
Abstract
Vascular dementia is the second most common type of dementia after Alzheimer’s disease (AD). Subcortical ischemic vascular disease refers to a form of vascular cognitive impairment characterized by the presence of diffuse white matter hyperintensities (WMHs) and multiple lacunar infarcts. These neuroimaging findings are mainly caused by cerebral small-vessel disease (cSVD) and relate to aging and cognitive impairment, but they can also be silent and highly prevalent in otherwise healthy individuals. We aimed to review studies on blood and cerebrospinal fluid (CSF) markers related to the presence of WMHs and lacunar infarcts that have been conducted in the past in large population-based studies and in high-risk selected patients (such as those with vascular risk factors, vascular cognitive impairment, or AD). Relevant associations with the presence and progression of cSVD have been described in the blood for markers related to inflammatory processes, endothelial damage and coagulation/fibrinolysis processes, etc. Also, different combinations of CSF markers might help to differentiate between etiologic types of dementia. In the future, to translate these findings into clinical practice and use biomarkers to early diagnosis and monitoring vascular cognitive impairment would require the replication of candidate markers in large-scale, multicenter, and prospectively designed studies.
Keywords
Introduction
Subcortical Ischemic Vascular Disease
Vascular cognitive impairment comprise a wide spectrum of cognitive dysfunctions that range from subtle or even clinically undetected (silent or covert) changes to the presence of an established dementia. Subcortical ischemic vascular disease (SIVD) is a term that encompasses a subtype of vascular cognitive impairment characterized by the presence of extensive white matter hyperintensities (WMHs) and multiple lacunar infarcts in brain imaging. 1 Although these brain lesions might be related to several etiologies, they are predominantly caused by cerebral small-vessel disease (cSVD). 2
Apart from lacunar infarcts and WMHs, brain atrophy and the presence of visible Virchow-Robin spaces (VRSs) are other common radiologic features of cSVD. 3 Although their relationship to vascular cognitive impairment is not as well established as it is for lacunar infarctions or WMHs, they will be probably considered among that spectrum in the coming years. Finally, hemorrhagic manifestations of cSVD such as cerebral microbleeds or superficial siderosis are out of the focus of this review.
Subcortical ischemic vascular disease is a progressive condition that evolves from normal cognitive status to established dementia, and its clinical and imaging characteristics partially overlap with other dementias. Therefore, SIVD biomarkers should provide a tool for an early detection, prediction of clinical course, differentiation from other dementias, and even to monitor response to specific treatments. 4
Research on biomarkers in the past has been mainly focused to relate candidate markers to specific neuroimaging cSVD features (mainly lacunar infarcts and WMHs) in several population-based studies or in selected, high-risk participants, such as those with vascular risk factors.2,5,6 Other studies were designed to compare candidate biomarkers among different types of vascular cognitive impairment groups (i.e., SIVD versus mixed dementia) or even to show differences from Alzheimer’s disease (AD) participants at different stages (mild cognitive impairment (MCI), mild to moderate dementia, etc.) or from healthy subjects. The majority of studies were conducted on blood proteins, although here we will review human studies on both blood and cerebrospinal fluid (CSF) biologic markers (not only proteins but also mRNA, genes, peptides, protein fragments, and lipids). Finally, both cross-sectional and longitudinal associations between biomarkers and imaging cSVD markers will be described, since in the past few years, information on accumulation of WMHs and incident lacunar infarcts in serial magnetic resonance imaging (MRI) examinations have become available.
Imaging Features of Cerebral Small-Vessel Disease and Subcortical Ischemic Vascular Disease
Silent brain infarcts (SBIs) are small brain ischemic lesions, which occur without a corresponding stroke-like event. They can be found in 8% to 28% of healthy subjects and their prevalence increase with age and hypertension. The great majority of SBI are indeed lacunar infarcts, since >90% of them are small infarcts found in the subcortical white matter, basal ganglia, thalamus, and infratentorial region, and usually they are caused by cSVD.7,8 Although many variations have been reported in the past regarding their diagnostic criteria concerning aspects such as size, CSF signal characteristics, or the presence of peripheral gliosis or degree of cavitation, they are usually defined in MRI as lesions thought to be of vascular origin, with CSF-like intensity signal in all pulse sequences, and with a maximum diameter comprised between 3 and 20 mm. 9
White matter lesions appear at MRI as focal or confluent, hyperintense lesions on brain T2-weighted sequences that are located in the deep subcortical white matter or in periventricular areas. 10 These WMHs also increase steadily with age and are found more often in subjects with vascular risk factors, such as hypertension or diabetes.11,12 In these conditions, arteriolosclerosis (vessel wall thickening and luminal narrowing) leads to restriction of cerebral blood flow and intermittent lack of oxygen supply, which triggers a series of events such as neuroinflammation and blood–brain barrier disruption.13,14 It has been recently shown that newly appearing focal WMHs display the signature features of acute ischemic stroke on brain MRI (restricted water diffusion on diffusion-weighted images), although with time, the characteristics of these lesions evolve and appear similar to those of areas with preexisting WMHs. 15
Visible VRSs are described as dilated spaces with accumulation of interstitial fluid, which surrounds small, deep, perforating arterioles as they go through deep gray and white matter. They are visible on T2- and T1-weighted MRI sequences and share signal characteristics with CSF. Virchow-Robin spaces have been described as a constant feature in pathologic studies of cSVD. 16 Virchow-Robin spaces are also present in general populations and their prevalence increases with age, hypertension, and with the presence of other markers of cSVD. 17
Brain atrophy is characterized by the loss of neuronal cells and brain parenchyma, with resulting increase in the volume of ventricles and sulci. Increased brain atrophy has been described in elderly healthy people, but an abnormal grade has been used as an outcome measure in AD, cSVD studies, and other neurologic disorders.18,19 Representative examples of these common MRI features are shown in Figure 1.
