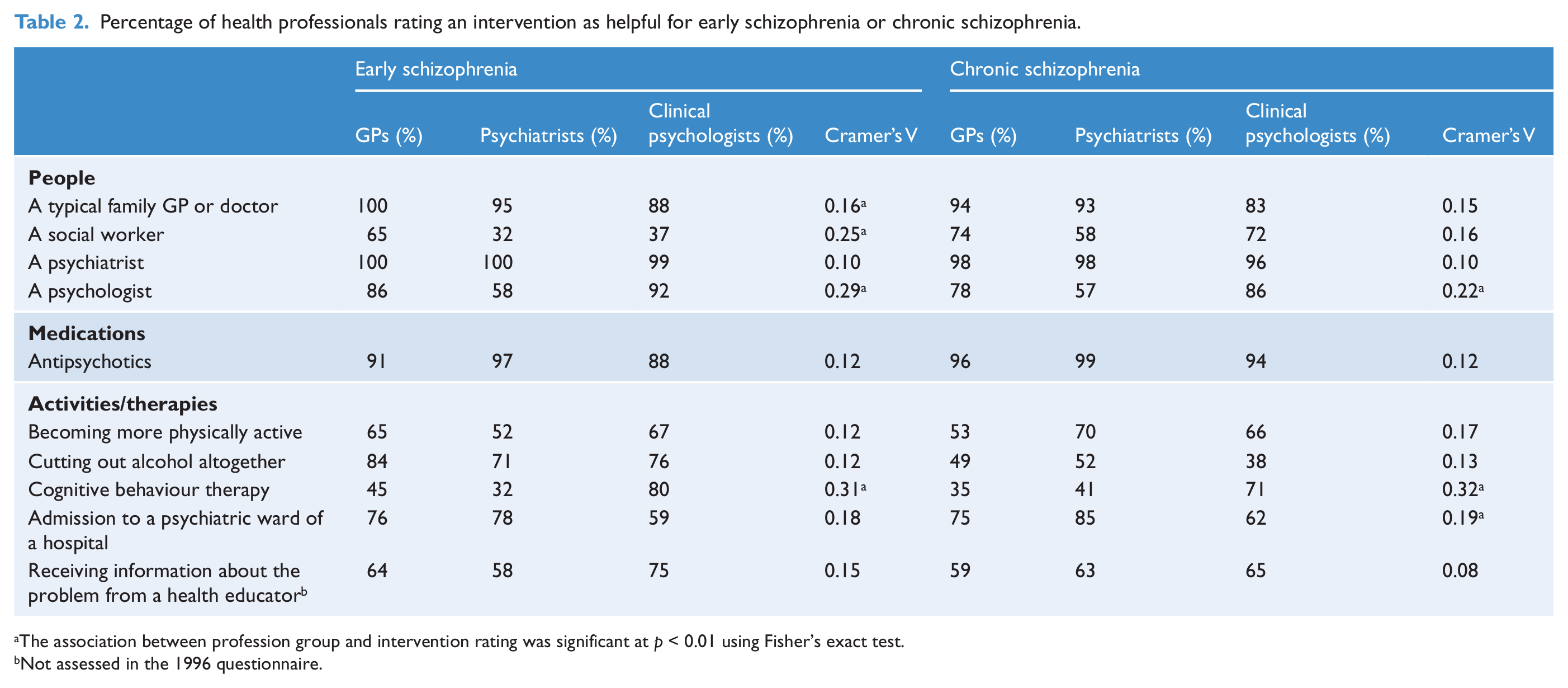
The association between profession group and intervention rating was significant at p < 0.01 using Fisher’s exact test.
Not assessed in the 1996 questionnaire.
Change over time
Interventions endorsed as helpful for early schizophrenia in 1996 were GPs, psychiatrists, clinical psychologists, antipsychotics and admission to a psychiatric ward (Jorm et al., 1997a). In 2012, admission to a psychiatric ward was not endorsed because 35.2% of clinical psychologists said it depends. In addition, psychologists were not endorsed because 35.5% of psychiatrists said it depends.
