
Abstract
In the current study, the presence of cerebral cortical microinfarcts (CMIs) was evaluated in a series of 21 patients with a symptomatic high-grade > 50% stenosis of the carotid artery. A T2-weighted fluid-attenuated inversion recovery sequence and a T1-weighted turbo field echo sequence of the brain were obtained at 7.0 Tesla magnetic resonance imaging. Primary study endpoint was the number of CMIs and macroinfarcts. In total, 53 cerebral infarcts (35 macroinfarcts; 18 CMIs) were found ipsilateral to the symptomatic carotid artery, in 14 patients (67%). In four of these patients, both CMIs and macroinfarcts were visible. In the contralateral hemisphere, seven infarcts (five macroinfarcts and two CMIs) were found in five patients (24%). In the ipsilateral hemispheres, the number of CMIs and macroinfarcts were significantly correlated (
INTRODUCTION
Atherosclerosis of the carotid artery is an important risk for cerebral ischemia. In daily practice, patients are classified as high risk mainly based on the stenosis grade of the carotid artery.1,2 Recent literature confirms that plaque characteristics may contribute to specify subgroups with an increased risk of (recurrent) ischemic cerebral events.3–5 Moreover, the presence of infarcts in the brain parenchyma that downstream to these lesions may be important for accurate risk stratification. Patients with infarcts and cerebral symptoms were found to profit more from carotid endarterectomy (CEA), compared with patients with just ocular symptoms.6,7 Therefore, sensitive detection of brain lesions in patients with carotid artery disease may be fundamental for identifying patient (sub)groups with the highest risk of recurrent stroke who might benefit most from carotid surgery.
Magnetic resonance imaging (MRI) has a high distinctive capacity in the diagnosis of larger cortical and basal ganglia infarcts. However, from pathology studies it is known that smaller cerebral cortical microinfarcts (CMIs) can be too small for visualization with conventional
The aim of the present study was to evaluate the presence of CMIs in a series of patients with a symptomatic high-grade stenosis of the carotid artery on high-resolution 7.0 T MRI.
MATERIALS AND METHODS
Subjects
In patients who are scheduled for CEA, 7.0 T MR images of the brain were obtained < 36 hours before surgery. In all patients, a symptomatic carotid artery stenosis of ⩾ 50% was diagnosed, and the indication for revascularization was discussed within a multidisciplinary panel including neurologists, radiologists, and vascular surgeons. An exclusion criterion was inability to undergo 7.0 T MRI owing to the metallic implants not approved for ultra-high-field strength MR imaging. The medical ethics committee of the University Medical Center Utrecht gave approval for this prospective study, previously described, 12 and all patients gave written informed consent. The current study was conducted according to the guidelines of the Declaration of Helsinki.
Imaging
Ultra-high-field strength MRI was performed on a 7.0 T MRI scanner (Philips Healthcare, Cleveland, OH, USA) with a 32-channel receive-coil and a volume transmit/receive-coil for transmission (Nova Medical, Wilmington, MA, USA). The MRI protocol consisted of a T2-weighted fluid-attenuated inversion recovery sequence 13 and a T1-weighted turbo field echo sequence. The fluid-attenuated inversion recovery sequence was acquired in sagittal orientation with a field of view of 250 × 250 × 190 mm3, an acquired voxel size of 0.8 × 0.8 × 0.8 mm3, repetition time 8,000 ms, inversion time 2,250 ms, echo time 300 ms (equivalent echo time 154 ms), flip angle 100°, turbo spin echo factor 125, SENSE factor in anterior-posterior direction and right-left direction 2.5 × 2.5. Scanning time was 12 minutes 56 seconds. The T1 turbo field echo sequence was acquired in sagittal orientation with a field of view of 200 × 250 × 200 mm3, an acquired voxel size of 1.0 × 1.0 × 0.5 mm3 repetition time 4.8 ms, echo time 2.2 ms, flip angle 8° and scanning time was 1 minute 37 seconds.
