
Abstract
Stem cell therapy has showed considerable potential in the treatment of stroke over the last decade. In order that these therapies may be optimized, the relative benefits of growth factor release, immunomodulation, and direct tissue replacement by therapeutic stem cells are widely under investigation. Fundamental to the progress of this research are effective imaging techniques that enable cell tracking in vivo. Direct analysis of the benefit of cell therapy includes the study of cell migration, localization, division and/or differentiation, and survival. This review explores the various imaging tools currently used in clinics and laboratories, addressing image resolution, long-term cell monitoring, imaging agents/isotopes, as well as safety and costs associated with each technique. Finally, burgeoning tracking techniques are discussed, with emphasis on multimodal imaging.
INTRODUCTION
Disruption of blood flow to the brain during stroke is the third leading cause of death in the United States, with 800,000 new cases presenting each year, and an estimated annual cost of $60 billion. 1 Early restoration of blood flow is crucial, yet at present, only clot-busting tissue plasminogen activator has FDA (Food and Drug Administration) approval for treatment in acute stroke. As of 2015, over 3,000 clinical trials have either been undertaken or are in progress (http://www.Strokecenter.Org/trials/clinicalstudies/list.2015). Potential therapeutic compounds have targeted different stages of stroke progression, including: excitatory cell death2,3 and inflammation/ischemia-reperfusion injury, 4 as well as trials aiming to reduce the risk of a subsequent stroke 5 —none has proven successful.
Conversely, preclinical studies and early-phase clinical trials indicate that the use of stem cells offers a promising reparative strategy for acute ischemic brain injury. A variety of stem/progenitor cell types are being investigated for their therapeutic potential, including: mesenchymal, hematopoietic, neural and adipose-derived progenitor cells, induced pluripotent stem cells and cell lines (see Liu et al 6 for table of current trials). Although the precise mechanism underlying the benefit of stem cell transplantation remains to be determined, it now seems unlikely that these cells are able to replace lost neuronal circuitry directly in humans as initially proposed. In fact, they appear to function as microfactories for a protective cocktail of neurotrophins, growth factors, and other substances that induce restorative processes (e.g., angiogenesis, neurogenesis, and synaptogenesis), and antiinflammatory mediators.7,8 The ability of stem cells and their secretions to improve outcomes after stroke has been shown extensively through improvement in a variety of outcome parameters studied in animal models: decreased infarct volume and pro-inflammatory biomarker expression,9,10 increased anti-inflammatory biomarker(s)11,12 and growth factor expression, 13 improved functional recovery,15,16 inhibition of glial scar formation,1719 and increased angiogenesis.7,17 These outcomes offer convincing, yet relatively crude measures of the healing capacity of stem cells, as each provides only indirect evidence of beneficial stem cell activity.
Precise mechanistic understanding involves the study of cells in vivo, following administration to an animal, alongside complementary imaging of stroke pathology itself. 20 Observing cell migration, localization, division and/or differentiation, cell survival and protein release or expression will enable optimization of a therapy that already shows considerable promise. Several questions require the use of a range of in vivo imaging technologies to provide an answer: do therapeutic stem cells end up in the brain? If not, can we engineer an environment to attract more there? What protective substances do they release? Are these substances different depending on the location of the cells? How long do transplanted cells survive and what do they turn into? Does this vary with respect to the source of therapeutic stem cells? Is one more effective than the other? Many of these aspects were reviewed in 2012 by Adamczak and Hoehn. 21 In this review, we provide an update on significant advances and improvements in the field, as well as comprehensive selection guides for researchers and clinicians. Specifically, we discuss the recent advances in neuroimaging technologies (many of which we use in our laboratory to answer the above questions) that facilitate the study of these cellular activities in humans and animal models. We will also address image resolution, long-term cell monitoring, imaging agents/isotopes, as well as safety and costs associated with each technique. Finally, burgeoning tracking techniques are discussed, with emphasis on multimodal imaging.
CELL TRACKING TECHNOLOGIES: OVERVIEW
The first methods for cell tracking relied on analysis of the differential expression of surface markers on stem cells versus endogenous cells,22,23 and therefore involved killing many animals to fulfill sufficient time points for a longitudinal study. The use of positron emission tomography (PET), single-photon emission computed tomography (SPECT), magnetic resonance (MR) imaging (MRI), and optical imaging minimizes the number of animals required for each study. More informative data are produced, as each animal can be used as its own control (i.e., prestroke and at various stages after stroke) in longitudinal experiments. Depending on the species used, behavioral improvements can be difficult to measure accurately and objectively, and small improvements are disguised if a single animal cannot be observed over days. However, the longitudinal, noninvasive nature of behavioral tests provides means for obtaining information that complements imaging well.
The scope of PET, SPECT, MRI, and optical imaging is discussed in the following sections. Facilities permitting, none of these is considered universally preferential. Each has benefits with respect to image resolution, long-term stem cell monitoring, sensitivity of imaging agent, duration of image acquisition, suitability for clinical use, and cost. Appropriate selection of a technique must consider the relative importance of each of these. For example, forms of bioluminescent optical imaging theoretically allow for stem cells to be imaged indefinitely (providing information about the dynamics of stem cells, such as location, migration, and proliferation), and can be performed at a relatively low cost, but due to the low penetration of light from bioluminescent cells, 24 this imaging modality is constrained with respect to the depth of tissue that can be observed. Conversely, PET, SPECT, and MRI are able to detect stem cells deep within a subject, but either require the use of a radioactive isotope that may damage the functionality of cells (PET/SPECT), 25 or typically have low sensitivity (MRI). 26 Efforts are underway to overcome these restrictions (discussed in the sections below), through improved cell-labelling techniques and by combining modalities so that one may accommodate the shortfalls of another (multimodal imaging). The following sections describe the principles and practicalities of these methods clinically and preclinically and are summarized in Table 1.