Representative examples of imaging markers of cerebral small-vessel disease. From left to right: brain infarct affecting caudate nuclei is shown by a white arrow (fluid attenuated inversion recovery (FLAIR) magnetic resonance imaging (MRI)), extensive white matter changes (FLAIR MRI), and enlarged perivascular spaces involving basal ganglia shown by white arrows and moderate tempooccipital brain atrophy (T2 MRI); 1.5 Tesla MR (Signa HDx 1.5, General Electric, Waukesha, WI, USA).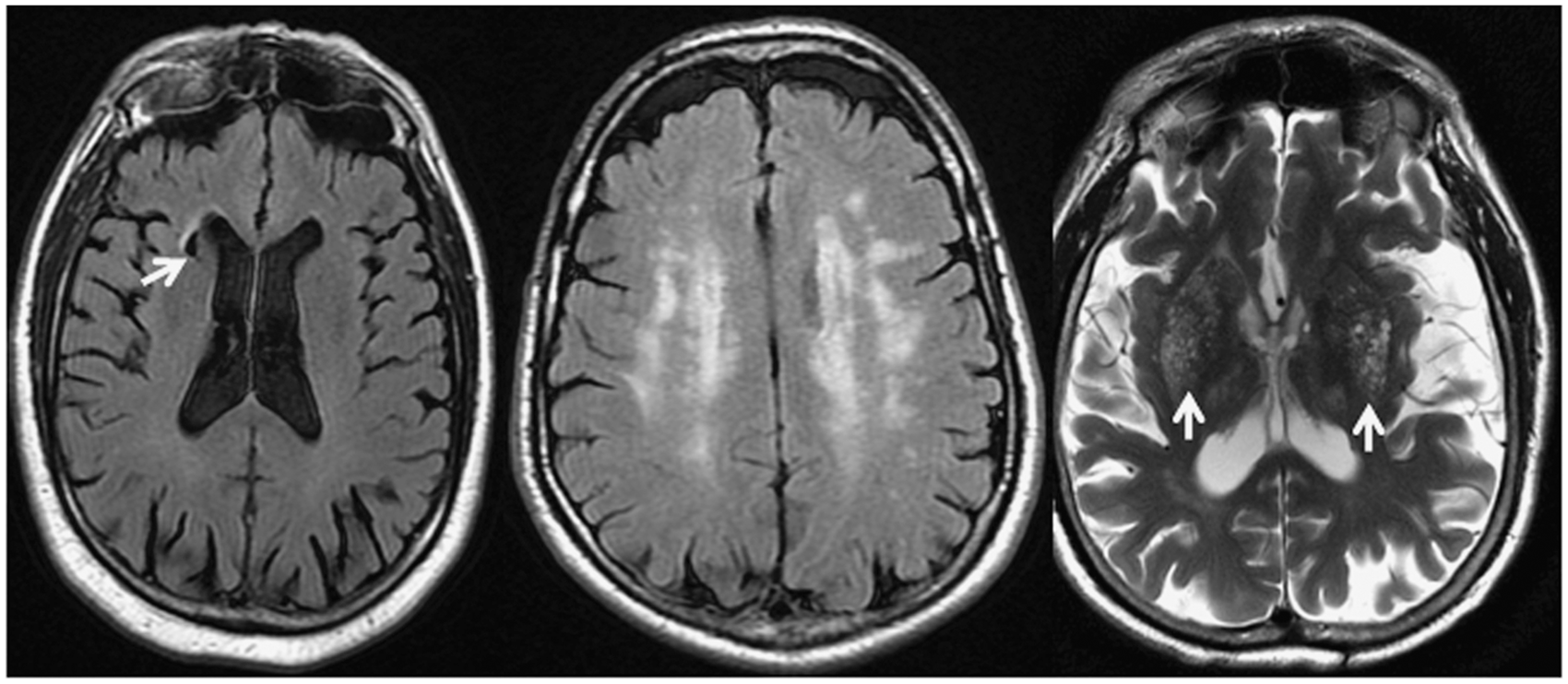
Blood Biomarkers Associated with Imaging Features of Cerebral Small-Vessel Disease and Subcortical Ischemic Vascular Disease
A biomarker is ‘a characteristic that is objectively measured and evaluated as an indicator of normal biologic processes, pathogenic processes or pharmacologic responses to intervention’ according to the National Institutes of Health Definitions Working Group. 20 Several families of candidate biomarkers have been studied so far in relation to SIVD. We will focus in this review on biomarkers related to inflammation, endothelial dysfunction, hemostasis, and components of the renin–angiotensin–aldosterone system, among others.
Inflammatory biomarkers
Inflammation has been recognized as a key component in cerebrovascular and neurodegenerative diseases.21,22 Inflammation might contribute to SIVD through several processes such as atherogenesis, low-grade inflammation, and platelet aggregation, which are mediated by cytokines, leukocyte adhesion molecules, chemokines, growth factors, and also lipids. 21
C-reactive protein (CRP) and interleukin-6 (IL-6) are the most commonly studied inflammatory biomarkers in this field. C-reactive protein, an acute-phase reactant synthesized in the liver in response to IL-6, has been widely used as a vascular inflammatory marker. It has been associated with the pathogenesis of atherosclerosis, development of diabetes, hypertension, metabolic syndrome, and with the appearance of cardiovascular events. 23 – 26 Interleukin-6 is secreted by T cells and macrophages to stimulate immune response and by smooth muscle cells of blood vessels as a proinflammatory cytokine. It is associated with myocardial infarction, stroke, cardiovascular death, and peripheral arterial disease.26,27
Several studies focused on the analysis of inflammatory markers in the context of SBI in general populations. High levels of IL-6 and CRP were found associated with the risk of SBIs in one study, and confirmed by other, in which it was shown that the combination of Acrolein, CRP, and IL-6 was associated with the risk of both SBIs and WMHs. 28 – 30
However, some studies have also reported negative associations. C-reactive protein and IL-6 levels were analyzed in a large study and only a cross-sectional association of IL-6 with WMHs was found. Neither SBIs incidence nor WMH progression at follow-up were associated with IL-6 or CRP, although small rates of progression might have limited statistical power to show associations. 31
On selected populations at higher risk for SIVD, such as those with vascular risk factors (diabetes and hypertension) or other clinical conditions such as kidney failure, IL-6 and CRP were similarly associated with SBIs as in population-based studies. 32 – 34 Given the close relationship between SBIs and the risk of future clinical stroke and cognitive decline, these inflammatory markers might prove potentially useful predictors of outcome in specific populations.
Regarding WMHs, increased plasma levels of CRP have been linked to their presence and progression in some studies, while in others the association was not found.10,31,35– 40
Other typical features of cSVD and SIVD, such as the presence of brain atrophy and VRS have also been related with inflammatory biomarkers. The association between CRP, IL-6, and fibrinogen with visible VRSs and WMHs was examined in the Lothian Birth Cohort 1936. A weak association was found between inflammatory markers and visible VRS, which was not present between inflammatory markers and WMHs. 41 Other authors assessed the association between plasmatic neopterin (a molecule expressed by activated monocytes) and VRSs. Neopterin levels were found linearly associated with the amount of VRSs at the basal ganglia. 40 Both studies suggest that inflammation might play a role in the enlargement of perivascular spaces, as it happens with other diseases such as multiple sclerosis, in which the inflammatory activity coincides with the dilation of perivascular spaces.
