
Abstract
FK506 is a candidate drug for acute stroke. For such drugs, any decision to proceed to clinical trial should be based on a full and unbiased assessment of the animal data, and consideration should be given to the limitations of those data. Such an assessment should include not only the efficacy of a drug but also the in vivo characteristics and limits to that efficacy. Here we use systematic review and meta-analysis to assess the evidence for a protective effect of FK506 in animal models of stroke. In all, 29 studies were identified describing procedures involving 1759 animals. The point estimate for the effect of FK506 was a 31.3% (95% confidence interval 27.2% to 35.4%) improvement in outcome. Efficacy was higher with ketamine anaesthesia and temporary ischaemia and was lower in rats, in animals with comorbidities, and where outcome was measured as infarct size alone. Reported study quality was modest by clinical trial standards, and efficacy was lower in high-quality studies. These findings show a substantial efficacy for FK506 in experimental stroke, but raise concerns that our estimate of effect size might be too high because of factors such as study quality and possible publication bias.
Introduction
Only tissue plasminogen activator has proven efficacy in human studies (The National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group, 1995) despite an experimental literature describing the efficacy of more than 700 drugs in experimental stroke. While this might be due, at least in part, to factors such as the inappropriately long time windows used in most stroke trials, there remain concerns with the interpretation of the available animal evidence supporting efficacy, and Pound et al (2004) have argued for a more systematic evaluation of animal data before proceeding to clinical trials. Important information to be gained from such an approach may include not only the demonstration that a drug can have neuroprotective activity under ideal conditions, but also some idea of any limits to that efficacy, which may impact on clinical usefulness.
The ideal candidate neuroprotective drug is both effective and is sufficiently safe to allow it to be administered in a prehospital setting without extensive patient workup. We have been developing a clinical trial protocol for the prehospital administration of combination neuroprotectants in patients with suspected stroke (the Time Window in Neuroprotection (TWiN) study). To identify candidate drugs, we performed a brief semisystematic literature review, and then scored drugs according to criteria including the evidence for their efficacy, their safety profile and their potential ease of use (our unpublished observations). We are now exploring in more detail the limits to and determinants of efficacy for drugs thus identified, including FK506.
Systematic review and meta-analysis have contributed greatly to the interpretation and aggregation of data in clinical sciences. Systematic review uses a methodical approach to minimise the risk of bias in the selection of studies for inclusion, whereas metaanalysis combines results from individual studies to produce a better estimate of treatment effect (Egger et al, 2001). Stratified metaanalysis can then be used to explore the impact of particular study characteristics (Macleod et al, 2004, in press).
FK506 was identified in our semisystematic review as a candidate neuroprotective drug for the TWiN study; it has been used in transplant medicine for many years (Murphy et al, 2003), and clinical trials in stroke are planned (Labiche and Grotta, 2004). Biological activities of FK506 include inhibition of calcineurin activity (Liu et al, 1991) and of neuronal apoptosis (Macleod et al, 2001), and efficacy in animal models of renal (Nalesnik et al, 1990), hepatic (Suzuki et al, 1993) and myocardial (Weinbrenner et al, 1998) ischaemia. Here we have investigated the neuroprotective properties of FK506 in experimental stroke using systematic review, metaanalysis and stratified metaanalysis. Specifically, we have calculated a global estimate of the efficacy of FK506, and examined the impact of reported study quality and various study characteristics on the estimate of effect size.
Materials and methods
Studies of FK506 in animal models of stroke were identified from Pubmed (1974 to January 2004), Embase (1980 to January 2004) and BIOSIS (1969 to January 2004): search strategy [〈FK506〉] AND [〈stroke〉 OR 〈ischaemia〉]; hand-searching abstracts of scientific meetings including the Society for Neuroscience and the International Society for Cerebral Blood Flow and Metabolism; reference lists of identified publications; requests to senior authors of identified publications for references to other studies. We included all controlled studies of the effect of FK506 in animal models of focal cerebral ischaemia, where the outcome was measured as infarct size or a neurologic score.
We defined a ‘comparison’ as the assessment of outcome in treatment and control groups after treatment with an administered dose of drug or with vehicle, with treatment starting a given time before or after the induction of cerebral ischaemia. For each comparison, we extracted data for mean outcome, standard deviation (s.d.) and number of animals per group. Values for data expressed graphically were requested from authors. Where FK506 was administered in multiple doses, the comparison was grouped according to the first dose at the first time it was administered and the dose administered was recorded as the total dose in the first 24 h after ischaemia.
Where neurological tests were performed at different times, only the final test was included. Where one group of animals was scored in more than one neurological domain (for instance, motor and sensory scores), or where both neurological score and infarct size were measured, data were combined using metaanalysis (see below) to give an overall estimate of effect size and its standard error. We defined effect size as the proportional improvement in outcome (infarct size, neurologic score or combined score) in treated animals relative to untreated ischaemic controls.
The reported methodological quality of individual studies was scored against the following criteria: publication after peer review; statement of control of temperature; random allocation to treatment or control; masked induction of ischaemia; masked assessment of outcome; use of anaesthetic without significant intrinsic neuroprotective activity; appropriate animal model (aged, diabetic or hypertensive); sample size calculation; compliance with animal welfare regulations; statement of potential conflict of interests (Horn et al, 2001; Macleod et al, 2004). Each study was given a quality score out of a possible total of 10 points, and the group median was calculated.
