
Abstract
We have developed and tested an Italian version of the Migraine Disability Assessment (MIDAS) questionnaire, an established instrument for assessing headache-related disability. A multistep process was used to translate and adapt the questionnaire into Italian, which was then tested on 109 Italian migraine without aura patients, 86 (78.9%) of whom completed the form a second time 21 days later. Overall MIDAS score had good test–retest reliability (Spearman's correlation 0.77), closely similar to that found in English-speaking migraineurs, and individual responses were also satisfactorily reliable. Internal consistency was good (Cronbach's alpha 0.7). These findings support the use of the MIDAS questionnaire as a clinical and research tool with Italian patients.
Keywords
Introduction
Migraine is a primary headache form characterized by recurrent pain attacks of moderate to severe intensity, associated with autonomic symptoms (1). It is a widespread disorder, affecting about 10–15% of the general population (2–4), that often limits everyday activities. Work and school performance are impaired (5–7) but participation in family, recreational and social activities may also be reduced (8, 9). Migraine headache may vary in frequency, duration, pain intensity, and number and severity of associated symptoms, both from patient to patient, and with time in a given patient. The condition has a wide range of impacts, from little or none to recurrent or prolonged difficulties in daily activities (6, 10, 11).
Disability refers to the impact of illness on ability to work and function in various settings and roles (12). Information on disability in migraine complements the diagnosis by helping the physician to assess the need for treatment (11). Furthermore, reduction in headache-related disability is one of the main treatment goals in the most recent guidelines for the management of headaches, published by the United States (US) Headache Consortium (13). Despite this, and although specific questionnaires to assess headache-related disability have been developed (14–17), assessment methods are not yet standardized.
The Migraine Disability Assessment (MIDAS) questionnaire was designed and tested by Stewart and Lipton to capture headache-related disability in all life domains over a clinically relevant time period. The questionnaire, which has been extensively studied and validated (16, 18–20), contains just seven questions and has simple and intuitive scoring rules. These features suggest the instrument as an optimal tool for screening purposes and for informing treatment decisions on individual patients. It would therefore be useful to have versions of MIDAS in languages other than English for use with non-English speaking patients.
The aim of the present study was to produce a definitive Italian version of the MIDAS questionnaire using formal translation procedures and subsequently to assess internal consistency and the test–retest reliability of scores from one administration to another, in a clinical series of Italian migraine patients.
Methods
The MIDAS Questionnaire
The English version of the MIDAS self-administered questionnaire adapted in this study was that published in 1999 (16). The first five questions investigate the influence of headache on three domains of activity over the preceding three months: paid work or school work, household work, and family social and leisure activities. Questions 1 and 2 investigate paid work, enquiring as to the number of days off work due to headache and the number of days where productivity was reduced by half or more. Questions 3 and 4 ask the same questions about household work. Question 5 enquires about missed days of recreational, social and family activities. The last two questions (A and B) concern headache frequency (number of days with headache in the previous 3 months) and headache intensity (average pain intensity of headache attacks); they are not used to calculate disability.
The total score is obtained summing the individual scores (number of days affected) of the first five questions. Four disability grades are obtained expressing increasing impairment of activities: grade I, minimal or infrequent disability, when total score is 0–5; grade II, mild or infrequent disability, when total score is 6–10; grade III, moderate disability, when scores range from 11 to 20; and finally grade IV, severe disability, for patients with total scores of 21 or more.
Translation
The translation was a multistep process employing a standardized methodology (21, 22). Briefly, two translators produced two independent Italian translations and met to develop a single agreed version. This forward translation was evaluated by a panel of experts in terms of use of simple, correct language and equivalence to the English version. The panel consisted of the principal study investigators (neurologists with experience in clinical migraine and research on migraine, and experts on health outcome research), one of the translators, and a member of the Italian Association of Headache Patients (AIC). The forward translation was modified by the panel and then back-translated into English by two different expert translators. The two backward translations were submitted to one of the developers of the original MIDAS (RB Lipton) to assess conceptual and semantic equivalence to the English questionnaire. A final meeting of the panel produced the definitive Italian translation, taking note of the comments of RBL.