Image analysis
Image analysis was performed with MeVisLab 2.4 (MeVis Medical Solutions AG, Bremen, Germany). The presence of CMIs and macroinfarcts on the high-resolution fluid-attenuated inversion recovery images and T, turbo field echo images of the brain were described, relative to the side of the scheduled CEA. The brain was systematically divided in seven regions: frontal, parietal, occipital, temporal, caudate nucleus, lentiform nucleus, and thalamus. For each of these regions, presence or absence and number of CMIs and macroinfarcts in both hemispheres were determined. CMIs were defined as infarcts < 3 mm in cortical length. Two observers (JH and AR), masked for each other's assessment, performed the image analysis; the intraclass correlation coefficient and 95% confidence interval of ipsilateral infarcts (macro and micro) has been evaluated for interobserver agreement. In a consensus meeting, final decision of all infarcts was made; the final infarcts were used for statistical analyses.
Statistics
First, the relation between number of infarcts and baseline characteristics (age, type of symptoms, and stenosis grade) was evaluated by a Kendall's tau test. Second, the relation between number of macroinfarcts and CMIs was evaluated by the Kendall's tau test and the median difference in number of CMIs and macroinfarcts in the ipsilateral and the contralateral hemisphere by a Mann-Whitney
Statistical analyses were performed in IBM SPSS Statistics version 20 (IBM Corporation, Armonk, NY, USA).
RESULTS
Subjects
Twenty-one patients with a symptomatic stenosis in the carotid artery, scheduled for CEA between May 2011 and September 2013, were included. Carotid endarterectomy was planned on the left carotid artery in 12 patients and on the right side in the remaining 9 patients. Of these patients, seven were diagnosed with a stroke, nine with a transient ischemic attack and five with amaurosis fugax. Mean age of the patients (14 male) was 69 ± 8 years. Baseline characteristics are presented in Table 1. Imaging was performed 1 day before surgery in 20 patients; for