Data were processed as described previously (Macleod et al, 2004). Briefly, for each comparison, the mean outcome for the treatment group and the s.d.'s in treatment and control groups were expressed as a proportion of the outcome in the control group, and the effect size (the difference between the treatment and control groups) and its standard error were calculated. Data were aggregated using a weighted mean difference method with the random effects model of DerSimonian and Laird (1986), a more conservative technique than fixed-effects metaanalysis.
To explore the impact of study characteristics on estimates of effect size, we then performed a stratified metaanalysis with experiments grouped according to reported quality score; use of aged, diabetic or hypertensive experimental animals; anaesthetic used; whether the data had been published in full or in abstract; permanent or temporary ischaemia; method of occlusion; outcome measure; time to outcome measurement; route of drug delivery; single or multiple dosing regime; and species and gender of animal used. The significance of differences between groups was assessed by partitioning heterogeneity and using the χ2 distribution with n−1 degrees of freedom, where n equals the number of groups. To allow for multiple comparisons, we set our significance level at P<0.001.
Results
Electronic searching identified 581 publications meeting the search criteria, of which 39 (23 papers, 15 abstracts) described the effect of FK506 in focal cerebral ischaemia, where the outcome was expressed as a volume of infarction or a neurological score. Hand searching identified a further 10 abstracts. In all, 20 abstracts described work also described in full papers, and since the search was performed one further abstract has been published in full. In response to our request for further relevant information one author provided unpublished data. This meta-analysis is therefore based on data from 24 full papers published between 1994 and 2004 (Sharkey and Butcher, 1994; Sharkey et al, 1996; Kuroda and Siesjo, 1996; Butcher et al, 1997; Aoyama et al, 1997; Takamatsu et al, 1998, 2001; Yoshimoto and Siesjo, 1999; Kuroda et al, 1999; Toung et al, 1999; Bochelen et al, 1999; Miyazawa et al, 2000; Aronowski et al, 2000; Arii et al, 2001; McCarter et al, 2001; Ebisu et al, 2001; Fredduzzi et al, 2001; Maeda et al, 2002; Brecht et al, 2003; Furuichi et al, 2003a, 2003b; Nito et al, 2004; Chung et al, 2004; Shichinohe et al, 2004), four abstracts (Sharkey et al, 1997; Toung et al, 1997; Janelidze et al, 1999; McGregor et al, 2001) and one personal communication (J Aronowski); it represents the work of 14 independent groups, and nine of 29 publications came from groups funded directly by the Fujisawa Chemical Company, the manufacturers of FK506. Within the 29 studies, 109 comparisons (see Materials and methods for definition) were identified.
The global estimate of the effect of FK506 was 0.313 (95% confidence interval (CI) 0.272–0.354, P<10−50), an improvement in outcome of around 30% (Figure 1). There was significant statistical heterogeneity (χ2=361, df=108, P<10−28) between comparisons. Study characteristics are shown in Table 1. No study described a sample size calculation or contained a statement of potential conflict of interest. Random allocation to treatment group was described in only six studies; induction of ischaemia by an investigator masked to treatment allocation in one study and masked assessment of outcome in two studies. The median reported quality score (see Materials and methods) was 4 (range 0 to 7), and classifying studies by quality score accounted for a significant part of the between-group heterogeneity (χ2=113.3, df=7, P<10−20), with studies of higher quality giving a lower estimate of effect size (Figure 2).