Harmfulness
‘John tries to deal with his problems on his own’ was the only intervention rated as harmful by at least 50% of each profession for both schizophrenia vignettes (early schizophrenia: GPs 89%, psychiatrists 88%, clinical psychologists 81%; chronic schizophrenia: GPs 76%, psychiatrists 74%, clinical psychologists 61%).
Anxiety disorder vignettes
Table 3 shows the percentage of health professionals who rated each intervention as helpful for social phobia and PTSD. Only interventions with a rating of at least 66% from one profession group are reported. For the social phobia vignette, all three groups endorsed psychiatrists, psychologists, becoming more physically active, reading about people with similar problems and how they have dealt with them, courses on relaxation, psychotherapy, CBT, consulting a book that gives information, and receiving information from a health educator. GPs were not endorsed because 29.6% of clinical psychologists said it depends. The largest associations between profession and intervention rating were for a counsellor and telephone counselling, which were rated as helpful by more GPs than psychiatrists or clinical psychologists.
Percentage of health professionals rating an intervention as helpful for social phobia or post-traumatic stress disorder.
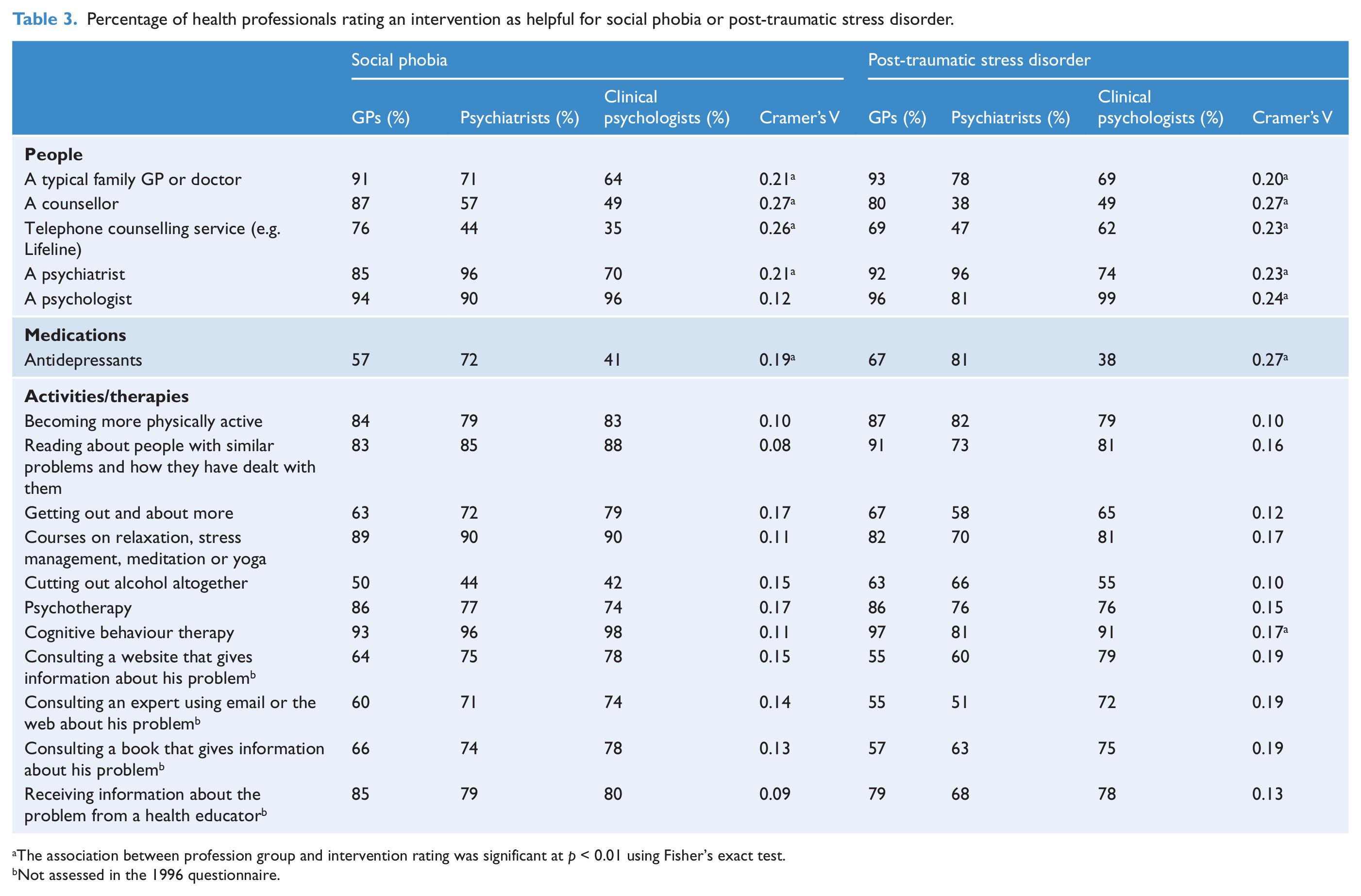
The association between profession group and intervention rating was significant at p < 0.01 using Fisher’s exact test.
Not assessed in the 1996 questionnaire.
Results were similar for the PTSD vignette. Interventions endorsed by all three groups were GPs, psychiatrists, psychologists, becoming more physically active, reading about people with similar problems and how they have dealt with them, courses on relaxation, psychotherapy, CBT, and receiving information from a health educator. Again, a counsellor was rated as helpful by more GPs than psychiatrists and clinical psychologists. Antidepressant ratings also significantly varied by profession group for both vignettes. Most psychiatrists endorsed their helpfulness, followed by fewer GPs, and then by only a minority of clinical psychologists.
Harmfulness