Test–retest reliability
The inclusion criterion for the study were diagnosis of migraine without aura according to International Headache Society criteria (1) and presentation at the Regional Headache Center, C. Besta Neurological Institute, Milan, or the Headache Center of the University of Bari. Between May and November 1999 one hundred and nine consecutive eligible patients of both sexes were enrolled from among outpatients presenting at these centres. They were asked to complete the Italian MIDAS twice: the first time at the centre after routine neurological examination in the presence of the neurologist and the second at home 3 weeks later. This 21-day interval was the same as that used in the original MIDAS validation studies (16, 18). During the first compilation patients were urged to report on anything that was unclear or gave rise to any problem. No change in ongoing therapy (symptomatic or prophylactic) was prescribed to the patients during the course of the test–retest study.
Test–retest reliability between the first and second compilations was evaluated by the Spearman and Pearson correlation tests on total score and individual question scores (including the last two unscored questions). The Spearman correlation tends to be conservative because it is not usually influenced by outliers, whereas the Pearson correlation coefficient is influenced by outliers. The Student t
The stability of MIDAS grades between first and second compilations was evaluated as percentage concordance of the second compilation relative to the first. The internal consistency of MIDAS scoring was assessed using Cronbach's alpha.
Results
All patients completed the form relatively quickly and none asked any questions which indicated they had difficulties understanding any part of the questionnaire. Cronbach's alpha was 0.74 at the first compilation and 0.75 at the second, and hence exceeded the 0.70 level considered to indicate good internal consistency. We therefore conclude that the form was easily understood and well accepted by the patients. The impression of all the physicians involved in the study was that the Italian version retained the easy-to-understand format of the original MIDAS, and furthermore that the scoring was simple to calculate.