Imaging modalities currently available for tracking stem cells in stroke
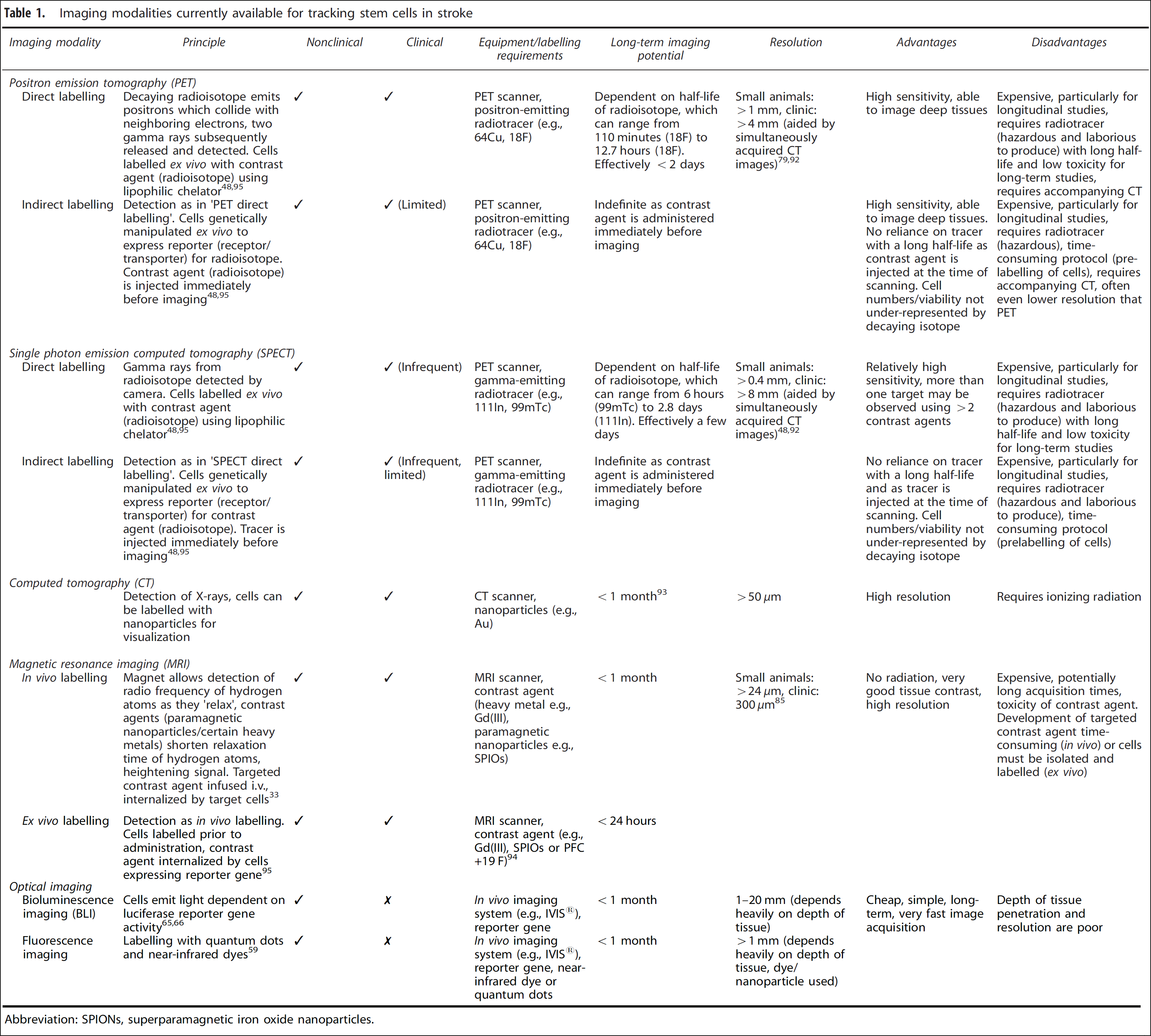
Abbreviation: SPIONs, superparamagnetic iron oxide nanoparticles.
MAGNETIC RESONANCE IMAGING: IMAGING WITH MAGNETISM
The localization of therapeutic stem cells to an infarct after stroke is widely studied under the premise that successful transplantation relies heavily on targeted cell delivery. Magnetic resonance imaging has been used to confirm successful (or unsuccessful) cell migration,27,28 to provide a quantitative assessment of various routes of administration (for example, intravenous versus intraarterial) 29 and to identify potential safety concerns associated with each route. 30 Whether one stem cell source if more suited than another to localize to an infarct is also of great interest. To date there have been very few studies directly comparing stem cells from various sources for stroke therapy, 31 and none comparing their ability to localize at an infarct. Magnetic resonance imaging presents an exciting opportunity for conducting such research.