Quality characteristics of included studies
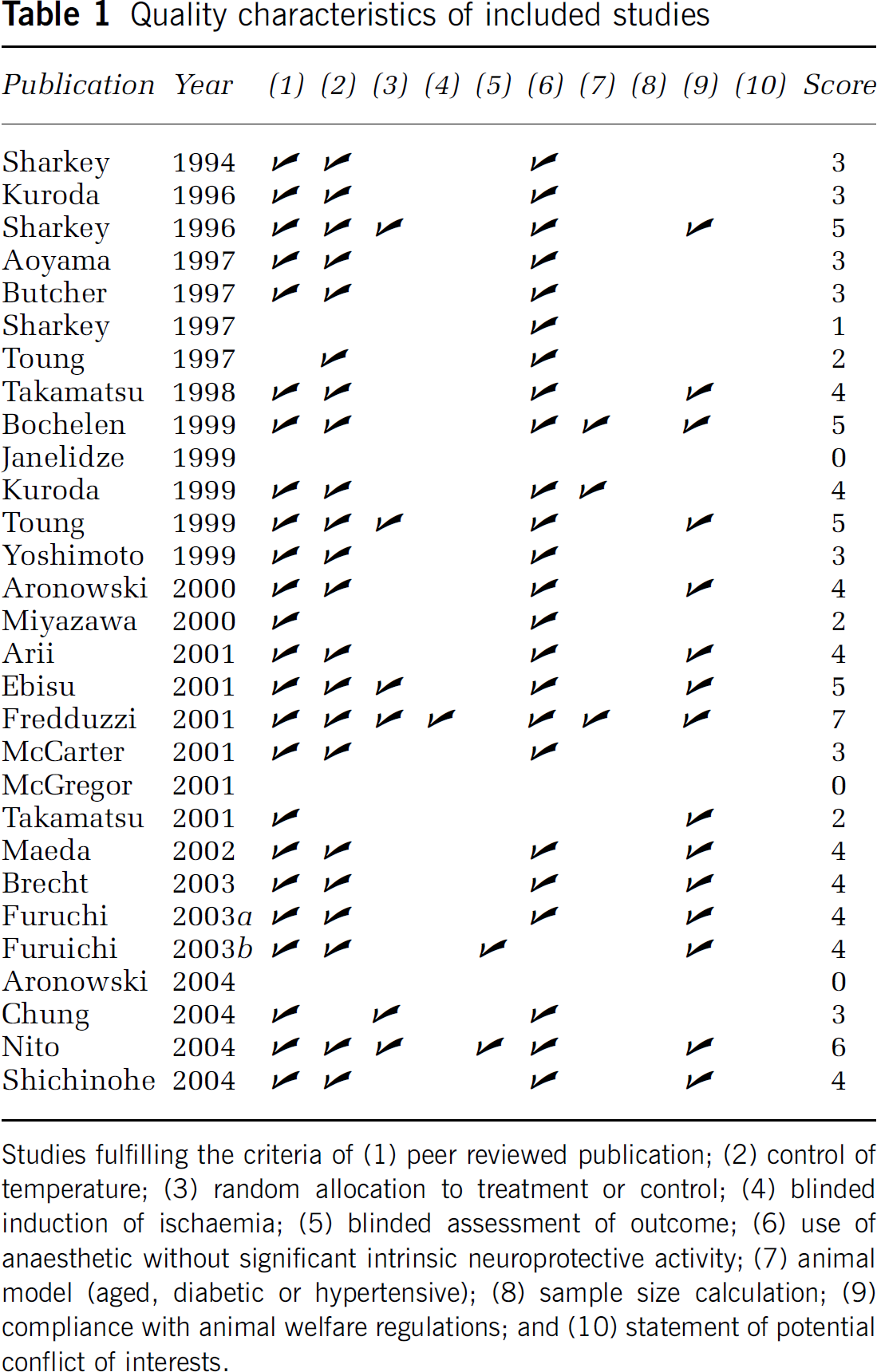
Studies fulfilling the criteria of (1) peer reviewed publication; (2) control of temperature; (3) random allocation to treatment or control; (4) blinded induction of ischaemia; (5) blinded assessment of outcome; (6) use of anaesthetic without significant intrinsic neuroprotective activity; (7) animal model (aged, diabetic or hypertensive); (8) sample size calculation; (9) compliance with animal welfare regulations; and (10) statement of potential conflict of interests.
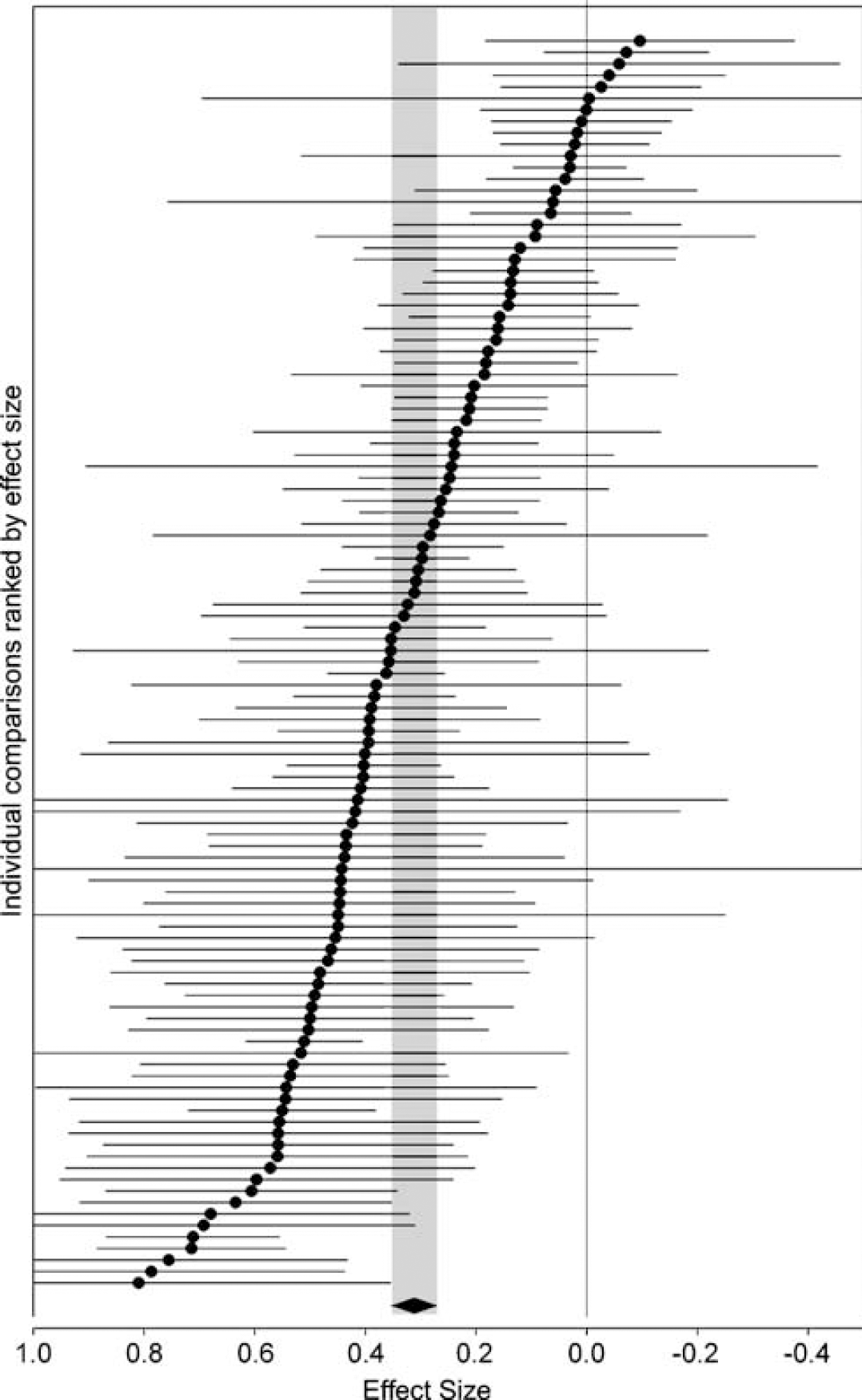
