
Abstract
In 2006, Zamboni reintroduced the concept that chronic impaired venous outflow of the central nervous system is associated with multiple sclerosis (MS), coining the term of chronic cerebrospinal venous insufficiency (‘CCSVI’). The diagnosis of ‘CCSVI’ is based on sonographic criteria, which he found exclusively fulfilled in MS. The concept proposes that chronic venous outflow failure is associated with venous reflux and congestion and leads to iron deposition, thereby inducing neuroinflammation and degeneration. The revival of this concept has generated major interest in media and patient groups, mainly driven by the hope that endovascular treatment of ‘CCSVI’ could alleviate MS. Many investigators tried to replicate Zamboni's results with duplex sonography, magnetic resonance imaging, and catheter angiography. The data obtained here do generally not support the ‘CCSVI’ concept. Moreover, there are no methodologically adequate studies to prove or disprove beneficial effects of endovascular treatment in MS. This review not only gives a comprehensive overview of the methodological flaws and pathophysiologic implausibility of the ‘CCSVI’ concept, but also summarizes the multimodality diagnostic validation studies and open-label trials of endovascular treatment. In our view, there is currently no basis to diagnose or treat ‘CCSVI’ in the care of MS patients, outside of the setting of scientific research.
INTRODUCTION
In 2006, the vascular surgeon Paolo Zamboni 1 reintroduced the pathophysiologic concept of venous outflow pathology ultimately leading to multiple sclerosis (MS). He based this concept (or ‘the big idea’) on the well-known histopathologic features of a perivenous localization of inflammatory MS lesions. He coined the term ‘chronic cerebrospinal venous insufficiency’ (CCSVI) in analogy to perivenous inflammation in chronic venous insufficiency of the legs. While Zamboni's approach does not challenge the commonly accepted understanding of MS immunopathology, 2 it does relegate it to the final stage in the disease cascade. According to the ‘CCSVI’ concept, MS pathology starts with intracranial venous stasis based on a proximal obstruction of the main cervical and thoracic veins. This leads to perivenous diapedesis of erythrocytes in the white matter with subsequent release of iron, the actual catalyst of the widely known and accepted immune cascade. 1 The theory of venous outflow changes reaches back to the times of Charcot, who in 1868 provided an early histopathologic description of perivenous inflammation in MS. 3 In 1947, Putnam believing that thrombosis of the cerebral veins was a common finding in MS patients published preliminary results of treatment using dicoumarin in MS patients after experiments using induced sinus thrombosis in primates. 4 However, his findings have not been validated or revisited since this time. In 1986, Schelling posed the hypothesis that venous intracranial or intraspinal reflux has a significant role in the development of MS. 5 Subsequently, Zamboni et al6–8 published several studies that were meant to support the ‘CCSVI’ hypothesis. They applied catheter angiographies to show various extracranial venous outflow obstructions in the internal jugular veins (IJVs) or azygos veins, 9 and reported a correlation of the clinical course of MS with specific patterns of venous obstructions. 10 Subsequently, they reported improvement in the Multiple Sclerosis Functional Composite (MSFC) in relapsing remitting (RR) MS and a reduction in Gadolinium enhancing lesions on brain MRI during a mean follow-up of 18 months in a small monocentric open angioplastic intervention study. 9 The ‘CCSVI’ and its presumed efficacious therapeutic approach termed as ‘liberation treatment’ caused enormous interest in the scientific community, among patient support groups and in the media. Several clinical trials on angioplasty have started since, and numerous desperate MS patients seek relief from their incurable disease through questionable medical procedures. However, in the meantime the number of publications that refute the ‘CCSVI’ hypothesis has far exceeded that of its supporters. This review aims to analyze and critically comment on methodical aspects of ‘CCSVI’ in the context of (patho-)physiologic plausibility, which refers mainly to color-coded duplex ultrasonography (US), which is the only method according to Zamboni to define ‘CCSVI’. In addition, we aim to comprehensively present the literature on studies reproducing and confuting this theory, including treatment studies.