Regarding brain atrophy, IL-6 has been associated with severe cortical atrophy, and decreased gray matter or hippocampal volumes in cross-sectional studies of candidate biomarkers,31,42 and also in studies using panels of multiple biomarkers.43,44
Finally, it needs to be mentioned that interactions between inflammatory biomarkers and age, gender, and ethnicity might exist. As an example, Japanese populations were suggested to have lower CRP levels and weaker associations with WMHs than those seen in western populations. 45 Likewise, gender differences had also been proposed, with higher prevalence and greater progression of WMHs in women than in men, and a stronger association between IL-6 and WMHs in women than in men.39,46,47
Circulating blood biomarkers associated with silent brain infarctions and WMHs ordered by relevance according to number of patients recruited in the studies
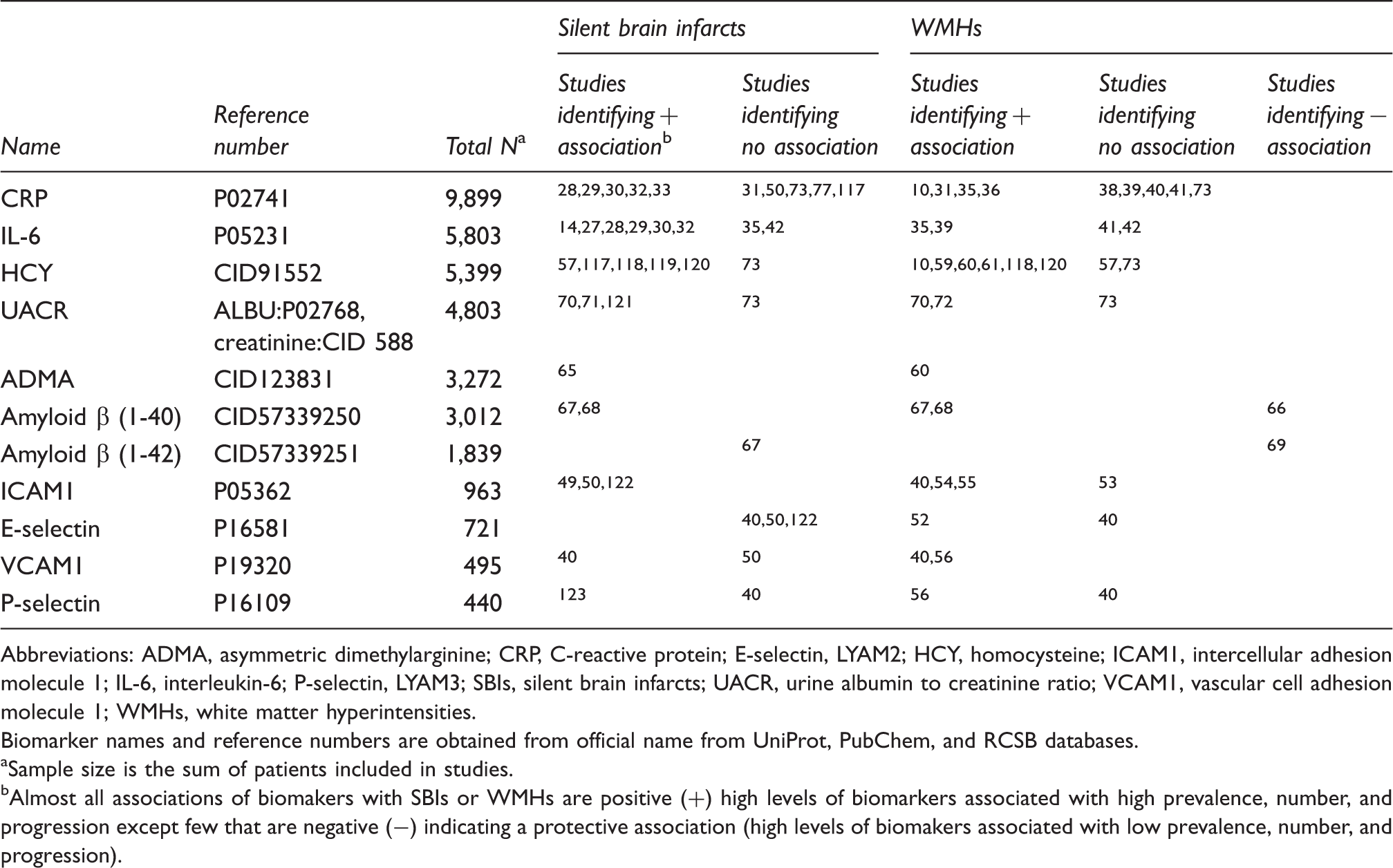
Abbreviations: ADMA, asymmetric dimethylarginine; CRP, C-reactive protein; E-selectin, LYAM2; HCY, homocysteine; ICAM1, intercellular adhesion molecule 1; IL-6, interleukin-6; P-selectin, LYAM3; SBIs, silent brain infarcts; UACR, urine albumin to creatinine ratio; VCAM1, vascular cell adhesion molecule 1; WMHs, white matter hyperintensities.
Biomarker names and reference numbers are obtained from official name from UniProt, PubChem, and RCSB databases.
aSample size is the sum of patients included in studies.
bAlmost all associations of biomakers with SBIs or WMHs are positive (+) high levels of biomarkers associated with high prevalence, number, and progression except few that are negative (−) indicating a protective association (high levels of biomakers associated with low prevalence, number, and progression).
Endothelial dysfunction
The healthy endothelium plays a pivotal role in regulating brain vascular homeostasis and many factors may alter this and converge to generate endothelial dysfunction. Endothelial dysfunction appears as a result of persistent ischemia/reperfusion and inflammation generating oxidative stress from unbalanced free radical formation that leads to peroxynitrite formation, lipid peroxidation, protein modification, matrix metalloproteinase (MMP) activation, and DNA damage. All these combined with the previously covered proinflammatory stimuli (chemokines, cytokines, and adhesion molecules that interact with leukocytes and platelets), and enhanced by the concurrence of vascular risk factors promotes that the endothelium becomes dysfunctional, blood–brain barrier permeability is disrupted allowing infiltration of the brain parenchyma with circulating toxic molecules and prothrombotic changes may occur. 48
A panel of 24 analytes including cytokines, chemokines, growth factors, adhesion molecules, cell surface receptors, and inductors of apoptosis was tested in a small group of subjects (
Besides, endothelial damage markers have also been involved not only in the presence but also in the progression of SBIs over time, and in fact they might be predictive in diabetic populations.50,51
White matter hyperintensities have also been related to higher levels of several endothelial dysfunction markers like soluble E-selectin, soluble intercellular adhesion molecule 1, soluble P-selectin, and soluble vascular cell adhesion molecule 1 in cross-sectional studies. 52 – 56 Moreover, both baseline WMH load and intercellular adhesion molecule 1 were independent predictors of WMH progression after adjustment by potential confounders in a longitudinal assessment of the community-based Austrian Stroke Prevention study. 55
Homocysteine (HCY) is a product of the metabolism of dietary methionine. The liver is the major site of HCY metabolism, with kidney also making a significant contribution. Elevated levels of HCY can result from a variety of causes although folate deficiency appears to be a major determinant of fasting HCY levels in otherwise healthy individuals as well as in patients with kidney failure.
The mechanisms underlying the association between HCY with brain vascular disease are not completely understood but may involve both vascular and neuronal pathways.
Homocysteine levels were measured within a middle-aged cohort from the Framingham Offspring study, a strong association was found between higher plasma HCY levels and lower total cerebral brain volume and with an increased risk of SBI, whereas no relation was found with WMH volumes. 57 Similar associations were obtained in the Rotterdam Scan study, where a continuous and graded association of HCY was found with SBIs, although HCY levels were also higher in those with more WMHs. 2
Both types of lesions were combined in a study, to define a diffuse cSVD subtype (presence of both lacunar infarction and WMHs) and a focal subtype (isolated lacunar infarction). Homocysteine was described as a stronger predictor for the diffuse than for the focal subtype. Also, other markers of endothelial dysfunction, such as intercellular adhesion molecule 1 and thrombomodulin, could improve the prediction of these lesions together with HCY. 58
More recently, HCY levels appeared also associated with progression of WMHs in a cohort with symptomatic atherosclerotic disease from the SMART-MR study (Second Manifestations of Arterial Disease-Magnetic Resonance study). 59
Homocysteine positive association with the presence of WMHs is also well documented with symptomatic cSVD patients, such as those having a transient ischemic attack (TIA) or subcortical stroke, where it is not only associated with MRI lesions but also with cognitive status.60,61 Since cognitive impairment has been associated with hyperhomocysteinemia, several studies have investigated whether vitamin supplementation to reduce HCY levels would also delay cognitive decline. Results obtained to date either in healthy elderly individuals or in those with prior stroke or TIA do not confirm the efficacy of this treatment to prevent cognitive decline. 62 – 64
Asymmetric dimethylarginine is an endogenous inhibitor of endothelial nitric oxide synthase (eNOS). Abnormally high asymmetric dimethylarginine levels reflect the presence of endothelial dysfunction and they are also related to hyperhomocysteinemia. Higher levels of asymmetric dimethylarginine were described in 47 symptomatic cSVD patients as compared with healthy controls, which were also correlated with WMH severity, but not with the number of lacunar infarcts. 60 Meanwhile, in stroke-free subjects from the Framingham Offspring cohort, baseline plasma asymmetric dimethylarginine levels were predictive of the risk of SBIs (assessed 4 years later) but not for large WMHs. 65
Amyloid peptides (Aβ1-40 and Aβ1-42 species) are generated by amyloid precursor protein cleavage. They are able to aggregate into fibrillar deposits both in brain tissue (plaques) and in vessel walls. Several studies have suggested a toxic effect on the vessel wall of the Aβ1-40.