one patient, imaging and surgery were on the same day. The median interval between symptoms and imaging was 21 days (range 11–78 days). At increasing delays, the findings on MRI can less certainly be linked to the clinical symptoms. Nevertheless, the delay of 78 days was one single case. For the rest of the cohort, the range of delays between symptoms and imaging was 10–38 days. As the number of macro- and microinfarcts in this patient was not outlying, we decided not to exclude this patient from analysis.
Baseline characteristics of all included patients (
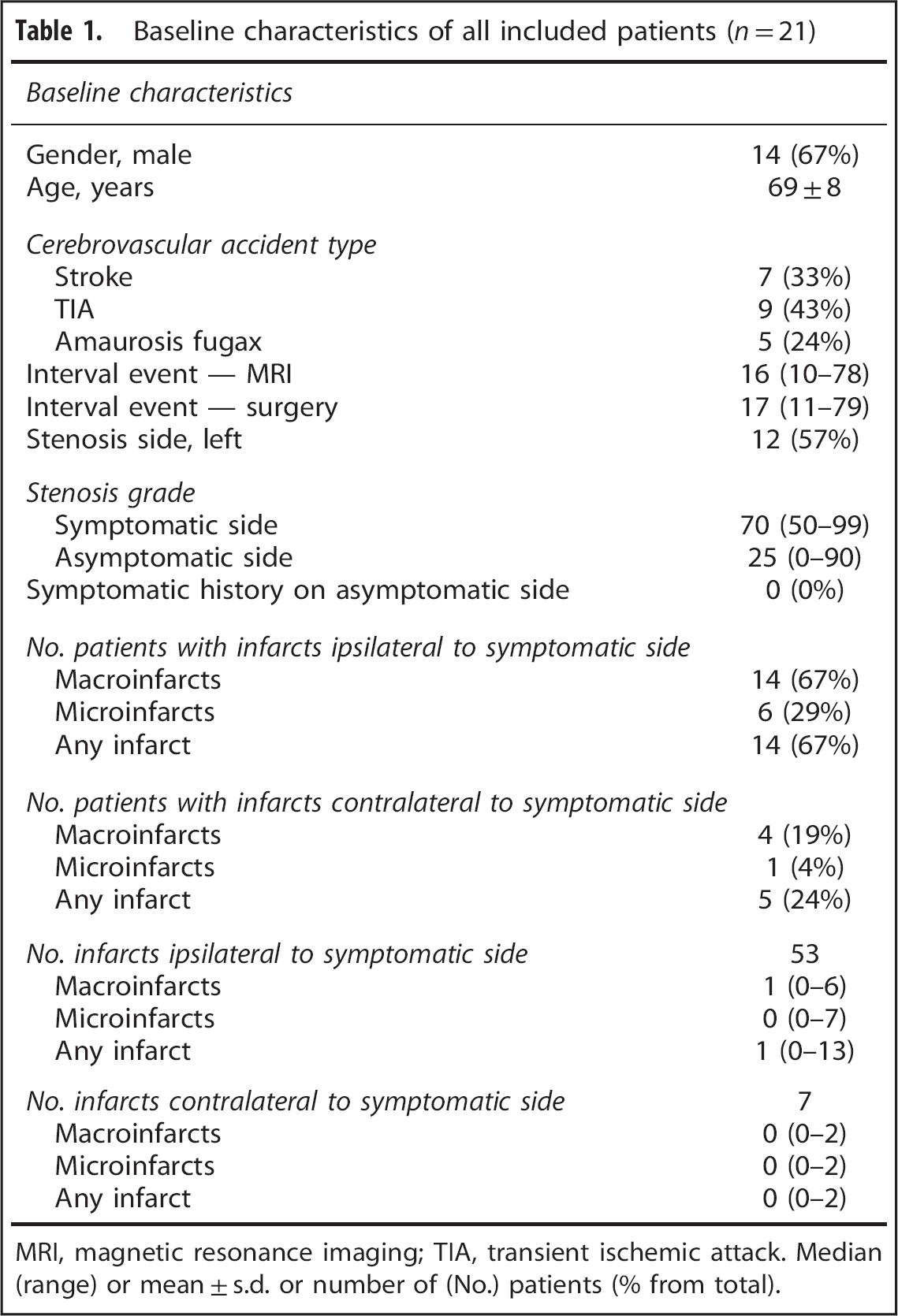
MRI, magnetic resonance imaging; TIA, transient ischemic attack. Median (range) or mean ± s.d. or number of (No.) patients (% from total).
None of the patients had a previous CEA of the ipsilateral carotid artery and none of the patients had a previous carotid revascularization or a history of symptoms on the contralateral carotid artery.
Cerebral burden