Point estimate and 95% CIs for global estimate and each of 109 comparisons ranked by effect size. Effect size is the improvement in treated animals expressed as a proportion of the outcome in control animals. The diamond indicates the global estimate and its 95% CI, also shown as the grey band. The solid vertical line marks where treatment and control are equal.
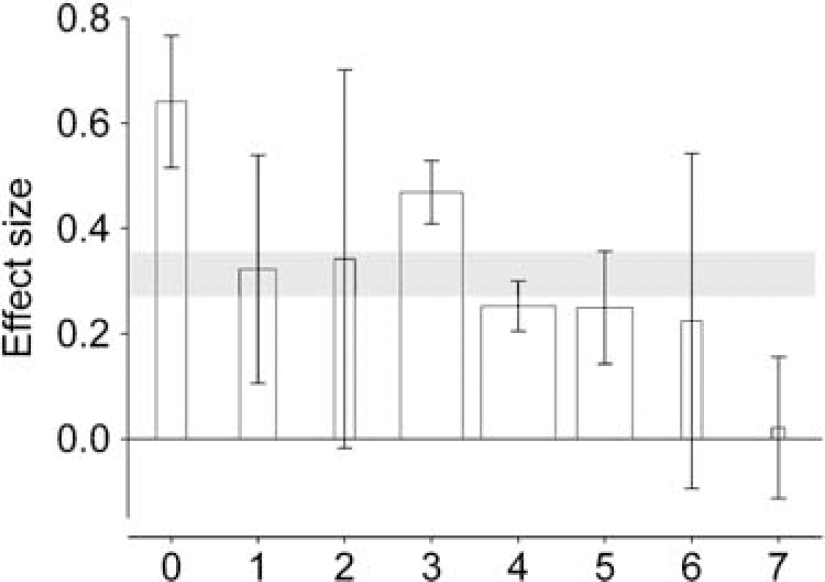
Point estimates and 95% CIs of effect size by reported study quality score. The thickness of each bar reflects the number of comparisons contributing to that data point. The 95% CI for the global estimate is again shown as a grey band. There is a significant relationship between reported quality score and effect size.