Of the 109 patients enrolled, 86 (78.9%) completed the MIDAS form twice, while 23 (21.1%) did not return the second form and were considered dropouts. The main characteristics of the patients are shown in Table 1. As expected, the sample consisted of more than twice as many women as men. The mean age and the proportion of women were similar to those reported for migraine patients within the general population (2–4). Mean illness duration was 17.2 years; mean education was 12.9 years.
Main characteristics of the headache without aura patients

As Table 1 shows, there were no significant differences between the dropouts and those who completed the study, although those who completed tended be women, older, with more education and longer illness duration; furthermore the percentage of patients with grades III and IV (moderately and severely disabled) was higher in participants than dropouts.
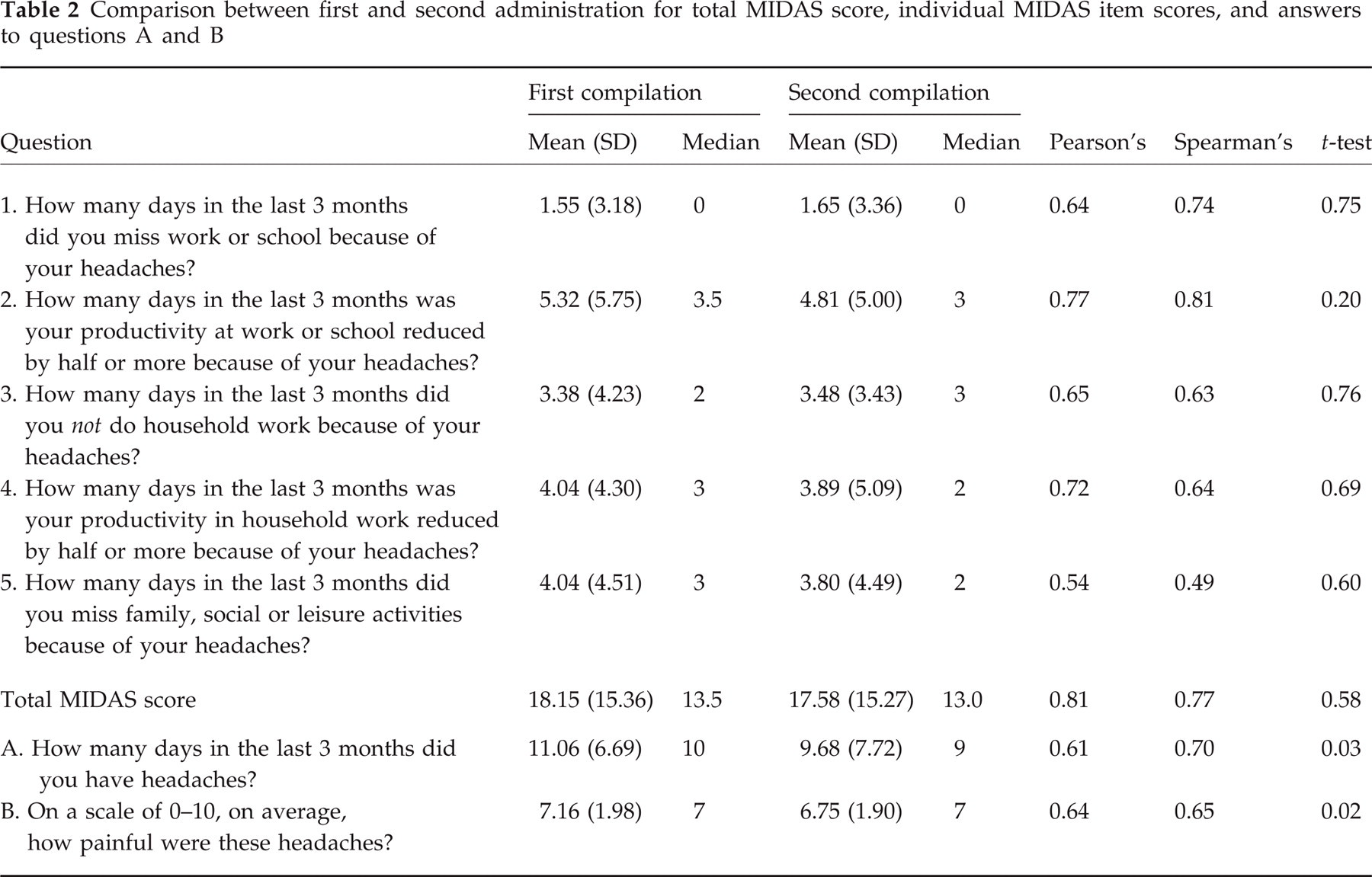
The results of the first and second compilations, in the 86 patients who completed the form twice, are compared in Table 2. For each question, mean score was lower at the second compilation; however, the differences were never significant by the t-test. Spearman's correlation coefficient ranged from 0.49 for question 5 to 0.81 for question 2. As expected, Pearson's coefficient values were similar to those of Spearman (Table 2). Total MIDAS scores also correlated highly from one compilation to the next (Pearson's 0.81 and Spearman's 0.77). For questions A and B Pearson's correlation coefficients were 0.61 and 0.64 and Spearman's correlations were 0.70 and 0.65, respectively.
Comparison between first and second administration for total MIDAS score, individual MIDAS item scores, and answers to questions A and B
The numbers of patients who changed MIDAS disability grade from the first to the second compilation are shown in Table 3. The overall concordance was 64%, i.e. 55 of the 86 patients had the same MIDAS disability at both compilations. In 27/31 (87%) the difference was one grade, and in four (13%) the difference was >1 grade. In none of the 27 cases was the change in disability grade due to a one-point change in score; in two cases it was due to a two-point change and in another two to a three-point change. The percentage concordance was high in patients with minimal and with severe disability (77% for grade I; 80% for grade IV), but was much lower in patients with mild to moderate disability (27% for grade II; 54% for grade III).