An association of Aβ1-40 but not Aβ1-42 with WMHs and lacunar infarcts was described in a heterogeneous population composed of AD, MCI, and cerebral amyloid angiopathy patients. 66 Likewise, others described Aβ1-40 levels strongly associated with diffuse cSVD (defined as the presence of multiple lacunes and WMHs) in a cohort of acute lacunar stroke. 67
Besides, studies of amyloid β peptides on healthy individuals have provided mixed results. Authors from the Rotterdam Scan study reported a strong association between both elevated peptides and SBIs or extensive WMHs in apolipoprotein E4 carriers. 68 On the contrary, no cross-sectional associations were found with WMHs or lacunes in the Three-City Dijon study but instead, low levels of both species were associated with WMH progression after 4 years of follow-up. 69 Further research in larger populations is needed to determine how Aβ deposition in the brain affects plasma and CSF levels of peptides. High circulating levels could mean a damaged neurovascular unit as a consequence of ischemic microvascular disease and WMHs. However, low circulating levels would reflect deposition on vessel wall, as it has been described in cerebral amyloid angiopathy, and further cerebrovascular damage.
Microalbuminuria, assessed by means of urinary albumin to creatinine ratio might reflect early kidney damage or systemic endothelial dysfunction.
Microalbuminuria was found as an independent risk factor for SBI and moderate WMHs in a community-based study on elderly Japanese participants. 70 Similar findings were described for SBIs, and for WMHs or brain atrophy in hypertensive populations.71,72 All of them support the idea of microalbuminuria as an early marker of preclinical brain damage in essential hypertension, and suggest its potential usefulness to identify high-risk patients, which might be candidates for preventive approaches.
Finally, microalbuminuria was also found to be a risk factor for decreased total cerebral brain volume in the Framingham Offspring study. 73
A summary of the most relevant biomarkers associated with endothelial function is shown in Table 1.
Hemostatic abnormalities
Molecules involved in the coagulation and fibrinolytic pathways have been largely studied in symptomatic cardiovascular and cerebrovascular disease. Tissue factor, coagulation factor VII, or thrombomodulin are among the most investigated players, and it is well known that a prothrombotic status is associated with cardiovascular risk. 74 However, less is known about the role of hemostatic biomarkers in SIVD with most of the studies yielding discordant evidences (Supplementary Table 1).
Thrombomodulin has been associated with the presence and number of lacunar infarctions and also with WMHs, especially in the presence of microalbuminuria.53,70,75 Plasminogen activator inhibitor-1 is one of the main inhibitors of fibrinolysis, acting on tissue plasminogen activator and urokinase. Results on the relationship between plasminogen activator inhibitor-1 levels and SBI or WMHs are conflicting and the same could be argued for fibrinogen or D-dimer (a marker of fibrinolytic turnover).
A small study described that the levels of thrombin–antithrombin complex and cross-linked D-dimer were higher in a group of patients with subcortical vascular dementia and severe leukoaraiosis (Binswanger's disease) at deteriorating states as compared with patients with other neurologic diseases. 76
Finally, von Willebrand factor, a glycoprotein expressed by endothelial cells after tissue damage, showed more consistent results. High plasma von Willebrand factor levels were associated with the presence, and number of SBI, with periventricular but not deep WMHs, and with WMH burden. 77 – 80
Renin–angiotensin–aldosterone system
The components of the renin–angiotensin–aldosterone system have been studied as candidate markers in cSVD because of their role in hypertension, endothelial function, and the regulation of smooth muscle cell proliferation and tone. 81 Specifically, results with angiotensinogen, angiotensin, angiotensin converting enzyme (ACE), and angiotensin II receptor type 1 have been reported. Although most of the studies refer to single nucleotide polymorphisms, few have evaluated protein levels (or protein activity) involved in this pathway (Supplementary Table 1).
Angiotensin converting enzyme levels were investigated in a cross-sectional study of 510 subjects, the Genetique de l’Infarctus Cerebral study. These authors found an association between plasma ACE levels and the presence of multiple lacunar infarctions, but not with WMHs. 82 Later on, increased ACE levels have been found in those subjects with greater progression of deep WMH volume but with less progression of cortical atrophy, suggesting a dual role (beneficial/detrimental) of ACE in the brain. 83
Extracellular matrix proteins
Matrix metalloproteinases are a family of zinc- and calcium-dependent endopeptidases secreted as proenzymes by several cell types as neurons and glial cells. 84 Matrix metalloproteinases act cleaving almost all matrix proteins, and this process is inhibited by tissue inhibitor of metalloproteinases. Besides matrix proteins, they can process cytokines and neuronal structural proteins such as myelin basic protein or tight junction proteins. A role for this family of proteases has been suggested in postmortem studies of vascular dementia, including subjects with Binswanger’s disease. 85 Matrix metalloproteinase-9 and tissue inhibitor of metalloproteinase-1 plasma levels were found to be associated with WMHs and brain atrophy in a study within 583 participants of the Framingham Offspring study. 86
Lipid metabolism
The diagnostic value of total cholesterol, high-density lipoprotein cholesterol, low-density lipoprotein cholesterol, and triglycerides is not well established for cSVD. In the Leukoaraiosis And DISability (LADIS) study, progression over time of cSVD markers were analyzed and the authors described protective associations of low-density lipoprotein and triglycerides with lacunes and WMH progression, respectively. 87
In contrast, in a study of two independent cohorts, comprising a total of 2,608 elderly participants, several lipid fractions (triglycerides, low-density lipoprotein, and high-density lipoprotein) were analyzed, and it was shown that increasing triglyceride levels were associated with increasing frequency and severity of lacunes and WMH volume. These findings were similar considering those subjects taking or not taking lipid-lowering drugs. 88
However, other authors tested a similar lipid profile and found no association between lipids and WMH volumes or SBIs for their whole population. Nevertheless some associations emerged between lipids and WMHs in APOE4 carriers or in those presenting worsening total cholesterol or high-density lipoprotein cholesterol over time. 89
Lipoprotein-associated phospholipase A2 is an hydrolase enzyme produced by inflammatory cells that circulates mainly to bound low-density lipoproteins and less frequently with high-density lipoproteins. 90 Its use was approved by the FDA (Food and Drug Administration) for cardiovascular risk prediction. Its proinflammatory activity is supported by a number of epidemiologic studies suggesting that plasmatic lipoprotein-associated phospholipase A2 is an independent predictor of cardiovascular events. Our group analyzed lipoprotein-associated phospholipase A2 activity in a population of middle aged to elderly hypertensives and an association between this enzyme and SBIs was found in women, but not in men. 6 Lipoprotein-associated phospholipase A2 mass and myeloperoxidase were found to be associated with WMH volumes, but not with brain infarcts in another study in which no interactions with gender were noticed. 38
Lipoprotein-associated phospholipase A2 mass and activity have also been described as a risk factor for dementia in the Cardiovascular Health Study. Regarding subtypes, lipoprotein-associated phospholipase A2 mass has been mainly related to AD subtype, while the enzyme activity was a risk factor for vascular dementia. 91
A summary of lipid metabolism molecules associated with SBIs and WMHs are shown in Supplementary Table 1.
Other blood biomarkers
In this section, we will consider other markers from which evidence is less strong or cannot be included in any of the families already presented here (Supplementary Table 1).