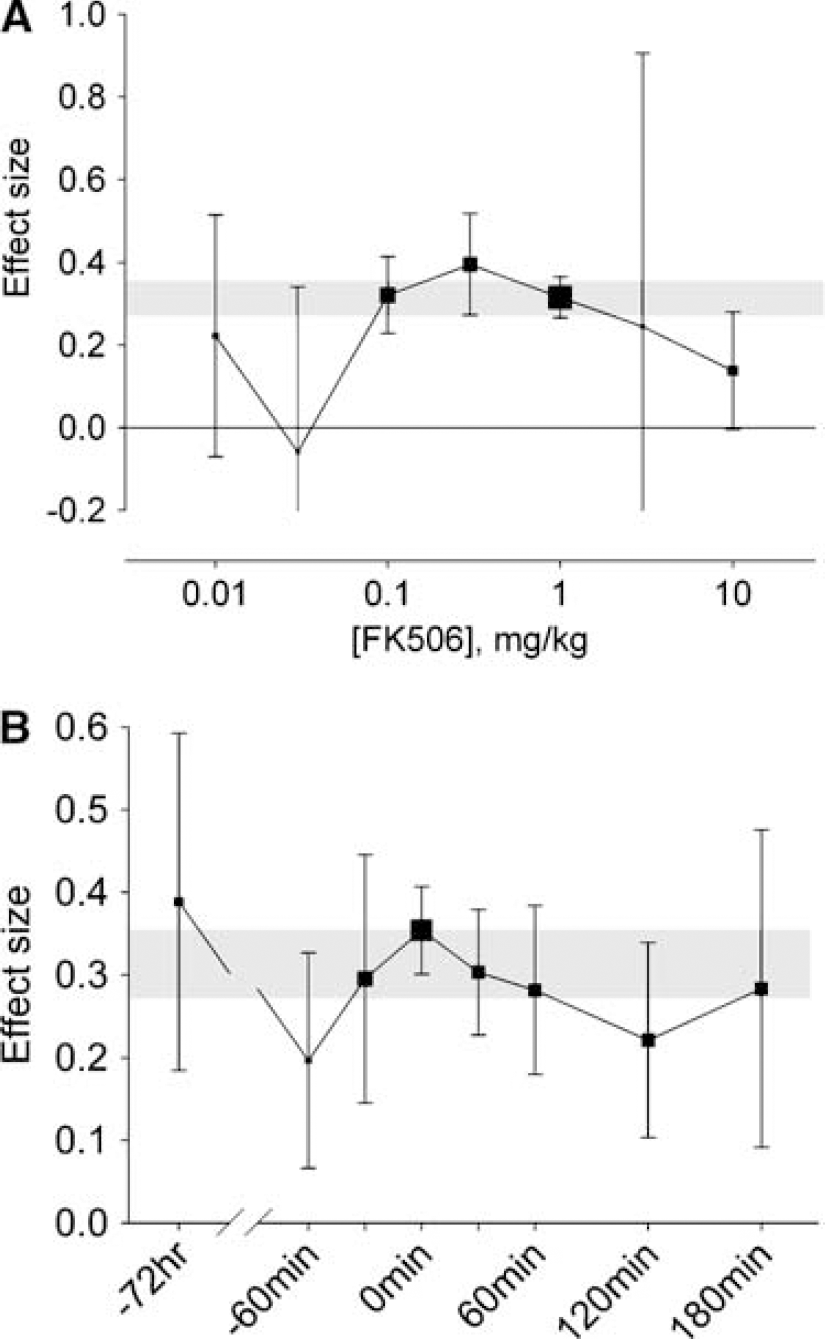
Significant protection was seen for all doses of FK506 above 0.03 mg/kg, with doses above 3 mg/kg giving less protection than intermediate doses (Figure 3A). Significant protection was also seen for all time points, with no apparent interaction between time of administration (up to 5 h post occlusion) and effect size (Figure 3B).
Point estimate of effect size and 95% CIs by (
Study design characteristics are shown in Table 2. Effect size was significantly higher in temporary ischaemia models (Figure 4A: χ2=52.3, df=3, P<10−10) and in studies using ketamine anaesthesia (Figure 4B: χ2=102.8, df=5, P<10−19). Experiments using MRI measures of infarct size gave more conservative estimates of effect size than those using histological measures of infarct size, and these in turn were more conservative than those using a combined outcome score or mortality (Figure 4C; χ2=86.0, df=3, P<10−18). Furthermore, the time at which outcome was measured was important; the longer the interval between ischaemia and measurement of outcome, the greater the effect size (Figure 4D; χ2=45.6, df=4, P<10−8).
Design characteristics of included studies
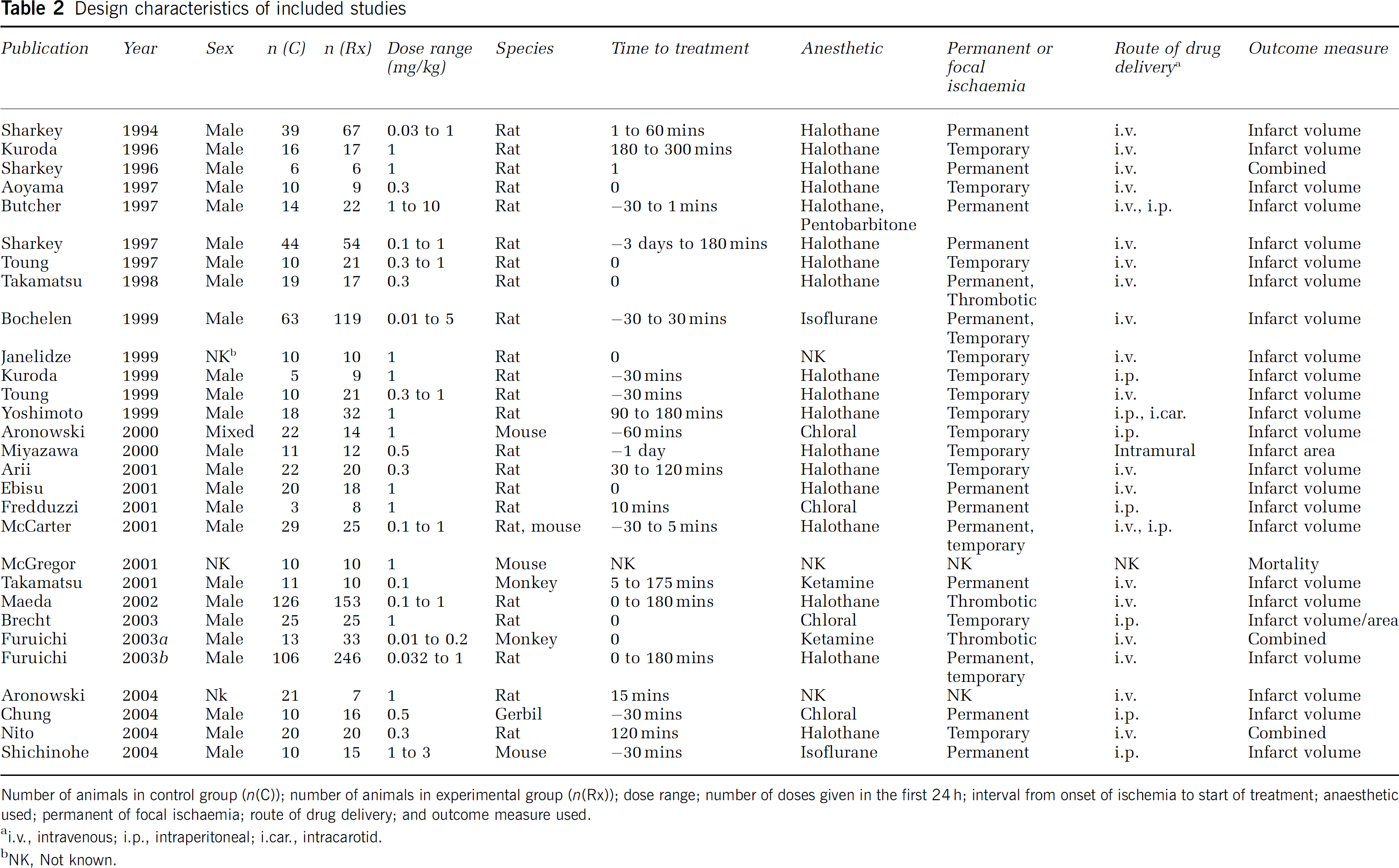
Number of animals in control group (n(C)); number of animals in experimental group (n(Rx)); dose range; number of doses given in the first 24 h; interval from onset of ischemia to start of treatment; anaesthetic used; permanent of focal ischaemia; route of drug delivery; and outcome measure used.
i.v., intravenous; i.p., intraperitoneal; i.car., intracarotid.
NK, Not known.
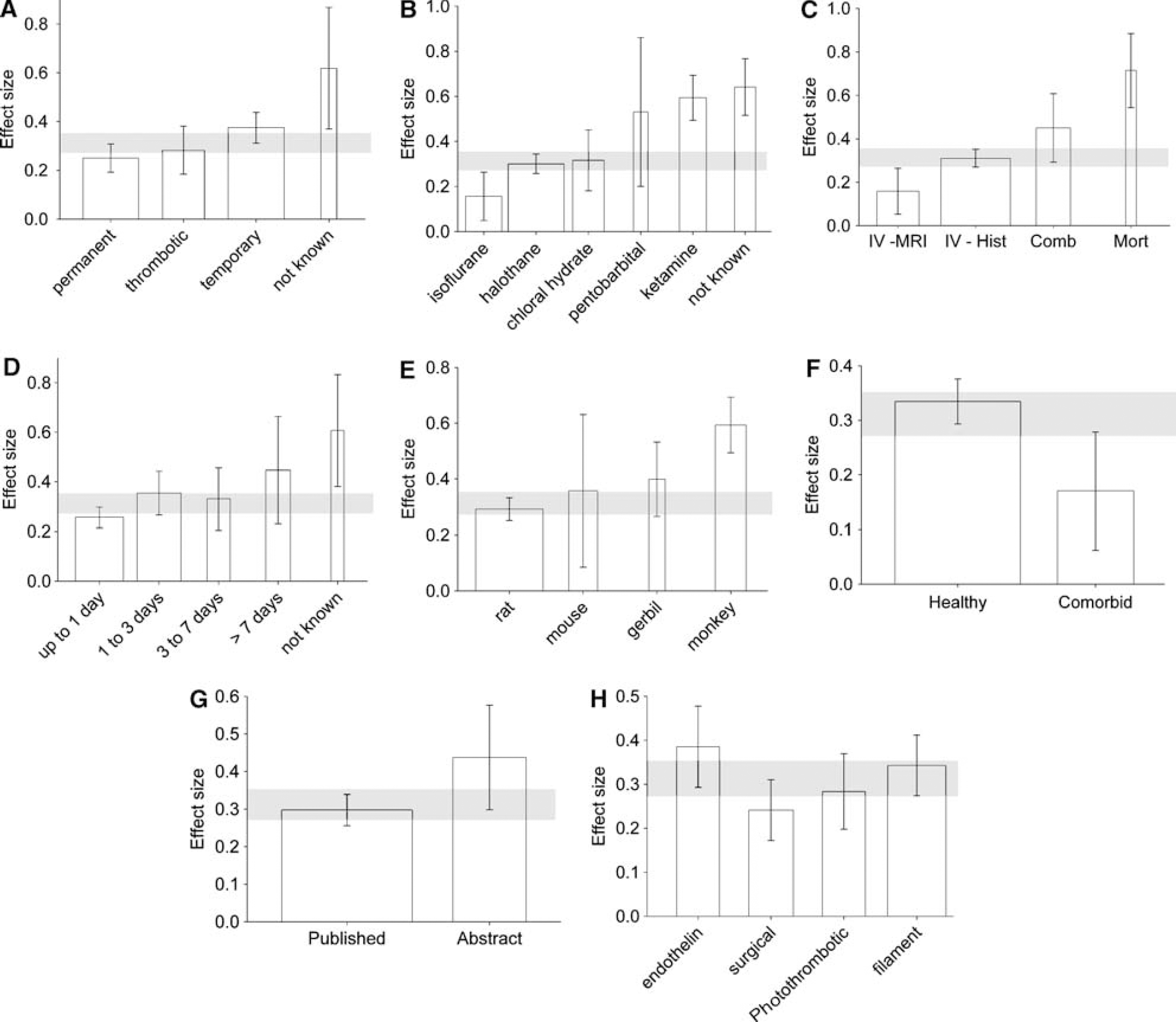
Point estimate of effect size and 95% CIs by (
Experiments on monkeys gave a higher estimate of effect size than those using rodents (Figure 4E; χ2=51.4, df=3, P<10−10), and effect size was higher with healthy animals (Figure 4F; 0.333, 0.299 to 0.368) than where hypertensive or hypoglycaemic animals were used (0.170, 0.079 to 0.261; χ2=44.8, df=1, P<10−10). Studies published in abstract only gave a higher estimate of effect size (Figure 4G; 0.436, 0.309 to 0.563) than those published in full (0.297, 0.263 to 0.332: χ2=21.6, df=1, P<10−5).