Classical MRI enables the observation of structural aspects of a subject with respect to the diffusion patterns of water through tissue. Images are acquired through the detection of radio frequency waves emitted from the hydrogen atoms within water, as the protons within hydrogen—acting as local magnets—are excited then ‘relax’ following the application of a pulsed magnetic field to the subject (Figure 1A). In order for MRI to be useful in imaging at the cell and molecular level, this detection process must be enhanced through the application of either a contrast agent or superparamagnetic nanoparticles. These are either T 1 or T2 agents depending on whether they affect the longitudinal (T1), or transverse (T2), relaxation times of water. Clinical MRI systems have magnetic field strengths ranging from 0.2 to 7 Tesla (T), the majority of machines functioning at 1.5 T, 32 whereas small rodent systems operate using greater field strengths −4.7 to 11.7 T. 33 4.7 T machines and above enable the acquisition of higher resolution images with lower cell detection limits, and are required to generate sufficient resolution to image detail of an ~ 25 g (versus ~ 80 kg) animal.
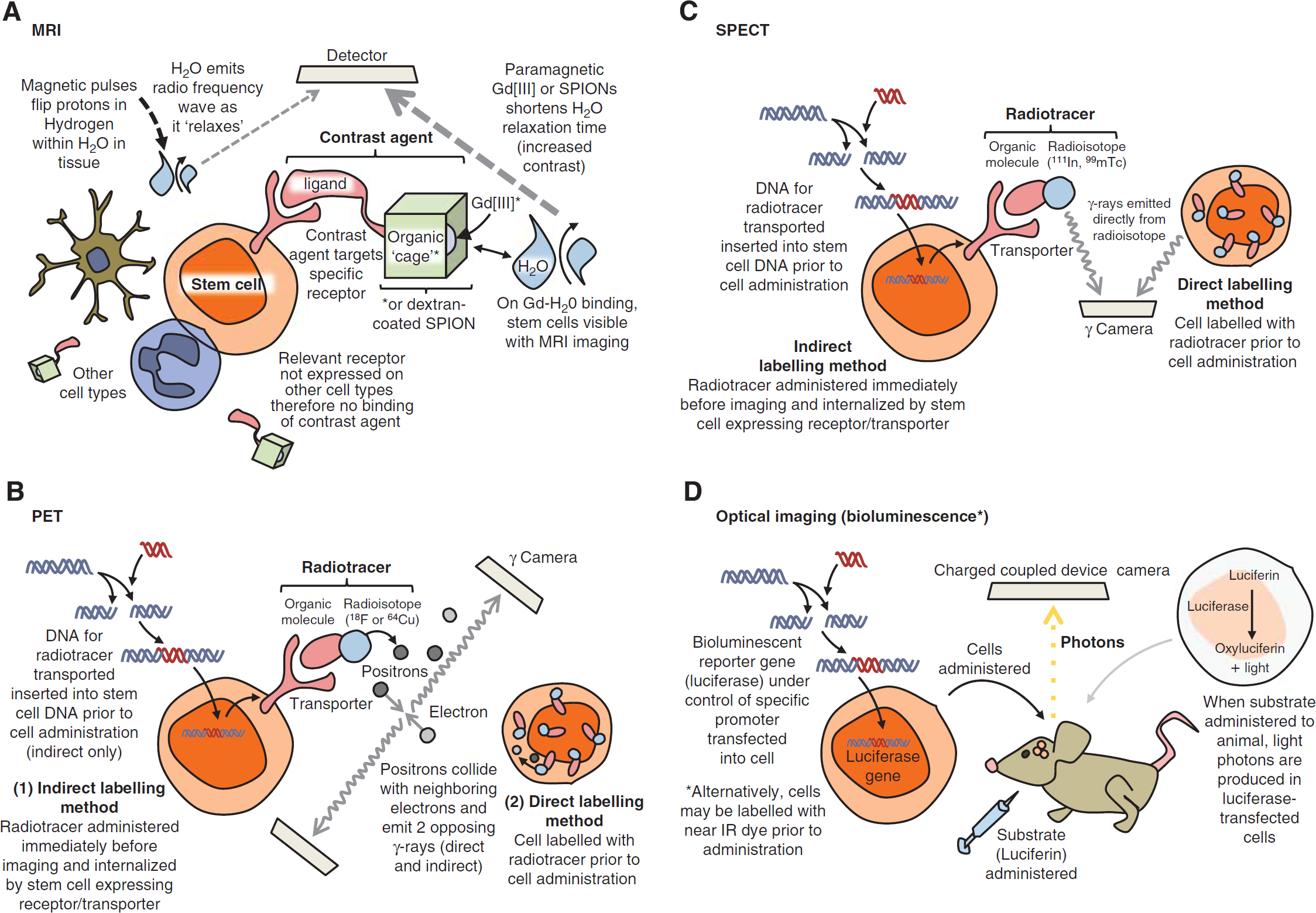
Principles of stem cell labelling for different imaging modalities. (
Recently, MRI has become highly useful in real-time, noninvasive imaging of stem cell activity. 34 Gadolinium chelates and iron oxide particles are currently the best contrast agent candidates to label cells for MRI, because they are well tolerated when injected directly into the blood.35–37
Gadolinium (III) (Gd[III]) is a heavy metal widely used in humans38,39 and experimentally40,41 as an ionic base for T1 contrast agents. Gd(III) enhances image contrast—i.e., the variation in grayscale—due to its ability to act as strong local paramagnet and therefore increase the relaxation rate of surrounding water molecules. Paramagnetism, whereby a substance is attracted to a magnetic field, relies on the existence of unpaired (free) electrons, and the strength of that attraction is correlated to the number of free electrons. (Diamagnetism is the opposite, whereby a substance with no free electrons is repelled from a magnetic field.) The paramagnetic properties of Gd(III) are highly potent: free electrons are nearly 700 times stronger than protons (the source of paramagnetism in MR images related to water content) as local magnets, and Gd(III) has seven free electrons. 42 The contrast of an image acquired with the use of Gd(III) is therefore enhanced approximately 5,000 times above what can be achieved without a contrast agent. 42
Gd(III) is highly toxic as a solubilized-free ion43,44 and so is chelated before use. The ability of Gd(III) chelates to enhance image contrast can be exploited further to observe specific cells, through modification of the chelate. A ligand that selectively binds to receptors on cells of interest may be covalently bound to the Gd (III) chelate, enhancing image contrast in the vicinity of the target cell/receptor (Figure 1A and Stasiuk et al 45 ). In addition, Gd(III) chelates are able to label stem cells with the use of a transfection agent and have been used in research for several years, 46 and more recently, Gd(III) ions have been used in nanoparticles to provide an even greater contrast enhancement.34,47
Where Gd(III) is considered as a paramagnet, superparamagnets have a larger susceptibility to magnetization 48 and so are excellent candidates for contrast enhancement in MR images. 49 The most commonly used superparamagnets are superparamagnetic iron oxide nanoparticles (SPIONs). 49 In addition to their ability to enhance T2 relaxation time of water, SPIONs have the benefit of being largely biologically compatible 50 (they are safely removed by existing metabolic pathways in cells) and can be detected using light and electron microscopy.51,52
Currently, many commercially available SPIONs are used in conjunction with a transfection agent, which may be toxic at certain levels either through cell death or prevention of cell division. 53 As a result, there has been a drive over the last decade to produce alternative coatings that facilitate the administration of SPIONs to cells without the use of a transfection agent. 49 Production of alternative coatings has also been driven by a more familiar magnetic trait of SPIONs: they have a tendency to clump together. Coating SPIONs with dextran or dextran derivatives is one method used to overcome this. 55 (Other surfactant-like coatings for SPIONs include glycosaminoglycans, starch, polyethyleneglycol, siloxane, and poly-lactic acid. 56 ).