The determined interobserver agreement was strong for macroinfarcts and CMIs. The intraclass correlation coefficient was 0.78 (95% confidence interval = 0.53 to 0.90) for macroinfarcts and 0.80 (95% confidence interval = 0.55 to 0.92) for CMIs.
Both for the ipsilateral and contralateral hemisphere, no significant correlation was found between number of infarcts (macroinfarcts and CMIs) and stenosis grade. Both macroinfarcts and CMIs are also seen in patients with only ocular symptoms (amaurosis fugax). However, for both the ipsilateral and contralateral hemisphere, no significant correlation was found between number of infarcts (macroinfarcts and CMIs) and type of symptoms. In the ipsilateral hemisphere, no significant correlation was found between number of infarcts (macroinfarcts and CMIs) and age. In the contralateral hemisphere, a significant correlation only was found between macroinfarcts and age (
Results of Kendalls tau correlation test, assessing the correlation between the stenosis grade and the number of infarcts and the correlation between CMIs and macroinfarcts
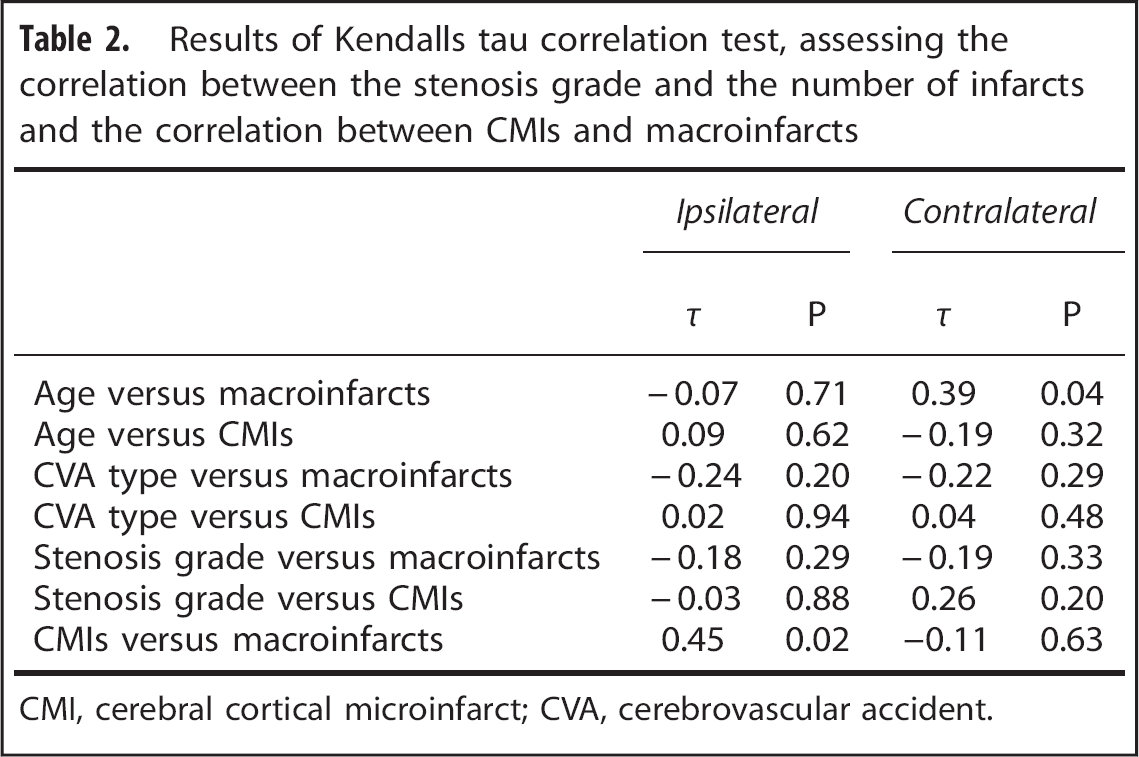