There was no increase in effect size in studies using multiple doses of FK506 (0.518, 0.334 to 0.703 versus 0.309, 0.274 to 0.343; χ2=4.6, df=1, P=0.03) or in studies using FK506 alone rather than in combination with other interventions such as tPA, magnesium or hypothermia (0.322, 0.285 to 0.358 versus 0.201, 0.135 to 0.266; χ2=6.2, df=1, P=0.01); while there was a trend for effect size to be higher with endothelin and filament models and lower with photothrombotic and surgical (occlusion by dividing artery or the external application of thread or aneurysm clip) models (Figure 3H; χ2=12.8, df=3, P=0.005), this did not reach our prespecified significance level.
Discussion
Treatment with FK506 lead to a substantial and highly significant improvement in outcome of more than 30%, and improved outcome was seen for all doses of FK506 above 0. 03 mg/kg and at each time point studied. Maximum effect size was seen with doses of 0.1 to 0.3 mg/kg administered within the first 30 mins of the onset of ischaemia, and FK506 was effective even when administered 3 days before the onset of ischaemia. The effective dose of FK506 is clinically relevant, being equivalent to that used long term in humans for immunosuppression after renal transplantation (0.2 mg/kg/day) (Murphy et al, 2003).
There are a number of potential difficulties with our approach: Firstly, our analysis can only include available data, and if negative studies are less likely to be published then this metaanalysis will overstate effect size. Furthermore, any bias (due perhaps to nonrandomisation or unblinded assessment of outcome) in individual studies will be reflected in the metaanalysis. Secondly, stratified metaanalysis remains a form of subgroup analysis. The stratifications reported here were prespecified, all analyses have been reported, and our stringent significance level accounts for multiple testing; nonetheless, some of our results might have arisen by chance and our data should be interpreted with caution.