Superparamagnetic iron platinum particles are precursors to iron-platinum-based nanoparticles currently synthesized for use in magnetic storage devices. These precursors exhibit magnetic moments superior to those of SPIONs, suggesting that they may form the basis of excellent contrast agents. 57 Superparamagnetic iron platinum particles have yet to be used to label stem cells in stroke treatment, and have yet to undergo extensive toxicity studies, but have been used successfully in targeting prostate cancer cells with up to 13 times the specificity of commercially available SPIONs.58,59
In addition to the development of more sensitive contrast agents and increased magnetic field strengths, increased resolution is being achieved through various means. Improving the system machinery by, for example, increasing the number of coil receiver channels or the magnetic field strength can increase signal strength. 60 Longer acquisition times also increase resolution, although this may be hampered by the susceptibility of patients to claustrophobia, or the length of time tolerated by an animal in the machine. 61 Should cost, time available for image acquisition, or movement of a subject be prohibitive, imageprocessing techniques can be applied postscanning. These usually rely on algorithmically combining several independent acquisitions of the same subject.
Magnetic resonance imaging is not without limitations: contrast agents can remain within injured tissue beyond the life span of the therapeutic cells, continuing to produce detectable signals and thus making discrimination between live and dead cells impossible.62–64 The use of indirect cell labelling methods (mentioned in the following section in conjunction with PET/SPECT) avoids this problem by requiring that a contrast agent be injected immediately before imaging. Where cells are directly labelled before administration, the metabolism/clearance of the contrast agent from tissue should be accounted for by assessing the retention of a contrast agent by transplanted viable, versus dead cells. 65 Contrast agents may also be diluted due to cell division, especially when cells are rapidly dividing. However, novel transfection agents and indirect labelling methods (see below, PET and SPECT) aim to overcome the limitations of MRI stem cell tracking in stroke and other neurological disorders.
POSITRON EMISSION TOMOGRAPHY AND SPECT: IMAGING WITH RADIOACTIVE TRACERS
Both PET and SPECT require a radiotracer (a compound containing a radioactive isotope) to label the desired cell type in order for cells of interest to be detected by a scanner. In PET imaging, the tracer contains a radioactive isotope that emits positrons (the antiparticles of electrons), which cause emission of two or more divergent gamma rays (high frequency photons) on annihilation with surrounding electrons as little as 1 mm away (Figure 1Band Khalil et al 66 ). These gamma rays are detected simultaneously by two opposing gamma cameras in a PET scanner as an indirect, high-resolution measure of the extent of cell localization or functional activity within a subject. Since PET images are created only where tracer is detected, scanning is often performed in conjunction with computed tomography (CT), which provides structural orientation for the PET images.
The key advantage of PET imaging over SPECT is increased sensitivity (by approximately two or three orders of magnitude). This is because SPECT imaging utilizes tracers that produce gamma rays directly rather than as a result of positron-electron annihilation (Figure 1C), which are detected by just a single gamma camera (although multiheaded cameras exist for accelerated acquisition of images). In both techniques, cameras rotate about a subject, recording gamma intensity every 3 to 6 degrees over each 360-degree rotation. Through this method, sequential tomographic 2D images are acquired through an axis of a subject, and constructed into a 3D interpretation of the recorded radioactivity. If radiolabelled stem cells are administered after stroke, these 3D acquisitions indicate the locations in which the tracer is most concentrated, and hence areas to which most cells have migrated. While physical aspects such as positron range and photon noncollinearity (the tendency of photons to deviate from annihilation at 180 degrees) limit PET resolution, SPECT resolution can be increased by improvements to equipment (for example, the beam-narrowing collimator). 67 Technological advances are therefore being made to enhance image resolution in SPECT, such as pinhole SPECT and μSPECT systems (containing many pinholes), which are able to produce a spatial resolution of less than 1 mm,68,69 and offer the possibility of small animal SPECT imaging.