CMI, cerebral cortical microinfarct; CVA, cerebrovascular accident.
In 14 patients, 53 cerebral infarcts (18 macroinfarcts; 35 CMIs) were found ipsilateral to the carotid artery scheduled for CEA, compared with 7 infarcts in the contralateral hemisphere (5 macroinfarcts; 2 CMIs). An example of two CMIs in the ipsilateral hemisphere is given in Figure 1 and an example of one macroinfarct in the ipsilateral hemisphere is given in Figure 2.
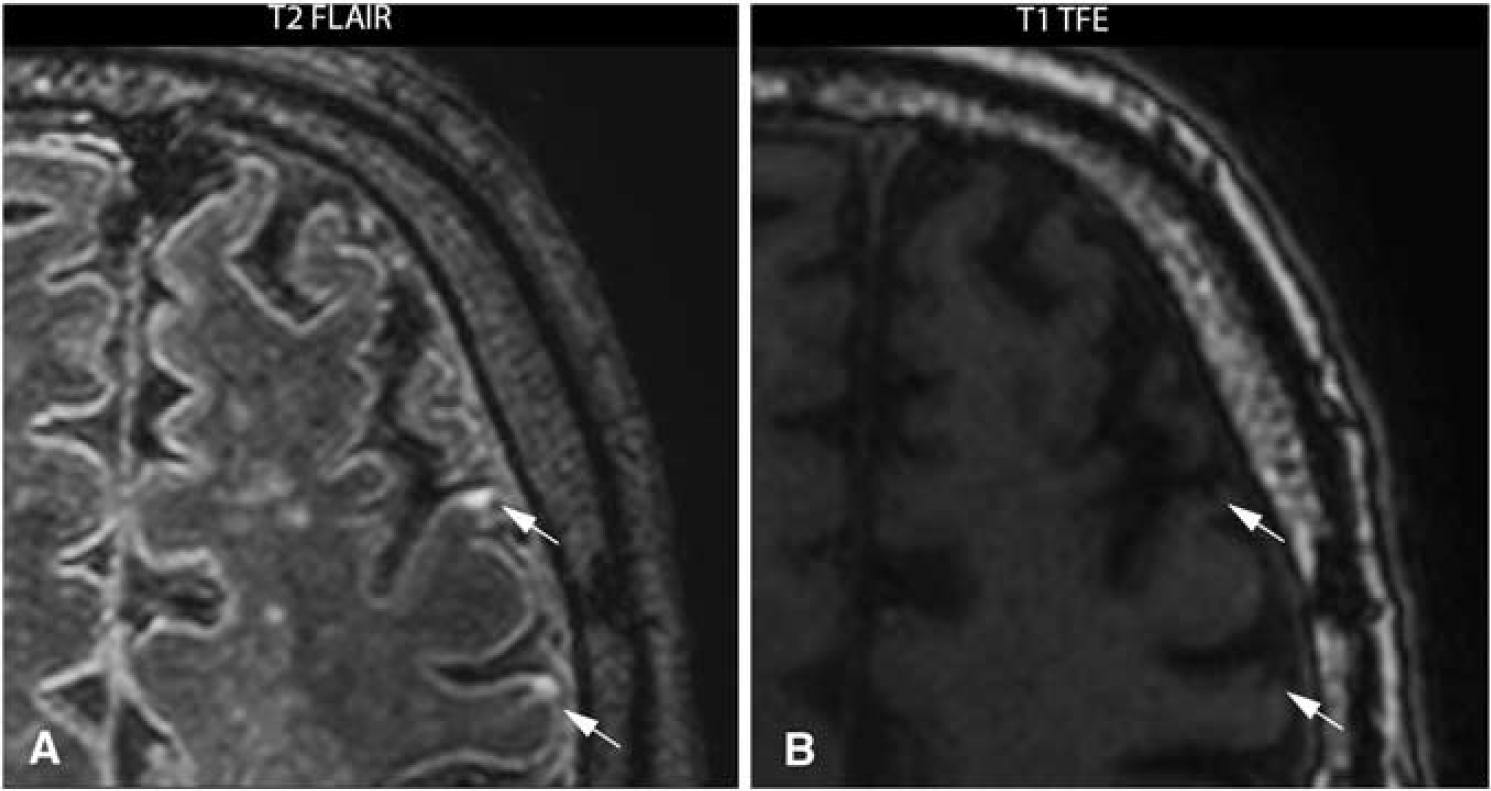
7.0 Tesla T2-weighted fluid-attenuated inversion recovery (FLAIR) image (
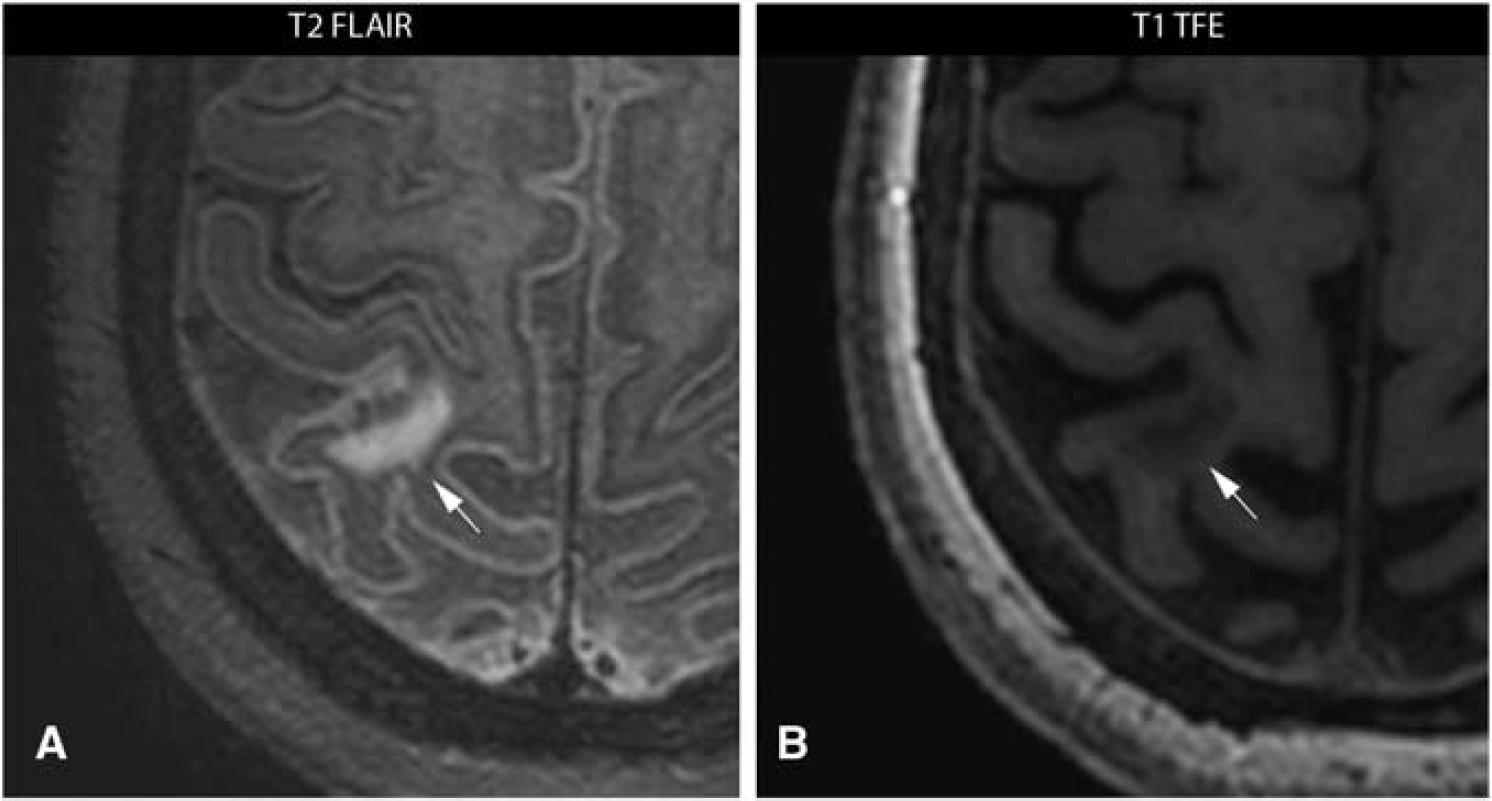
7.0 Tesla T2-weighted fluid-attenuated inversion recovery (FLAIR) image (
In all 14 patients with visible infarcts in the ipsilateral hemisphere, macroinfarcts were visible and CMIs were present in 4 of these patients. The presence of CMIs in the ipsilateral hemisphere was significantly correlated with the presence of macroinfarcts (
Results of Mann-Whitney
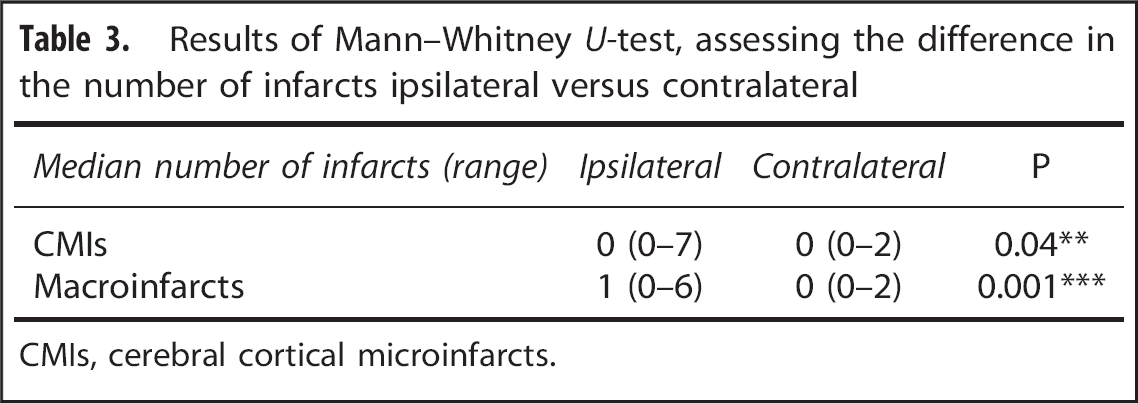
CMIs, cerebral cortical microinfarcts.