Highly sensitive cardiac troponin T and B-type natriuretic peptide are considered biomarkers of subclinical cardiac injury. Within the Atherosclerosis Risk In Communities (ARIC) study, both were analyzed and found to be related to the presence of SBIs and WMHs, and also with their incidence and progression, respectively. 92 However, in the Framingham Offspring cohort, investigators failed to find any association for B-type natriuretic peptide and SBIs or WMHs (taken B-type natriuretic peptide either as a part of a panel composed by eight different biomarkers or alone). Interestingly though, the full panel of biomarkers (which comprised molecules of inflammation, hemostasis, neurohormonal activity, and endothelial function) was associated with total cerebral brain volume. 73
Increased levels of uric acid are associated with elevated serum triglyceride, cholesterol, and blood glucose levels and with metabolic syndrome. Some reports have shown beneficial effects in acute stroke animal models and there is a clinical trial on neuroprotective effects of uric acid on stroke patients. Nevertheless, the relationship between uric acid and subclinical brain vascular disease remains unclear. Although one study found high levels of uric acid independently related to the presence of SBIs only in women, others found uric acid as a risk factor for WMHs only in men.93,94
Oxidative processes on lipids and carbohydrates lead to the formation of reactive carbonyl species that transforms proteins on advanced glycation end products. The activation of the receptor of advanced glycation end product induces proinflammatory cytokines and free radicals that also activate the receptor, thereby enhancing endothelial damage. Soluble receptor of advanced glycation end product levels were found to differ according to gender in the Northern Manhattan Study and were also inversely related with the risk of SBIs, particularly in Hispanics and non-Hispanic blacks. 95
Cerebrospinal Fluid Biomarkers and Subcortical Ischemic Vascular Disease
The release of cellular products and molecules into the extracellular space because of degeneration or acute damage should be reflected in the biochemical composition of the CSF. However, in contrast to blood biomarkers, few studies have been conducted to assess biomarkers of SIVD or their related MRI markers using CSF samples.
It has been described that levels of sulfatides, increased levels of myelin basic protein and neurofilament light polypeptide might be associated with some features of cSVD, in particular with WMHs. 96 – 99
Neurofilaments are part of the axonal structure and play a role on transport within the neuron. Neurofilament light polypeptide is the most abundant of the three filament proteins (heavy, medium, and light) that compose the neurofilaments. Neurofilament light polypeptide increase in CSF might be a consequence of axonal damage. Neurofilament light polypeptide was found to be increased in dementia-free patients in relation to increasing WMHs in a cross-sectional analysis from the LADIS study, in AD and in SIVD subjects, and also in MCI patients that later on developed subcortical vascular dementia.15,96,100 The later study showed that CSF levels of Aβ1-42, total Tau (t-Tau), and Phospho-Tau (P-Tau) distinguished between those MCI patients evolving to AD as compared with those who progress to SIVD.
Blood–brain barrier dysfunction as indicated by an increased albumin CSF/serum ratio has been related to WMHs in previous studies on patients with dementia. 101 Furthermore, MMP-2 and MMP-9 in CSF and plasma (in reference to CSF and plasma albumin) and MMP-3 activity were measured in a cohort of 60 patients with vascular cognitive impairment—no dementia. Matrix metalloproteinase-2 ratio was found to be significantly lowered in the whole group of vascular cognitive impairment subjects as compared with controls and also negatively correlated with the albumin ratio. Furthermore, the combination between MMP-2 index and MMP-3 activity was highly specific to differentiate SIVD from the control group. 102
Several combinations of CSF proteins might help to differentiate SIVD and AD from controls and from each other. Thus, markers reflecting AD pathologic assessment such as total Tau and Aβ1-42 separate AD from controls, while markers assessing white matter damage such as myelin basic protein and neurofilament light polypeptide discriminate SIVD from controls. Moreover, all of them together plus MMP-2, MMP-9, and tissue inhibitor of metalloproteinase-1 are able to distinguish between AD and SIVD with elevated sensitivity and specificity. 98
Likewise, another study performed in two independent cohorts determined a panel of 90 CSF proteins in several types of clinically established dementia (subcortical vascular dementia, AD, and mixed dementia) or at their prodromal stages (MCI), and compared them with healthy controls. On multivariate analysis, they found that heart-type fatty acid–binding protein and alpha-1 antitrypsin discriminated with 86% sensitivity and 86% specificity between those with mixed dementia and subcortical vascular dementia from controls. Also, these same diseases at their early stages (MCI) were also differentiated from controls with high accuracy by the combination of plasminogen activator inhibitor-1, regulated on activation normal T-cell expressed and secreted protein (RANTES), tissue inhibitor of metalloproteinase-1, and lipoprotein(a). 103 Interestingly also, some CSF proteins were altered in AD but not in subcortical vascular dementia, pointing to different pathophysiologic mechanisms.
Usefulness of cerebrospinal fluid biomarkers on discriminating dementia types
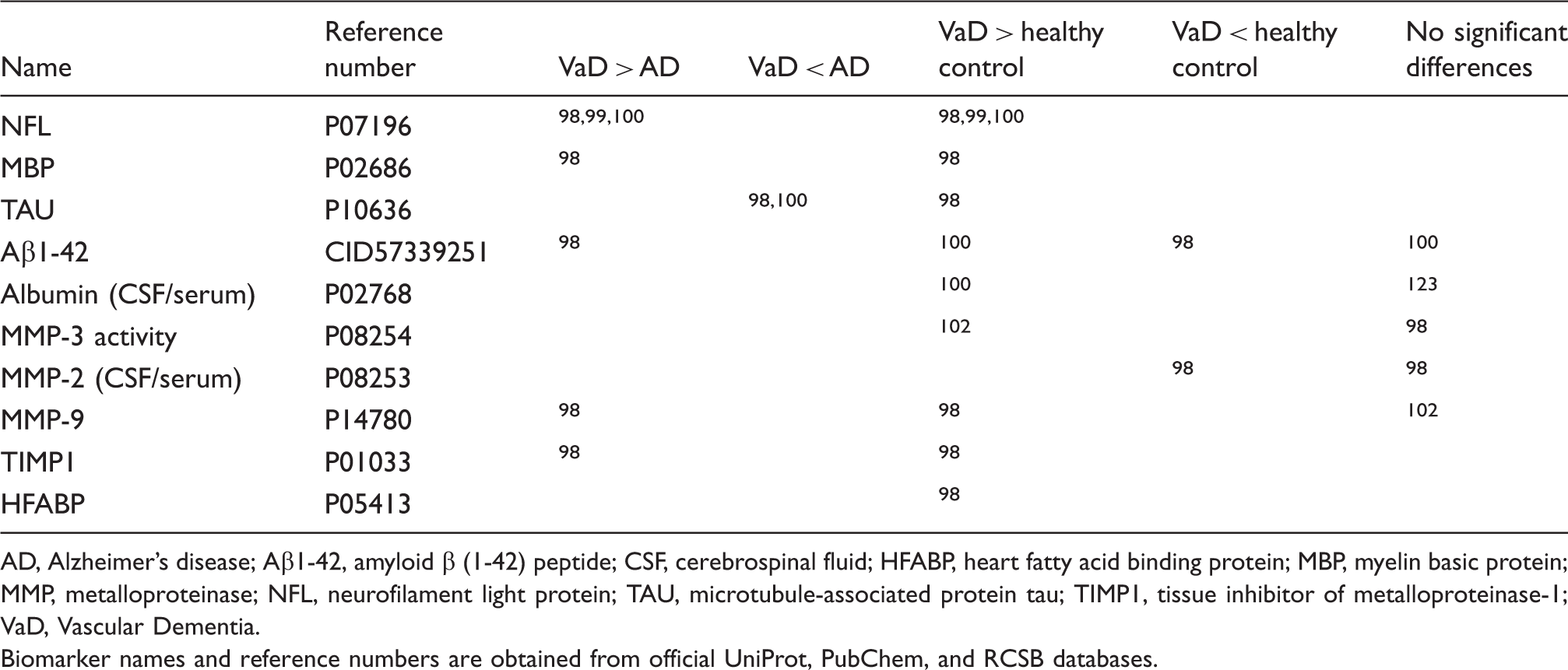
AD, Alzheimer’s disease; Aβ1-42, amyloid β (1-42) peptide; CSF, cerebrospinal fluid; HFABP, heart fatty acid binding protein; MBP, myelin basic protein; MMP, metalloproteinase; NFL, neurofilament light protein; TAU, microtubule-associated protein tau; TIMP1, tissue inhibitor of metalloproteinase-1; VaD, Vascular Dementia.