To study stem cell migration in stroke using PET/SPECT, cells may be labelled directly or indirectly with a radiotracer. Direct labelling is the most common: a tracer is retained within a lipophilic chelator (an organic structure or ‘cage’) that is able to enter cells of interest when applied ex vivo (Figure 1B). Once cells have been labelled, they can be administered to a subject. Labelling ex vivo in such a way does not distinguish between healthy and dying cells, as a radioisotope will decay (and therefore be detected) irrespective of the cellular environment. In addition, imaging over a long period of time means that decaying of the radioisotope may underrepresent the concentration of cells in a given area, or falsely indicate that the cells of interest are undergoing division. These two occurrences would be indistinguishable from each other: an isotope will inevitably produce a weakening signal relative to the volume of cells present over time, but the amount of tracer in each cell is divided after each cell division, and therefore also causes a weakened signal. Since it has been shown that both the number of cells administered and the timing of transplantation affect survival of transplanted cells, 70 and some studies are focused entirely on improving cell survival (with the use of scaffolds/matrices for example, Zhong et al 71 ), a means of discriminating between live and dead cells long term is highly desirable.
A better test of viability and cell concentration is through use of indirect labelling methods. These generally involve the genetic manipulation of cells ex vivo in order that they are able to produce an abundance of a particular protein involved in the uptake or accumulation of a tracer—a reporter protein.72,73 The tracer itself is then administered a defined period of time before imaging. The inclusion of genes in such a way means that only living cells will be identified, as unviable cells will no longer undergo protein synthesis and therefore be unable to generate the essential machinery for tracer uptake. Unlike direct labelling of cells, gene transfer methods are also able to indicate expansion of transplanted cells—there is no dilution of a tracer as cells divide, because a parent cell will supply each daughter cell with the same genetic material it uses to aid tracer uptake.
While possible, isolating and genetically manipulating cells, to label them indirectly, is considerably laborious if the technique is to be viable for cell tracking in the clinic. The use of PET for longterm imaging of stem cells in humans would be highly valuable, however, and searches for positron-emitting radioisotopes that can compete with the longer half lives of SPECT radiotracers are underway. Zirconium-based tracer, 89 Zr-oxinate4, for example, has recently been detected in cells up to 14 days after labelling and administration. 74 These properties are comparable to Indium-111 ( 111 In)-oxine, the gold-standard radiotracer for SPECT, which has been successfully used to monitor the migration and localization of CD34+ hematopoietic progenitor cells in rat models of myocardial infarction 75 and stroke. 76 In work by Brenner et al 77 and elsewhere, however, 111 In-oxine has been shown to affect the cellular integrity of hematopoietic progenitor cells. Reduced viability and proliferative capability reduce the potential for translation of this particular radiotracer, since the primary goal of therapeutic stem cells is that they are effective and not that they are of definitive whereabouts. 89 Zr-oxinate4 has also been shown to reduce cell viability by about 20% during the labelling process, although no further reduction is seen 24 hours later. It is evident that the use of a radioisotope is highly likely to affect cell function and/or toxicity. Identifying the maximum safe dose of a radiotracer is therefore crucial when developing modalities requiring a radioisotope for the clinic; for example, 18 F-fluoro-2-deoxy-D-glucose may used to label cells safely at concentrations up to 25 Bq/cell without compromising cellular function. 78
OPTICAL IMAGING
Optical imaging is used to improve the understanding of structural and functional components of stem cell therapy in preclinical stroke. Several fluorescent probes exist that are able to produce beautifully detailed images of stem cells within any tissue ex vivo. Recently, the use of fluorescent nano-diamonds (among other advanced probes) has even begun to overcome stalwart limitations of fluorescence imaging such as toxicity and background autofluorescence.79,80
The density of brain tissue, however, has always been an obstacle with individual cell tracking in fluorescence-based imaging techniques in stroke. As a result, the use of traditional fluorescent markers such as green fluorescent protein to label cells before administration after stroke is severely limited by the short wavelengths of such probes, and subsequent poor tissue penetration. To detect cells using fluorescence alongside current in vivo imaging systems such as IVIS®, probes in the near infrared (NIR) spectrum may be used. These penetrate tissue well and allow tracking of labelled cells, particularly in small rodents. Lipophilic NIR dyes have been shown to be useful in identifying the location of large numbers of stem cells after administration, even in deep tissue such as the brain in a 6-hydroxydopamine-induced rat model of Parkinson's disease. 81
Low tissue penetration of fluorescent labels (including NIR relative to other imaging modalities) makes optical imaging unfeasible for clinical use. Yet vastly improved acquisition time versus MRI and PET/SPECT, quick and simple cell-labelling protocols, and dyes that are long-lasting (1 month or more) with low toxicity and very good resolution (in particular with quantum dot-based fluorescent probes 82 ) form the basis of an informative, relatively cheap preclinical assessment of cell migration in vivo. The NIR-emitting quantum dots have been used successfully to visualize bone marrow stromal cells in traumatic brain injury in rats 83 as well as in a focal model of stroke 84 (the latter study observing NIR up to 8 weeks after stroke), indicating that NIR provides an excellent means for preclinical, long-term study of cell migration.