DISCUSSION
The current study is the first study that presents
CMIs are thus far mainly investigated in relation to dementia.8,11 However, recently, autopsy studies showed that CMIs are not limited to patients with dementia; in 6% to 43% of patients without dementia CMIs were found. 11 Besides, also a strong correlation was found between intracranial atherosclerosis and CMIs. 14 A prevalence of 43% in non-demented patients was found in a postmortem study in a general population cohort of people with an age of 75 years and older. 15 As the slice thickness in their specimens was already 10 micrometer, the size of microinfarcts visualized in this study were assumed to be much smaller than feasible for high-resolution 7.0 T MRI. In the current study, the prevalence of CMIs was 29% in the ipsilateral hemisphere and 5% in the contralateral hemisphere in a series of patients with a symptomatic high-grade atherosclerotic stenosis of the carotid artery. Because the CMIs in our study were found both in the ipsilateral and contralateral hemisphere and even in patients with only ocular symptoms, these infarcts may be the result of more generalized atherosclerosis. The significant higher prevalence of CMIs in the ipsilateral hemisphere in combination with the significant correlation between CMIs and macroinfarcts in the ipsilateral hemisphere is in agreement with the presence of a high-grade and possible vulnerable carotid plaque and patient symptoms.
In addition to the detection of CMIs, the current study is the second study thus far that evaluate cerebral (macro)infarcts at an ultra-high-field strength of 7.0 T. A previous study has shown that 7.0 T MRI enable to depict normal brain anatomy and ischemic lesions in patients with subacute and chronic stroke with a higher spatial resolution and more anatomic details. 16 In the current study, this high-spatial resolution was used to depict both macroinfarcts and CMIs.
As it is not guaranteed to find visible cerebrovascular damage in patients with a transient ischemic attack or amaurosis fugax, the finding that stroke patients have more often visible cerebral damage can be expected. However, both the number of macroinfarcts and CMIs are significantly higher in the symptomatic hemisphere, also in patients with only ocular symptoms. These findings suggest that CMIs prevail with the same pattern as macroinfarcts, and might also be an effect of the symptomatic vulnerable carotid plaque. The correlation between number of macroinfarcts and CMIs suggests that CMIs comprise a relevant part of the total cerebrovascular burden. Consequently, the ability to visualize CMIs
Although this is the first study that describes
Previous studies have shown that surgical treatment in the form of CEA is preferred over conservative treatment in patients with a symptomatic carotid artery stenosis of > 70% and moderately beneficial for patients with a symptomatic carotid artery stenosis of > 50%.19–22 Outcome of these studies was a clinical cerebrovascular event, whether visible on computer tomography (CT) or not. As CMIs are too small to visualize on CT, they were not taken into account in this setting. Thereby, in previous studies, CMIs are mainly related to global cognitive impairment and not to acute symptoms. 11 In the current study, no correlation was found between the stenosis grade and the visible CMIs (Table 2). This could be explained by the small range of stenosis grades in the current study because only patients with a high-grade symptomatic carotid artery stenosis are included. Although CMIs are seen with a similar pattern as macroifarcts, the clinical value of CMIs for risk stratification of patients with carotid artery atherosclerosis remains unknown.
In conclusion, the current study shows that in symptomatic patients with significant extracranial carotid artery stenosis, CMIs also impress as a relevant part of the total cerebrovascular burden and these CMIs prevail with a similar pattern as observed macroinfarcts. Assessment of this technique is needed in asymptomatic patients, patients with a lower stenosis grade, and healthy volunteers to explore and to validate the clinical benefit of visualizing cortical microinfarcts in these patients.
Footnotes
The authors declare no conflict of interest.
ACKNOWLEDGMENTS
We greatly acknowledge the use of MeVisLab (MeVis Medical Solutions AG, Bremen, Germany).