ULTRASOUND STUDIES
Venous Drainage and Neurologic Diseases
Currently, US is one popular technique for imaging the venous system. In the field of neurology, research begun to focus in the midnineties of the past century primarily on impaired venous drainage in primarily venous disorders like cerebral venous and sinus thrombosis.11,12 Subsequently, primarily nonvenous disease entities were studied. In transient global amnesia, an increased prevalence of IJV valve insufficiency (IJVVI) was seen which occurs in 20% to 30% of the normal population, but in up to 70% of transient global amnesia patients.13–15 A significantly increased prevalence of IJVVI was recently also shown for transient monocular blindness, 16 leucoaraiosis, 17 primary exertional headache, 18 primary intracranial hypertension, 19 and chronic obstructive pulmonary disease. 20 More recent research data suggest that the venous system may have a considerable role in arterial stroke. Yu et al 21 found that an impaired ipsilateral venous drainage due to a hypoplastic or aplastic lateral sinus (transversus and sigmoid sinus) was accompanied by pronounced infarction leading to higher morbidity and mortality. A further study analyzed whether collapsed veins as a result of intracranial artery occlusion might influence the extent of damaged brain tissue. 22
‘Chronic Cerebrospinal Venous Insufficiency’ Criteria—Are They Sound?
In 2007, Zamboni published the first US study investigating the relationship between impaired drainage and MS. The study was limited to the intracranial circulation, and provided the first description of an intracranial venous reflux in the deep cerebral veins (DCVs) defined by a retrograde flow of at least 0.5 second. 6 Two years later, he published a combined extracranial and intracranial US study, postulating four other criteria indicating impaired venous drainage, above the intracranial venous reflux which would later become his second ‘CCSVI’ criterion. 7 He specified the first criterion as extracranial reflux (>0.88 second) in the IJVs and/or vertebral veins (VVs) in sitting and lying position; the third criterion as a stenosis defined by a reduction in the crosssectional surface area (CSA) of the IJV of ≥50% or beyond a set threshold of 0.3 cm2; 8 the fourth criterion as a lack of flow in the IJV and VV again in supine and/or sitting posture despite visible vascular lumens; the final criterion as reverted postural control, in which the IJV does not collapse as would be physiologically expected in upright position. The study in which these criteria were presented and applied examined 109 patients and 177 nonaffected people. Zamboni found that each MS patient met at least two criteria, while none of the control group did. Thus, the sensitivity, specificity, the predictive, and negative-predictive values were each 100%. These astonishing results prompted other groups to attempt to confirm the findings using color-coded duplex sonography. Some research groups also found a very high prevalence of at least two positive criteria for MS patients alone, 23 while others described a relatively high proportion of healthy controls24,25 and patients with other neurologic diseases fulfilling the criteria. 26 In contrast, several other groups found that no or only few MS patients and healthy controls fulfilled the ‘CCSVI’ criteria.27–33 Despite these contradictory results, balloon angioplasty and stenting treatments of the venous system were performed based on these findings and are currently performed around the world. 34
The experience in ultrasonographic examination of cerebralvenous hemodynamics is limited, despite the fact that the technique is quite simple, and consequently well-researched and validated results describing normal and impaired venous drainage are lacking. Substantial data describing the normal venous blood flow using US have been published by our Berlin Charité research group in the past 15 years. Zamboni et al7–9 refer to our studies describing the venous outflow findings in MS patients and healthy controls. However, from our point of view, they misinterpreted our data leading to the logical conclusion that the Zamboni criteria are based in part on a misconception of our work. For this reason, we consider a methodological critique of ‘CCSVI’ concept a priority. We also consider the rash establishment of ‘CCSVI’ and particularly the concept of a ‘CCSVI’ syndrome 35 in the scientific literature, as questionable, because of the lack of scientific validation.
Recently, Laupacis et al 36 presented the first meta-analysis of existing results on the ‘CCSVI’ hypothesis, including all studies with MS patients and controls published so far. The meta-analysis explicitly addressed the question of ultrasound examination quality and suggests that one possible reason for a low prevalence of ‘CCSVI’ in some studies might be the insufficient experience of the investigators. 36 Interestingly, their analysis shows a significant negative association between the postulated qualification/experience of certain research groups and the number of their published ultrasound studies in this field.