Bioluminescence imaging bares similar advantages and disadvantages to fluorescence imaging (it is quick and relatively cheap, but severely limited when imaging deeper tissue). Its use is also therefore confined to preclinical studies. Bioluminescence is light generated by intrinsic properties of certain bacteria, fireflies (Photinus pyralis) and the North American click beetles (Pyrophorus divergens) in nature.85,86 These properties, involving chemiluminescent enzymatic (luciferase) reactions, have been applied to stem cells through genetic manipulation before cell administration (Figure 1D). While the light cannot be seen from inside an animal under normal conditions, light from both fluorescent probes and bioluminescence is detected by charged coupled device cameras cooled to around −150°C, rendering them highly light sensitive. Like fluorescence imaging, bioluminescence can be used to study cells long term: neural progenitor cells have been observed 21 days after stroke in both rat 87 and mouse. 88
Ultrasound is not currently widely used in cell tracking strategies due to very low resolution in the unmodified technique. High-resolution images, however, have been achieved after the inclusion of gold nanoparticles, which alter the optical properties of cells that would normally be indistinguishable through ultrasound. 89 Interesting also is that—although not used in an observational capacity—ultrasound in conjunction with microbubbles has been used to enhance the delivery of therapeutic cells to injury sites. 90
MULTIMODAL IMAGING
As described above and in Table 1, imaging modalities have varied limits with respect to contrast/functional/spatial resolution, background interference, sensitivity, and specificity. Since no single technique is excellent through all these criteria, current imaging strategies make use of multiple modalities simultaneously, where facilities exist. Multimodal imaging integrates two or more techniques, exploiting the strengths and thereby overcoming limitations of each, and has been increasing in use rapidly over the last decade. Positron emission tomography/CT has been standard practice in the clinic for over a decade 91 and is an excellent example of how imaging techniques can be combined effectively. The CT produces anatomic images that, along with MR images, are unparalleled in revealing structural detail. Positron emission tomography, and to a lesser extent SPECT, is highly indicative of functional activity. Overlaying simultaneously acquired PET and CT scans therefore enables the integration of structural and functional information, clarifying results, and reducing the likelihood of misinterpretation of data or misdiagnosis in the clinic. More recently, studies exploit the advantages of other techniques, combining MRI with SPECT imaging 92 and PET with bioluminescence, 93 among other examples. The huge advantage of these combinatorial approaches is rapidly becoming apparent to institutions, which are investing in imaging equipment with the capacity to execute more than one imaging modality simultaneously. The PET/MRI imaging has received particular attention for its potential in neuroimaging. While this is currently an expensive technique requiring specialized equipment (of which manufacturers suggest, ‘if you build it, they will come’ . 94 ), PET/MRI imaging was deemed feasible by Schlemmer et al, 95 and provides a superb opportunity to combine anatomic, physiologic, functional, and metabolic information. 96
Multimodal systems that have emerged using PET, SPECT, MRI, CT, and optical techniques in various combinations often require cells, which have been genetically manipulated to express a protein that has a binding site for not one, but two to three probes, each catering to a different modality—a double/triplefusion protein. For example, using this approach, a protein has generated containing regions that report green or red fluorescent protein, luciferase and the HSV1-TK enzyme, enabling cells to be observed fluorescence, bioluminescence, and PET or SPECT. 97
TRANSLATING CELL TRACKING TECHNOLOGIES TO THE CLINIC
In 2011, academic and industry leaders in stroke research gathered to consolidate the most recent advances and emerging data relating to ‘Stem Cells as an Emerging Paradigm in Stroke (STEPS3)’ . In particular, barriers to successful translation of cell therapy from animal models to the clinic were discussed, and the need for excellent imaging tools highlighted as follows:
‘Use of imaging in clinical trials is strongly encouraged to provide as much information as possible to assess vascular/structural lesions, infarct size, cell viability, location, the success and safety of implantation, and inflammation. Imaging should also be used to monitor safety and recovery and, when possible, to investigate mechanisms of action and provide information on surrogate markers of treatment effect. Imaging measures might also be useful to help stratify patients at baseline.’ 98
Use of state of the art imaging in the translation of cell therapy is therefore extremely valuable. The use of small rodent models of stroke is highly useful in testing therapeutic strategies in a reproducible, relatively high-throughput mammalian model. Despite this, the small, lissencephalic rodent brain and cerebrovasculature are considerably different from those of a human, and their use in assessing the prospective efficacy of imaging technologies in the clinic is severely limited by the differences in machinery (for example: smaller aperture, higher resolution). Large animal stroke models are laborious and often complicated and expensive, but to some extent they bridge the gap between rodent models and humans. Canine, 99 sheep, 100 pig, 101 and nonhuman primate102,103 models therefore enable the viability of imaging modalities to be tested in a larger, more structurally complex brain, in larger, clinical scale (lower resolution) scanners, and as such their translational potential.
Testing imaging modalities in large as well as in small animal models will also enable the techniques to be used to assess the safety 30 and efficacy of treatments in humans, 104 targeted cell delivery, 29 and even cell migration directly. 105 Sequential imaging in particular may enable the detection of aberrant cell migration and/or proliferation.106,107
Despite their advantages (cheap, high-throughput), optical/bioluminescent imaging systems are not suitable for translation into large animal models or the clinic, as they are severely limited by the low penetration of light through tissue of substantial thickness. Since they are not hampered by tissue depth, PET, SPECT, and MRI have significant potential for use in the clinic, and studies specifically investigating the translation of these modalities (radiotracer dose expansion 108 , for example) are underway. There is a clear trajectory toward the use of μPET and μSPECT systems in particular, where resolution of < 0.5 mm can be achieved in rodent models, into large animal models and the clinic.68,69
WHAT SHOULD YOUR LAB BE USING?