Biomarker names and reference numbers are obtained from official UniProt, PubChem, and RCSB databases.
Genetic Markers and Subcortical Ischemic Vascular Disease
Although cSVD includes several monogenic forms (cerebral autosomal dominant artheriopathy with silent infarcts and leukoencephalopathy (CADASIL), Fabry's disease, etc.), it is more often a sporadic disease related to aging and hypertension. 4 However, some pathologic traits of SIVD, such as WMHs are supposed to be inherited in a high percentage of cases (ranging from 55% to 80%). 37
Genetic variants associated with silent brain infarctions and WMHs
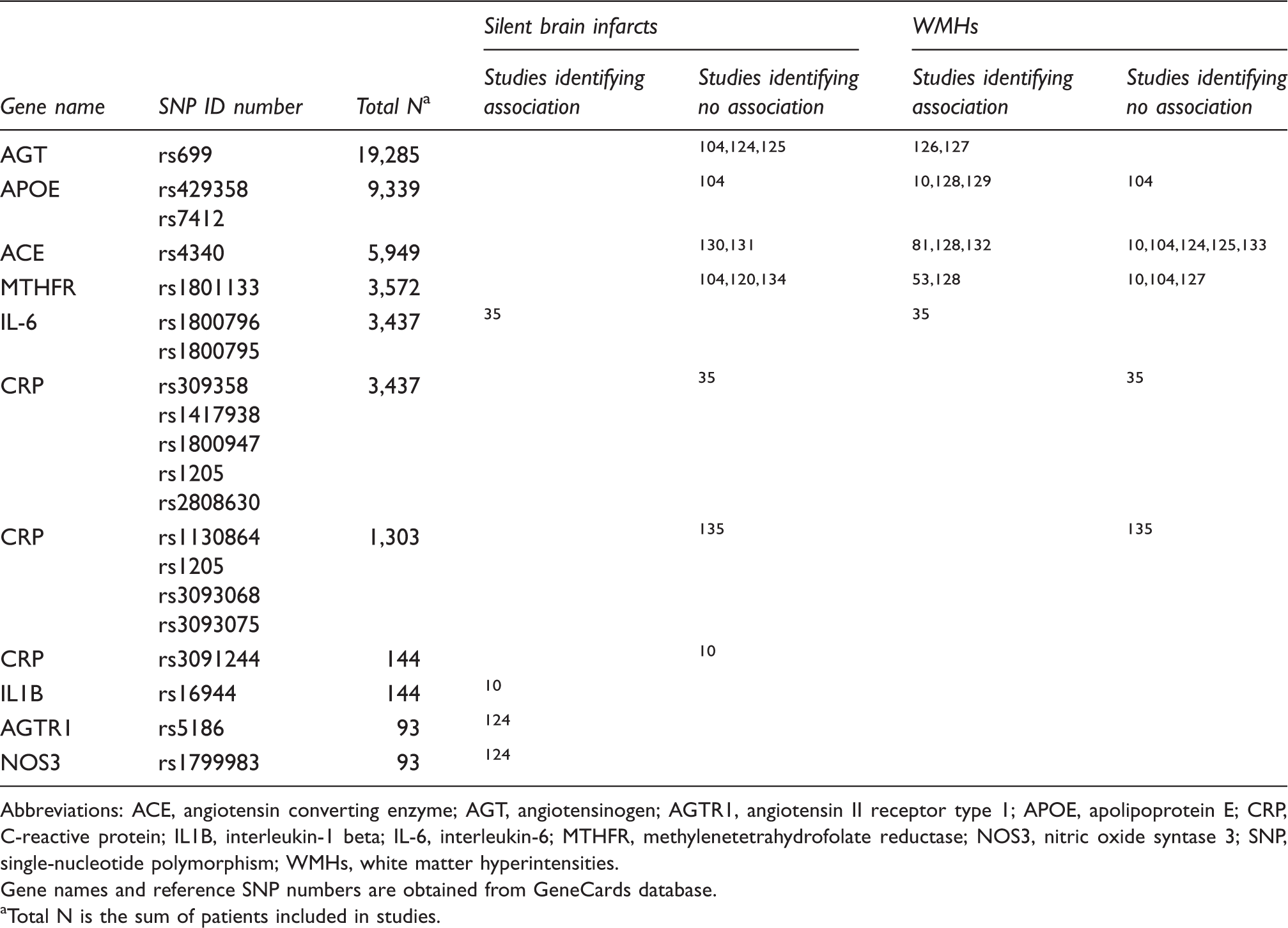
Abbreviations: ACE, angiotensin converting enzyme; AGT, angiotensinogen; AGTR1, angiotensin II receptor type 1; APOE, apolipoprotein E; CRP, C-reactive protein; IL1B, interleukin-1 beta; IL-6, interleukin-6; MTHFR, methylenetetrahydrofolate reductase; NOS3, nitric oxide syntase 3; SNP, single-nucleotide polymorphism; WMHs, white matter hyperintensities.
Gene names and reference SNP numbers are obtained from GeneCards database.
Total N is the sum of patients included in studies.
A meta-analysis of 46 studies, which included variants in 19 candidate genes involved in the pathogenesis of cSVD and including more than 2000 subjects found no convincing associations between APOE gene, ACE, methylenetetrahydrofolate reductase and angiotensinogen and WMHs. 104
Free genome-wide approaches have become available in the past few years. This approach enhances power to detect genetic associations in common diseases when combining results of different cohorts in meta-analysis. Any pathway, not only those that are suspected could be identified, but also uncovering novel genes involved in cSVD and SIVD.
Genome-wide association studies
Given the lack of consistent findings in candidate gene studies of cSVD, investigators from the Cohorts for Heart and Aging Research in Genomic Epidemiology (CHARGE) consortium performed a genome-wide association study and meta-analysis, to search for genetic variants associated with SBIs. No variants were found with statistical significance at genome-wide association study level (
Afterwards, results from a new genome-wide association study were published with WMH burden as outcome, in which one new locus was described in chromosome 17q25. This locus contained several genes such as WW domain–binding protein 2, tripartite motif-containing 65, tripartite motif-containing 47, mitochondrial ribosomal protein L38, Fas-binding factor 1, and acyl-coenzyme A oxidase 1, encoding proteins that were involved in apoptosis, innate immunity, cell cycle regulation, vesicular trafficking, and neuroprotection. 106 Later, authors from the Rotterdam Scan study replicated these associations within the 17q25 locus and more recently, the first replication for the same locus in a non-European population was published.107,108 Finally, this locus was related with WMHs in a cohort of subjects with acute ischemic stroke, although on the contrary to what should be expected regarding etiology, lacunar stroke was not associated. 109 For us it was also an unfortunate surprise that the large METASTROKE collaboration identified interesting candidate genes for cardioembolic (PITX2 and ZFHX3) and for large-vessel stroke (HDAC9) but no signal was found for small-vessel stroke. 110 Finally, linkage studies have identified several chromosomes with shared loci associated with WMH volumes and also with blood pressure parameters, suggesting pleiotropic genes might exist in these locations.111,112 New genetic technology including exome sequencing and epigenetics will probably be used in the coming years and might add new players to the field.