A few interventions were rated as harmful for social phobia by more than 50% of each group: analgesics (GPs 53%, psychiatrists 65%, clinical psychologists 60%); sedatives/hypnotics (GPs 72%, psychiatrists 58%, clinical psychologists 63%); and ECT (GPs 71%, psychiatrists 74%, clinical psychologists 86%). No interventions were rated as harmful by 50% or more of each profession for PTSD.
Discussion
This study reported on the beliefs of Australian GPs, psychiatrists and clinical psychologists about the helpfulness of treatments for mental disorders. Consensus was reached on the helpfulness of a variety of mental health professionals, therapies and activities for each mental disorder. Fewer interventions were thought to be helpful for the schizophrenia vignettes than the other vignettes. Some differences between professions were observed for particular interventions, but these were small to moderate in size. There was a tendency for each profession to rate its own professionals and treatments higher than those of others, as was evident in the 1996 survey and also in a recent survey of pharmacists’ mental health literacy (O’Reilly et al., 2010). A particularly striking example of this was in ratings of CBT for schizophrenia, which was heartily endorsed by clinical psychologists, but much less so by GPs and psychiatrists. Although medication is the core treatment for schizophrenia, Australian clinical practice guidelines also recommend psychosocial interventions, including CBT, to improve psychopathology and functioning (Royal Australian and New Zealand College of Psychiatrists Clinical Practice Guidelines Team for the Treatment of Schizophrenia and Related Disorders, 2005). Delivered in addition to usual care, CBT has evidence supporting its modest effect on positive symptoms, negative symptoms and functioning (Wykes et al., 2008), though a recent review suggests it may not be any more effective than nonspecific supportive therapy (Newton-Howes and Wood, 2011). The more tempered acceptance of CBT by GPs and psychiatrists mirrors clinical psychologists’ weak support for medical treatments (i.e. antidepressants) for treating anxiety disorders. The results from this study are similar to those reported from other countries that show beliefs about treatments vary somewhat across professional groups, particularly beliefs about antidepressants, psychotherapy and ECT (Lauber et al., 2005).