Thirdly, it has been argued that drug efficacy in animals should be assessed against behavioural rather volumetric end points (Stroke Academic Industry Roundtable, 1999). However, there is little evidence to show that this approach leads to better prediction of efficacy in clinical trial, and in fact in humans lesion volume determined by MRI diffusion-weighted imaging shows correlation both with impairment at 24 h (Tong et al, 1998) and with clinical outcome (Wardlaw et al, 2002; Engelter et al, 2003), although the relationship for lesion volume determined by CT is less clear (NINDS, 2000).
Similarly, we have aggregated data for outcome measured as infarct size and neurobehavioural outcome. Only four of 108 comparisons reporting infarct size measured an area of infarction rather than a volume; converting these areas of infarction to volume (assuming a spherical infarct) increased the overall estimate of effect size from 31.3% (27.2% to 35.4%) to 31.7% (27.5% to 35.8%), and similarly had a negligible effect on the stratified metaanalyses. More difficult is the combination of data from histological and neurobehavioural end points. Importantly, neither of these are themselves ‘pure’, instead representing an amalgam of either different histologic methods or of different neurobehavioural scores, and all are intended to measure the single entity of neuroprotective efficacy. Different outcome measures reflect different aspects of efficacy, and our aggregate estimate represents the best estimate of overall efficacy based on all the available evidence.
Finally, there is a conflict between including only studies of high technical quality and including all available studies (to minimise the risk of publication bias described above). As the metaanalysis technique weights each study by its s.d. the model does take some account of technical quality; labs which replicate their results with high fidelity will report low s.d.'s and their data will be given more weight in the metaanalysis.