This is a complex question, as it dependent on a number of different factors. Table 1 summarizes the principles, requirements/facilities, advantages, and disadvantages (including cost, resolution, and sensitivity), and other aspects of imaging modalities covered in this review (see Figure 2 for comparison of images and Figure 3 for an ‘at-a-glance’ guide to modality selection). Selection of imaging tools should be based on an assessment of the requirements of the study: are low cell numbers being used/is high sensitivity needed? Is morphological data/high spatial resolution needed? Is long-term/repeated imaging planned? Is the goal translation? Many imaging modalities are credited for their ability to be translated into the clinic—and rightly so. It should also be considered, however, that imaging protocols that are potentially detrimental to humans should not be overlooked, since they may be of use in preclinical studies: general priorities include keeping costs down in the laboratory and keeping safety high in the clinic; for example, while safety concerns with repeated doses of radiotracers may outweigh the advantages of long-term cell tracking in patients, the technique is extremely useful in the laboratory. Conversely, cost constraints in the laboratory may indicate the preferred use of optical imaging despite the low resolution in deeper tissues.
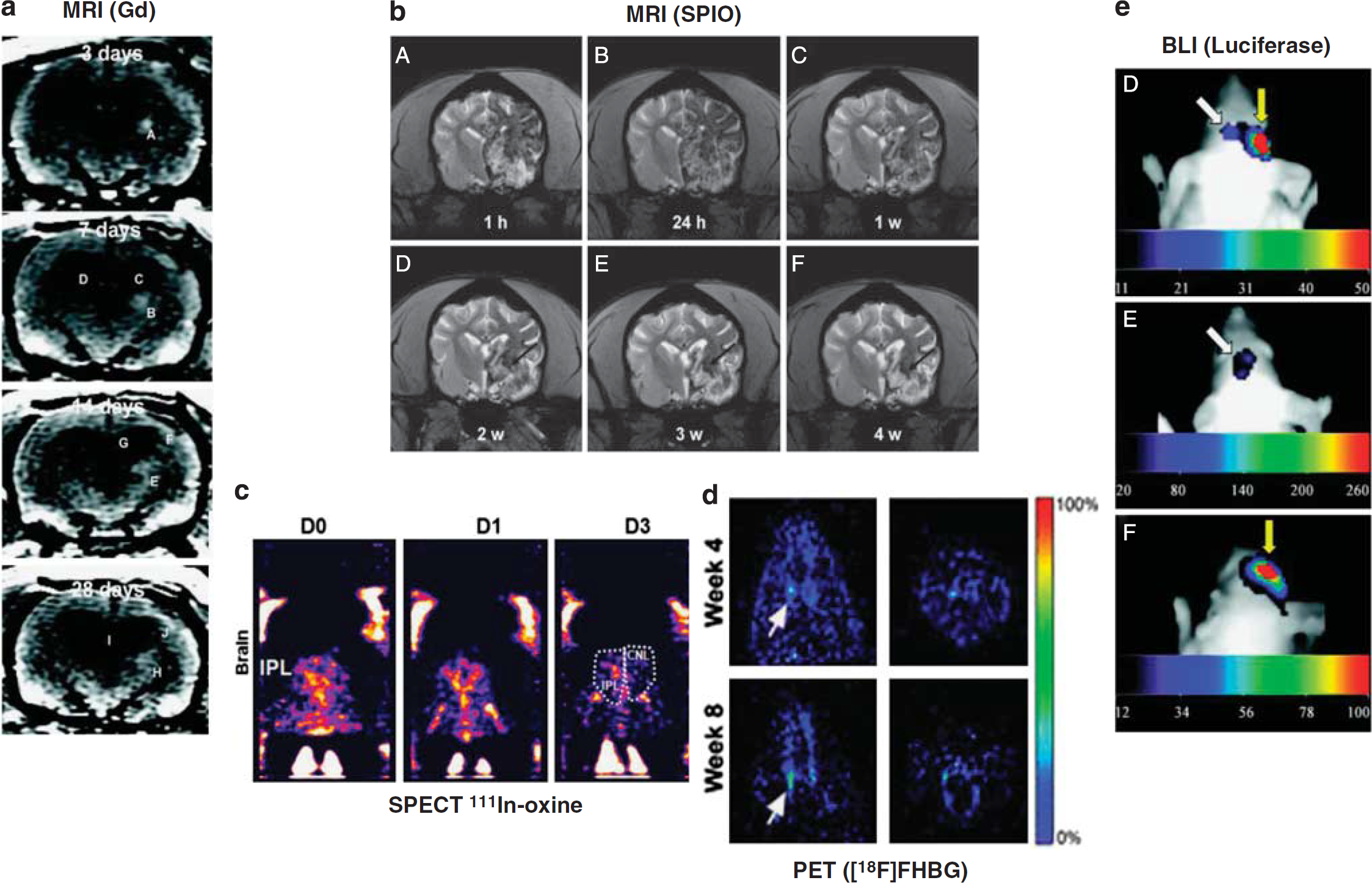
Comparison of imaging techniques for transplanted therapeutic stem cells following preclinical middle cerebral artery occlusion. (
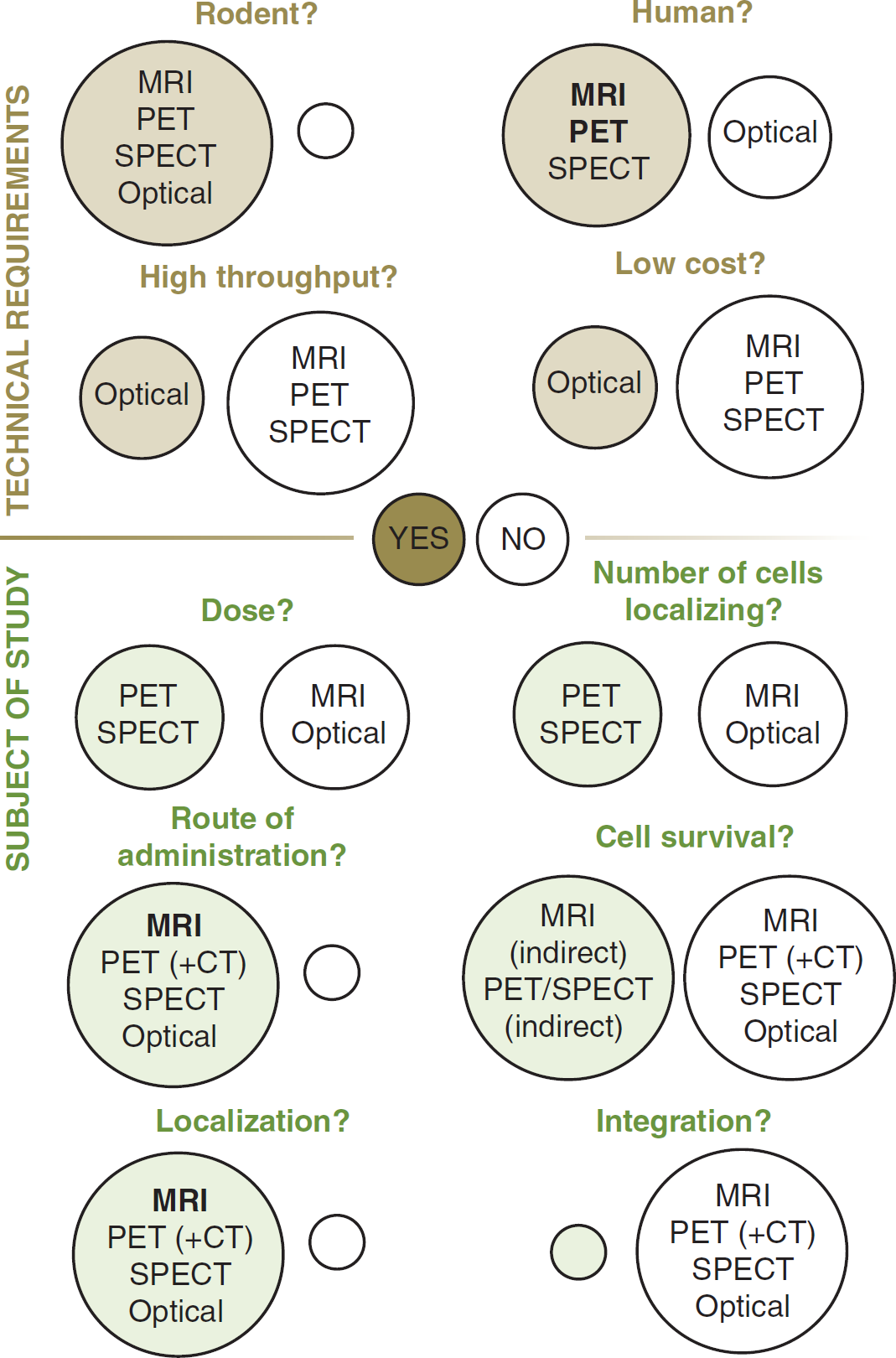
‘At-a-glance’ guide to imaging modality selection. Brown/green circles = ‘yes’ (i.e., this modality is a viable option), white circles = ‘no’ . CT, computed tomography; MRI, magnetic resonance imaging; PET, positron emission tomography; SPECT, single photo emission computed tomography.