Some changes over time were evident regarding beliefs about treatments for depression and early schizophrenia. A greater number of self-help and lifestyle activities were endorsed for depression in comparison with the 1996 survey, in line with research suggesting the value of physical activity (Mead et al., 2009), bibliotherapy (Gregory et al., 2004), yoga (Uebelacker et al., 2010) and relaxation techniques for depression (Jorm et al., 2008a). This is consistent with the prediction by Jorm et al. (1997a) that there would be a broadening of professional beliefs in the future. In the original survey there seemed to be a cohort effect related to training or attitudes, with younger medical professionals more accepting of psychosocial interventions than their older peers. In contrast to the depression results, the range of endorsed treatments narrowed for early schizophrenia. However, this may be due to the different response scale used in the current study, which permitted more nuanced responses including ‘depends’ and ‘don’t know’. This meant that some treatments were not endorsed by a majority of professionals, usually because helpfulness was judged to depend (on some unknown factor).
Ratings of antidepressant helpfulness varied across vignettes and professions. In the 1996 survey, antidepressants were rated as helpful for depression by 98% of GPs and psychiatrists and 89% of clinical psychologists, but in the current study helpfulness ratings were lower and antidepressants were thought to be helpful by all three professions only for the depression with suicidal thoughts vignette. This change over time may be partly attributed to the different response scale, allowing some respondents to say it depends. Given that more respondents thought antidepressants would be helpful for the depression with suicidal thoughts vignette, the depression vignette may have been interpreted as not severe enough to justify treatment with antidepressants. Meta-analyses have indicated that antidepressants are effective for very severe depression, but show minimal benefit over placebo in mild to moderate depression (Fournier et al., 2010). For the anxiety disorders, the three professions did not reach consensus on the helpfulness of antidepressants, with clinical psychologists in particular less likely to rate them as helpful. The lack of consensus for PTSD may reflect the inconsistency in conclusions from a variety of consensus guidelines on the treatment of PTSD, with some endorsing antidepressants as a first-line treatment, but others only as a second-line treatment (Stein et al., 2009). However, for social phobia, antidepressants have demonstrated efficacy in the short-term (Ipser et al., 2008) and both pharmacotherapy and CBT are recommended first-line options in clinical practice guidelines (Canadian Psychiatric Association, 2006).
Disorder severity may have been a consideration in responses, with higher ratings for the helpfulness of antidepressants and cutting out alcohol for depression in the presence of suicidal thoughts, as well as more respondents rating it harmful to deal with the problem alone. When asked to rate whether it would be helpful for John to deal with social phobia or PTSD on his own, very few thought this would be helpful, but most did not think it would be harmful either. These ratings suggest that many respondents did not see a clear need for professional help for these disorders. This is curious, particularly as more members of the public rated dealing with the problem alone as harmful than professionals (Reavley and Jorm, 2011) and without being treated these disorders are likely to cause longstanding problems.
This study has several limitations which suggest caution in interpretation of results. The response rate was quite low, particularly for GPs, which may reduce the generalisability of these results. The smaller sample size and greater number of vignettes meant that it was not feasible to examine whether age and gender were associated with helpfulness ratings. As in previous surveys, these results are based on a constrained vignette designed for use with the public, and responses could not convey strength of helpfulness of interventions. Further, using a vignette design to elicit treatment beliefs may not correspond with professional behaviour during clinical practice, where selection of treatment is likely to be dynamic and negotiated with the consumer. Finally, the response scale was not identical to that used in the original 1996 survey, as it allowed for responses of don’t know and depends.
Despite these limitations, the study gives an updated overview of treatment beliefs for mental disorders by Australian health professionals, which can be used as a benchmark with which to compare the beliefs of the Australian public.
Footnotes
Acknowledgements
We thank the Commonwealth Department of Human Services for conducting the mail-out to the health professionals.
Funding
This research was funded through an NHMRC Australia Fellowship and NHMRC Program Grant 566529.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.