Our analysis suggested that the use of ketamine anaesthesia leads to an absolute overestimation of effect size of around 30%. This is in keeping with its known actions as a noncompetitive NMDA antagonist (Martin and Lodge, 1985), with reports of synergistic activity with putative neuroprotective drugs (Chang et al, 2002), and with our findings for both nicotinamide (Macleod et al, 2004) and melatonin (Macleod et al, in press).
Effect size was lower in permanent rather than temporary ischaemia models; it might be that FK506 inhibits more effectively those pathophysiological pathways preferentially activated on reperfusion. Effect size was lower in animals with comorbidities, consistent with our findings for nicotinamide. However, most of these data come from the genetically distinct spontaneously hypertensive rat (SHR) strain, and it might be that the reduced effect size is a consequence of genetically determined factors other than blood pressure.
Effect size was higher in monkeys than in rodents, and it might be that this gives a better indication of potential efficacy in human stroke. It is widely held that primate ischaemia models provide a more useful guide to clinical efficacy, but because no neuroprotective agent has unequivocal efficacy in human stroke it is not possible to test this hypothesis.
The global estimate of the efficacy for FK506 is similar to that of nicotinamide (28.7% (Macleod et al, 2004)) and lower than that of melatonin (42.8% (Macleod et al, in press)). However, the melatonin literature does not include any animals with comorbidity, and because of differences such as these we believe that comparisons of these global estimates are invalid. Where there is a sufficient range of data, it might be possible to use regression modelling to approximate differences in effect size, but a more reliable estimate would require individual head-to-head studies.
True study quality is often higher than the score allocated from details available in the publication, particularly for publications available only in abstract. For instance, the quality score of one paper increased from 1 in abstract (Nito et al, 2002) to 6 on full publication (Nito et al, 2004). It is clearly difficult to convey experimental detail in the space available in Abstracts, and even in full publication constraints of space may militate against a complete description of the steps taken to minimise bias.
Reported study quality was similar to that for nicotinamide (Macleod et al, 2004) and melatonin (Macleod et al, in press), and grouping studies by reported study quality accounted for a degree of the heterogeneity between studies, with high-quality studies reporting smaller effect sizes. Importantly, these reports include some which describe work performed over 10 years ago, and it would be invidious to judge these publications against standards which had not gained wide acceptance until many years later. However, study quality is a potentially crucial issue. Bebarta et al (2003) have shown that studies reporting randomisation and/ or blinding are less likely to report positive findings than those which do not; the extent to which such deficiencies in study design might have led to the overestimation of the effect of FK506 is not known.
Our quality score is an empirically derived, ordinal scale, which seeks to measure study quality. It does appear to have some validity, because classifying comparisons by quality score accounts for a substantial proportion of the heterogeneity observed in each drug metaanalysis thus examined to date. The importance of individual scale items, and the possible contribution of alternative items, is the subject of ongoing research. In the meantime, we suggest that, where possible, investigators adopt these measures. Although some criteria (e.g. blinding) might be difficult to achieve in small scientific groups, developments in study design (for instance, randomising to treatment group after the induction of ischaemia) may help circumvent some of these problems.
Criteria have been published for reporting clinical trials (Moher et al, 2001), and we support the development of similar criteria for reporting experiments in focal cerebral ischaemia, compliance with which could be stated in full publication or abstract at minimal cost in space. We propose that these criteria should be (a) compliance with local legislation or guidelines regarding animal experimentation; (b) prespecified statement of sample size; (c) control of temperature; (d) randomisation to treatment or control; (e) induction of ischaemia and (f) determination of outcome performed masked to treatment allocation; and (g) disclosure of any potential conflict of interest and (h) the avoidance of anaesthetic agents with marked intrinsic neuroprotective activity.
While the overall results of this metaanalysis suggest that FK506 has substantial effect size, the decline in effect size seen with increasing reported study quality coupled with the possible influence of publication or other bias raise concerns that the true efficacy for FK506 might be substantially lower than reported here. Further large studies of high methodological quality (including randomisation to treatment group, and masked induction of ischaemia and assessment of outcome) are required to give a precise, unbiased assessment of the efficacy of FK506. Based on our observations, to have 80% power to estimate the percentage improvement in outcome after treatment to the nearest 10% would require 115 animals per group. Such sample sizes may seem large, but the use of smaller cohorts represents a false economy and results are likely to be misleading; ultimately more animals would be required.
This report adds to the existing data from systematic review and metaanalysis in the assessment of putative neuroprotective drugs. Using this approach, we now have data for 3092 animals from 208 individual comparisons. With the addition of further data, multiple regression modelling should allow identification of those factors which have greatest impact on estimates of effect size. In turn, this may allow identification of a subset of variables which are sufficient to describe the properties of an administered drug, potentially reducing the number of experiments needed to characterise that drug. Where drugs or groups of drugs depart from the derived model, this may reflect distinct in vivo properties of those drugs, and this could provide the basis for a system of drug classification based on in vivo rather than in vitro or ex vivo characteristics.
Footnotes
Acknowledgments
We are grateful to the authors of included studies for their assistance in conducting this metaanalysis, and in particular to John Sharkey, for helpful and insightful discussions.