The US examination of veins responsible of the intracranial drainage requires the consideration of the particular features and specific characteristics of the cerebral and cervical venous system which is essential for correct differentiation between physiologic variants/anomalies and pathologic findings. For example, unlike to other parts of the body, the cerebral venous system is valveless allowing a reversal of blood flow direction.37,38 Furthermore, intracranial veins are not capacitance vessels like the veins of the extremities, as they only dilate to a limited degree. A further characteristic is that they do not collapse in a vertical body position, because the skull is a sealed cavity.39,40 The situation is similar in the spinal cavity so that the term ‘craniovertebral cavity’ might be more accurate than the commonly referred to sealed ‘intracranial cavity’ . Another unique feature of cerebral venous drainage is its dependence on posture. Whereas in supine position the IJVs are the main drainage pathways, in upright position the IJVs generally collapse with the VVs and intraspinal veins compensating to a large extent.41–44 However, the IJVs are not always the main drainage veins in the supine position. In ~30% of healthy subjects, the extrajugular drainage pathways are at least similarly important for cerebral venous drainage. 45 Finally, anatomic and angiographic studies have shown that the drainage of the cerebral blood is asymmetric with a preferential outflow via the IJVs of the right side.46,47 These special characteristics are indispensable in the understanding of the craniovertebral venous drainage, although many of its aspects, for example, the postural mechanisms of the venous outflow have to be elucidated.
Point-by-Point Methodological Critique of the Zamboni Criteria
(1) Intracranial reflux. Zamboni introduced the criterion of intracranial reflux in 2007 and has not changed it afterwards. He defines intracranial reflux as a retrograde flow within the inner venous system of >0.5 second. 6 In this study, referring to intracranial veins, for which normal flow velocities and detection rates had been published in the past, is written in the Methods section: ‘using the trans-temporal acoustic bone window, we insonated at least one of the deep middle cerebral veins (dMCVs), including basal veins of Rosenthal, great vein of Galen, and internal cerebral veins, according to criteria previously described [Valdueza et al, 1996; Stolz et al, 1999; Zipper et al 2002]’ .48–50 However, none of these veins are presented in the figures. Instead, he shows that color-coded duplex signals of undefined vessels located in the white matter around the third ventricle, which are simply designated as orthograde and thus normal if blue-coded and as retrograde and thus pathologic if red-coded. The terminology used in the study is ambiguous. For instance, Zamboni refers to a group of veins as the ‘deep middle cerebral veins', but presumably means the ‘deep cerebral veins'. The deep middle cerebral vein is a clearly distinguishable vein that runs parallel to the middle cerebral artery and generally flows into the basal vein of Rosenthal (BVR). 51 In 2009, they again published a misleading image of an intracranial vein. 7 While the internal venous system, comprising the deep middle cerebral vein, the BVR, the internal cerebral vein, the vein of Galen, and straight sinus, is now correctly designated as the DCVs, Figure 2 of the paper presents a vein in the subcortical gray matter without any further identifying details. As the vein in the figure is coded red, Zamboni diagnoses venous reflux. A corresponding figure of a physiologic finding, which should in this case be coded blue, is not shown, although it is referred to in the figure legend. Another point of criticism is that a Doppler spectrum of a venous vessel is not shown although the Methods section states that the flow spectra and velocities in the DCVs were measured. The Doppler spectrum is important for a reliable differentiation from arterial signals based on its pulsatility, which is generally clearly lower for veins. Besides that, the typically low venous blood flow velocity often requires the use of a Doppler spectrum for a correct analysis of venous flow direction. Thus, venous anatomy and hemodynamic cannot be assessed just by color signals. Furthermore, arteries can overlap with veins in imaging, which is another reason that the Doppler spectrum should be derived for every vascular segment examined.