Genetic studies in disease progression
The majority of genetic studies have focused so far on cross-sectional associations and there is much less information on the relation of genetic variants and lesion progression. To our knowledge, only a recent study, described that both HCY levels and methylenetetrahydrofolate reductase C677T gene variation were associated with the progression of ventricular enlargement (i.e., subcortical atrophy) after a mean follow-up of 4 years. Interestingly, this progression was parallel to the decline on executive function. 83
RNA approaches
Circulating RNA was used to define profiles of differentially expressed genes to distinguish small deep infarct etiologies in a cohort of 184 ischemic stroke patients. Their results revealed several pathways alterated and related with inmune blood cells, that were different for lacunar and nonlacunar stroke patients. 113
MicroRNAs (miRNAs) are small noncoding RNAs that regulate mRNA expression by binding to untranslated regions. There are few miRNA but each can regulate hundreds of target genes, therefore they represent an important mechanism of gene regulation. Differential profiles of circulating miRNA for stroke subtypes, including small-vessel disease, were described in a preliminary report of a very small sample of young ischemic stroke patients, interestingly, they observed that some miRNAs remain stable expressed and in circulation even after several months from the onset of stroke and some are upregulated in small artery stroke as compared with large artery strokes (miR-130b, miR-29b, miR-301a, miR-339-5p, miR-532-5p, miR-634, and miR-886-5p). 114
More recently, a study focused on four well-known polymorphisms in miRNA sequences (miR-146a, -149, -196a2, and -499 alleles), described an association between some allele combinations and SBIs incidence, and an effect on HCY/folate levels. These had been previously associated with regulation of tumor necrosis factor-
Future Perspectives
Here we reviewed blood and CSF biomarkers that have been related to the appearance of characteristic MRI findings in cSVD, such as SBIs and WMHs. Although these lesions appear frequently on healthy elderly individuals, their presence and progression largely predispose to future cognitive impairment, and the presence of multiple lacunar infarcts and extensive WMHs are constant in SIVD.
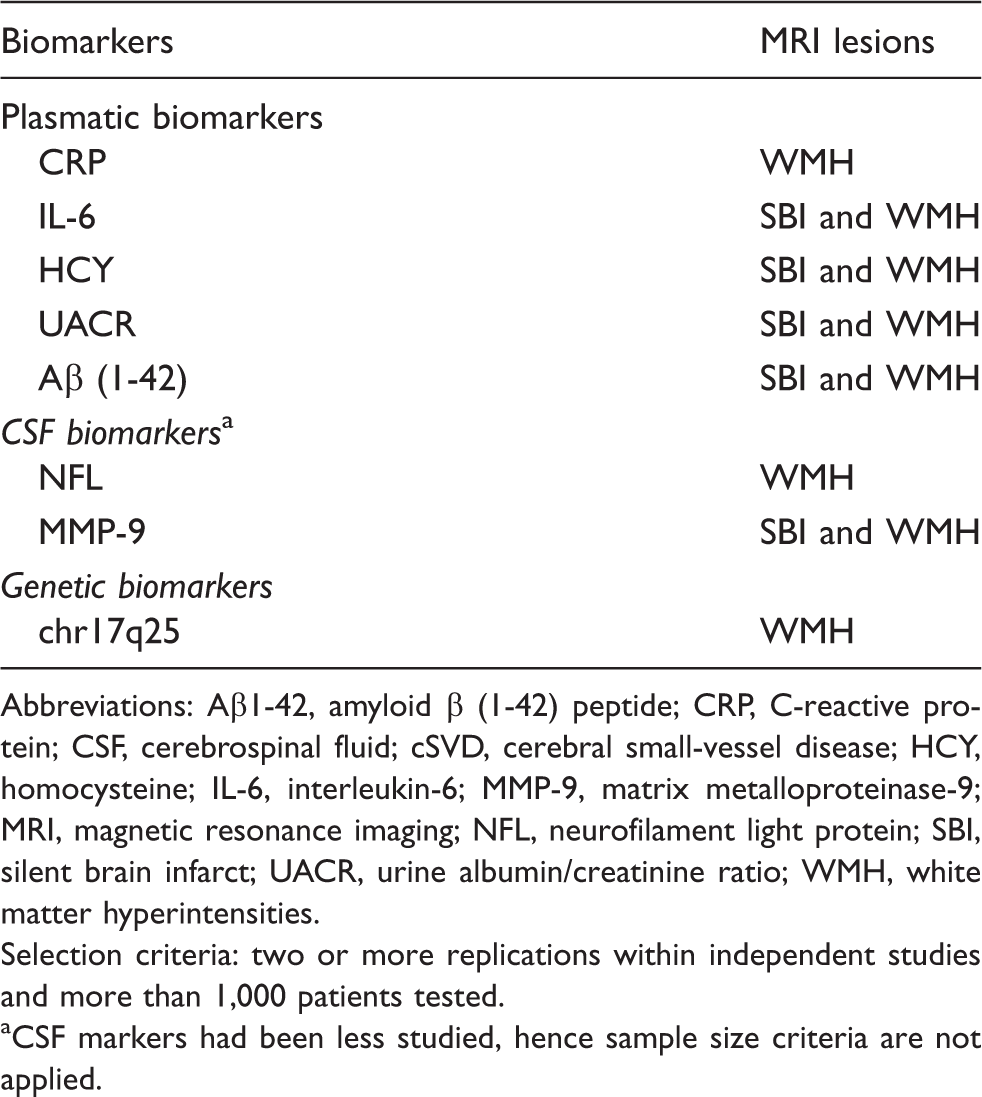
Available information for blood-circulating proteins highlights the involvement of several interrelated pathways (Figure 2A) including but not limited to neuroinflammation, hemostasis, and endothelial dysfunction. In addition, functional network maps using associated biomarkers may reveal new potential candidates (Figure 2B). Moreover, a deeper analysis of these pathways and links might be useful to find possible therapeutic targets in the future. A summary of the best performing biomarkers reviewed here is presented on Table 4. The majority of the studies performed to date with biomarkers show significant cross-sectional associations with several imaging or cognitive outcomes, but their predictive or discriminative ability regarding diagnosis remains to be established as well as the power of combining those different parameters in clinically useful scores.