Numbers of patients who changed MIDAS disability grade from first to second compilation

Table 4 shows test–retest correlation coefficients for Italian patients in comparison with those obtained in American and English patients (16, 18). Total MIDAS scores were similar in all groups even though the selection methods differed (migraineurs sampled from the general population in the United States of America and United Kingdom, clinical series for Italy).
Pearson's and Spearman's correlation coefficients in Italian, American and English migraine populations

Eighty-six migraine without aura patients from clinical series.
Ninety-seven migraine patients from general population, Stewart et al. (18).
One hundred migraine patients from general population, Stewart et al. (18).
Discussion
This is the first study to assess the MIDAS questionnaire in a language other than English after translation and adaptation. We previously conducted a pilot study to assess an Italian translation of the older six-item MIDAS questionnaire. This showed that the instrument was reliable and potentially useful for quantifying disability in Italian migraine patients (23). The present study has shown that the final Italian version of MIDAS is well-accepted by patients. The care taken with the translation and cultural adaptation has produced a questionnaire that retains the clear and simple language of the original.
Statistical analysis showed that the Italian MIDAS had satisfactory test–retest reliability. The total score and individual question scores were satisfactorily reproducible from one test to the next, with correlation coefficients similar to those reported when the original version of the questionnaire was tested on US and British migraine patients. The internal consistency of the Italian MIDAS was also good, with values of Cronbach's alpha of 0.74 and 0.75, closely similar to the values reported for US and British patients (16, 18). The test–retest reliability of the two unscored questions on frequency and intensity of headache was also satisfactory.
Question 5 had the lowest correlation coefficient in both our patients and the British patients (18). This may be because the activities probed by this question (social, family and leisure) vary more with time than the relatively constant activities of paid work and housework (probed by questions 1–4). The composite nature of question 5 may also have contributed to the variability, in that the weight given to the different activities may change with time. The clinical impression is that migraine patients are more likely to renounce leisure activity rather than family activity, even if severely affected by a headache.
In about a third of our patients, disability grade differed between the first and second compilations. In addition to random variation, changes in the severity and frequency of headaches over the relatively long 21-day period are possible, resulting in changes in MIDAS grade from one test to the next. In the recently proposed stratified care approach to migraine (24) patients with different MIDAS disability grades receive different symptomatic drugs as first-line treatment. Patients with lower grades may receive non-specific drugs (NSAIDS or analgesics), while patients with grades III and IV may have significantly better outcomes if given triptans from the outset (25, 26).
Considering our results in relation to the stratified care approach, we note that in patients with intermediate disability, MIDAS grades were not stable. However, only in a minority of cases (14 subjects, 16% of the patients who completed the study) would the change (i.e. from grades I–II to grades III–IV or vice versa) imply a different treatment plan.
It is worth noting that the majority of our patients (65.1% of the 108 enrolled, and 61.5% of those who completed the form a second time) had moderate or severe disability (grade III or IV, respectively). These percentages are higher than those reported by the Stewart et al. study on a sample of migraineurs from the general population in USA (18). This may be because migraineurs attending headache centres have more severe headaches than the entire migraine population. Another contributor to this difference could have been the fact that Stewart et al.'s study included migraine with aura patients (who usually have a much lower headache frequency than migraine without aura patients), while our study enrolled only migraine without aura patients.
In conclusion, the Italian MIDAS form maintains the brevity and simplicity of the English version, and is characterized by test–retest reliability parameters closely similar to those of the original. It is therefore suitable as a clinical and research tool with Italian patients
Footnotes
Acknowledgements
Particular thanks are due to Professor RB Lipton, not only for checking and commenting on the backward translations, but also for his for active encouragement throughout the study. Dr Giovanni Apolone provided valuable suggestions on study methodology. We also thank Mario Ajello, President of the Italian Association of Headache Patients. Don Ward checked the English. The study was supported by the Italian Ministry of Health.