The majority of modalities currently fall short of being able to record true integration of transplanted cells into existing networks, and understanding this thoroughly—what cells differentiate into (if anything) and what they release—will be of great benefit. The resolution required for this is not inconceivable: while it has yet to integrate stem cell imaging, functional MRI offers the opportunity to observe changes in brain connectivity (structural and functional modifications) in astonishing detail after stroke.109,110 In addition, the use of microoptical probes with in vivo multiphoton microscopy has now enabled the technique to be used to observe the processes of individual cells. 111
Monitoring stem cell migration with high resolution will be immensely useful in refining cell therapies. So little is currently known about cells posttransplantation; whether cells end up in the brain may ultimately be of little significance to their ability to improve outcome in stroke (although their being dispersed in unknown regions of the recipient would certainly complicate imaging due to, for example, positioning of the coil in MRI). Indeed, while many studies show stem cell homing to the brain after stroke,19,112 it has been shown that transplanted cells still improve recovery in rats treated with bone marrow stem cells after middle cerebral artery occlusion, despite the majority of these cells ending up in peripheral organs (including the lungs, spleen, and liver). 113 Furthermore, where one route of administration is preferable to another for stem cells from a particular source, imaging will—and does—help identify this. 114 Wherever therapeutic cells localize, tracking them in vivo will improve our knowledge of how these cells are of benefit. Understanding direct or indirect effects of these cells, whether they differentiate in the brain, resolves inflammation or releases growth factors; whether beneficial cells must migrate to an infarct or are able to act remotely is crucial in the refinement of a highly promising stroke therapy, and imaging promises to have an important role in this.
DISCLOSURE/CONFLICT OF INTEREST
The authors declare no conflict of interest.