(a) Main molecular pathways analyzed in subcortical ischemic vascular disease (SIVD). Pie chart of molecular pathways corresponding to those biomarkers reviewed with consistent association with SIVD lesions in more than 1,000 subjects. Portions represent percentage per number of pathways. (b) Functional network of biomarkers reviewed and their predicted partners. Network chart displaying prediction methods (neighborhood, gene fusion, cooccurrence, coexpression, experiments, databases, and textmining) applied to those biomarkers reviewed with consistent association with silent brain infarct (SBI) and white matter hyperintensity (WMH), and their predicted functional partners (underlined in red). Lines represent different link evidences according to different colors, based on databases such as Saccharomyces Genome Database (SGD), Online Mendelian Inheritance in Man (OMIM), FlyBase, and PubMed. Green head arrows: activation; red end lines: inhibition; green lines: coexpression; blue lines: binding; black lines: reaction; gray lines: statistically relevant cooccurrences of genes. Corresponding proteins to gene names of reviewed biomarkers displayed: troponin t (TNNT2), vascular cell adhesion molecule 1 (VCAM1), E-selectin (SELE), interleukin-6 (IL-6), lipoprotein phospholipase A2 (PLA2G7), C- reactive protein (CRP), intercellular adhesion molecule 1 (ICAM1), angiotensin converting enzyme (ACE), von Willebrand factor (vWF), plasminogen activator inhibitor-1 (SERPINE1), and P-selectin (SELP). Corresponding proteins to gene names of predicted partners displayed: urokinase plasminogen activator (PLAU), vitronectin (VTN), tissue plasminogen activator (PLAT), selectin P ligand (SELPLG), integrin beta 2 (ITGB2), integrin alpha L (ITGAL), interleukin-6 signal transducer (IL6ST), interleukin-6 receptor (IL-6R), troponin I type 3 (TNNI3), and troponin C type 1 (TNNC1); STRING database (http://string-db.org/). Best performing biomarkers in association with cSVD Abbreviations: Aβ1-42, amyloid β (1-42) peptide; CRP, C-reactive protein; CSF, cerebrospinal fluid; cSVD, cerebral small-vessel disease; HCY, homocysteine; IL-6, interleukin-6; MMP-9, matrix metalloproteinase-9; MRI, magnetic resonance imaging; NFL, neurofilament light protein; SBI, silent brain infarct; UACR, urine albumin/creatinine ratio; WMH, white matter hyperintensities. Selection criteria: two or more replications within independent studies and more than 1,000 patients tested. CSF markers had been less studied, hence sample size criteria are not applied.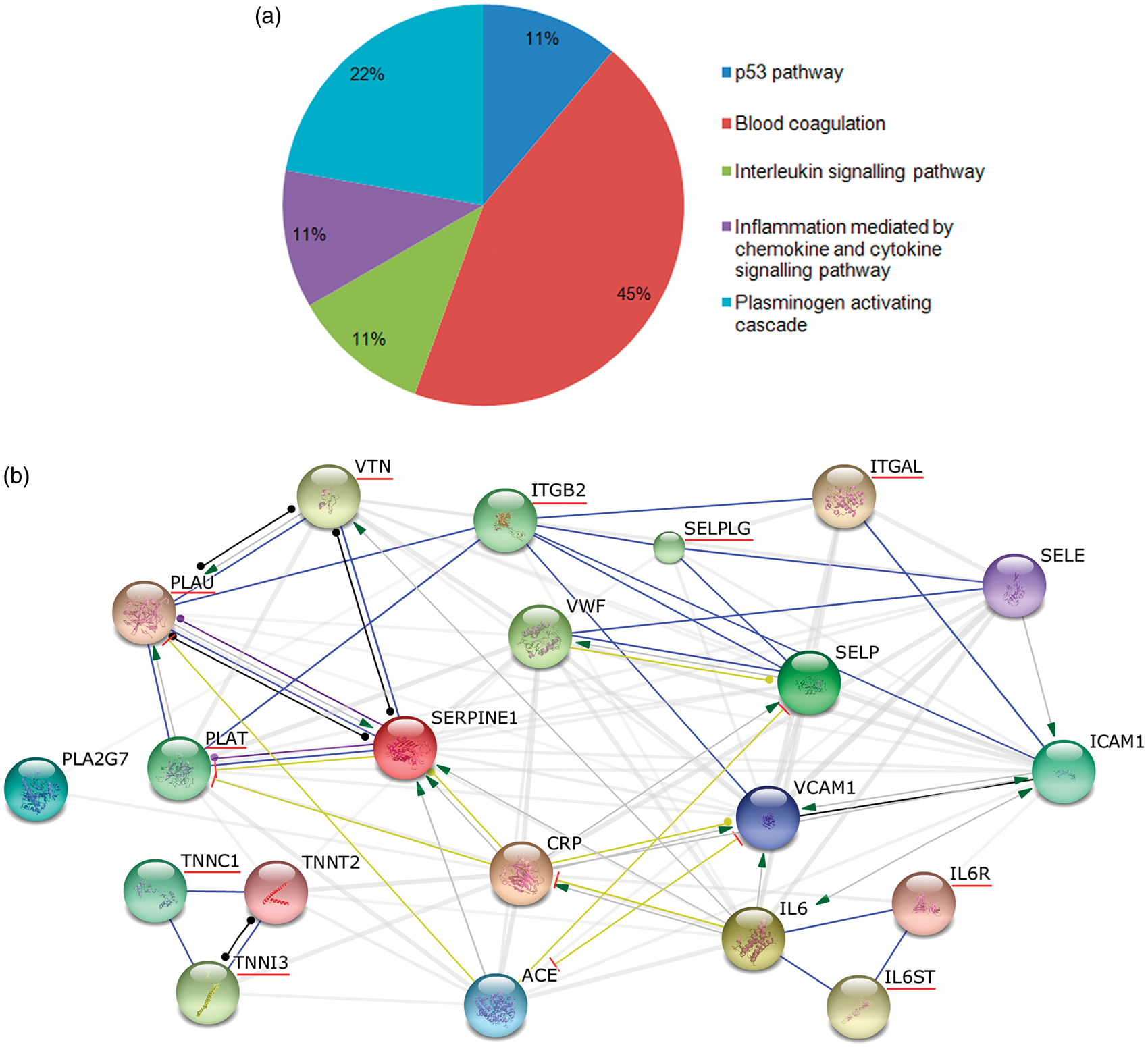
Also, some methodological issues might trouble the translation to clinical practice, such as the lack of replication of the findings in independent cohorts. This could be due in part, to the lack of consensus in the diagnostic criteria of these lesions in the past, the different ways to provide the results (i.e., WMHs rated considered as a volume measurement or with a qualitative assessment, etc.) and the different study design or statistical methods. An international effort to develop definitions and imaging standard for markers and consequences of cSVD is taking place, which will lead in the future to overcome these limitations. 116
Replication would also require the collaboration of multiple researchers sharing data from different populations and gathered in large consortiums. This approach has been proven useful in genome-wide association studies allowing unraveling genetic variants, which were not suspected before in this field.
Also, most studies in protein markers have analyzed mainly one or few candidate markers and, although several biomarkers involved in different pathways and combined in a diagnostic panel have been used in some recent studies, results should be replicated. Moreover, some promising candidate genes and proteins that are surrogates for the vascular risk factors behind SIVD such as hypertension might be explored and included in such panels.
Further, massive or nondirected proteomic approaches in well-characterized subjects with SIVD have not yet been performed. It is expected that in the near future, the use of this technology will lead to find new candidates.
Moreover, studies on the differentiation of different VCI subtypes have been scarcely performed in the past, most of them with reduced sample sizes and limited power to detect associations.
Finally, regarding the potential usefulness of blood biomarkers to predict the clinical course of VCI or even to monitor responses to potential new treatments, it is worth to mention that in the past few years some large population-based cohorts have started to report their results on how these brain lesions accumulate over time and on how blood biomarkers relate to this progression. What remains to be determined is whether biomarkers change in parallel with lesion accumulation or cognitive decline and can be used as surrogate markers for disease progression.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded with grants from the Fondo de Investigaciones Sanitarias (PI10/0705, CM10/00063, and CP09/136), from the Catalonian Society of Hypertension, the Càtedra-UAB Novartis de Medicina de Familia and IDIAP Jordi Gol, and from the Fundació Josep Palau Francàs. Neurovascular Research Laboratory takes part in the Spanish stroke research network INVICTUS (RD12/0014/0005).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Authors’ contributions
AV-B, IR-L, and JM helped in study conception and design, acquisition of data from the literature, analysis and interpretation of data, critically revised the manuscript for important intellectual content, and approved final version. CN, AB, and VL helped in study conception and design, acquisition of data from the literature, analysis and interpretation of data, drafted the manuscript, and approved the final version. PD helped in study conception and design, acquisition of data, analysis and interpretation of data, drafted the article, revised it critically for important intellectual content, and approved final version.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.