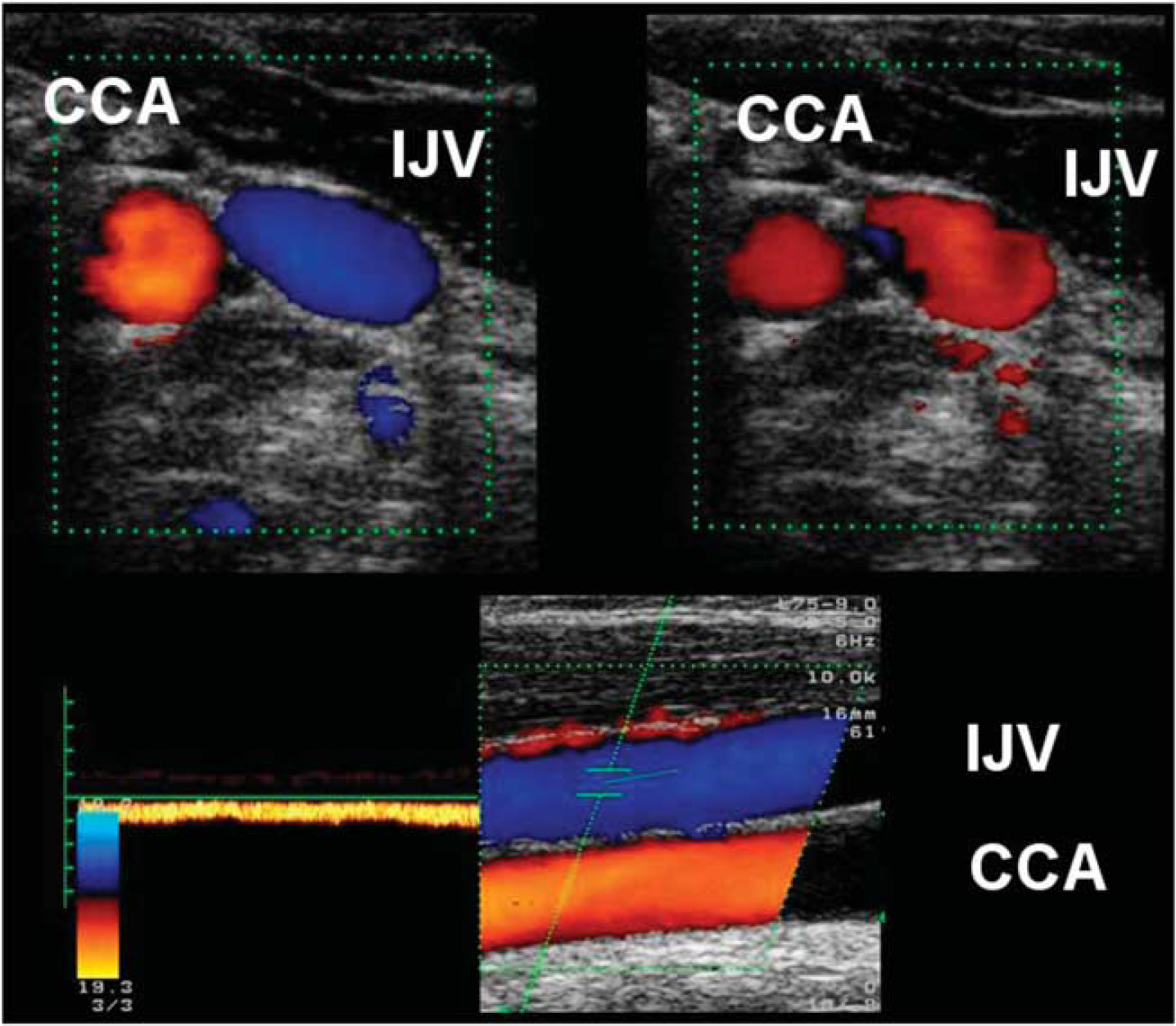
Extracranial color-coded duplex sonography of the internal jugular vein (IJV) and common carotid artery (CCA) in a transverse (top) and longitudinal (bottom) plane. Blood flow direction in the IJV seems to vary at different time points using a transverse insonation (top left: orthograde flow, blue coded; top right: retrograde flow, red-coded). Additional insonation in the longitudinal plane shows the continuous orthograd flow, blue-coded.
Zamboni defines venous reflux of DCVs as a red color-coded signal or rather as a flow signal toward the probe. This seems to be very crucial. Although the DCVs and the straight sinus run toward the occiput, causing predominantly a blue color-coded signal away from the probe, the BVR, for example, shows a red signal running toward the probe along its proximal section. A flow away from the probe is seen in its middle and distal sections. Correspondingly, the posterior cerebral artery, which runs parallel to the BVR, shows a red signal proximally and a blue signal distally (Figure 1). Due to its anatomic position in relation to the midbrain and the posterior cerebral artery, the BVR is detectable in almost 100% using color-coded duplex US, particularly in its middle and distal sections. In comparison, the other DCVs are more difficult to investigate using transcranial color-coded sonography. This especially applies to the internal cerebral veins, showing a detection rate of ~10% to 20%.48,52 As the anatomy of the BVR is extremely stable and forms part of the internal venous system, a flow toward the probe in the distal BVR can definitely be regarded as a pathologic finding. However, an image of a retrograde flow in the BVR was never shown by Zamboni. As a side note, a retrograde flow signal in the BVR can also be present in cerebral venous thrombosis12,48 and tumor-induced obstructions of the straight sinus,53,54 as well as in arterio-venous angioma. 55
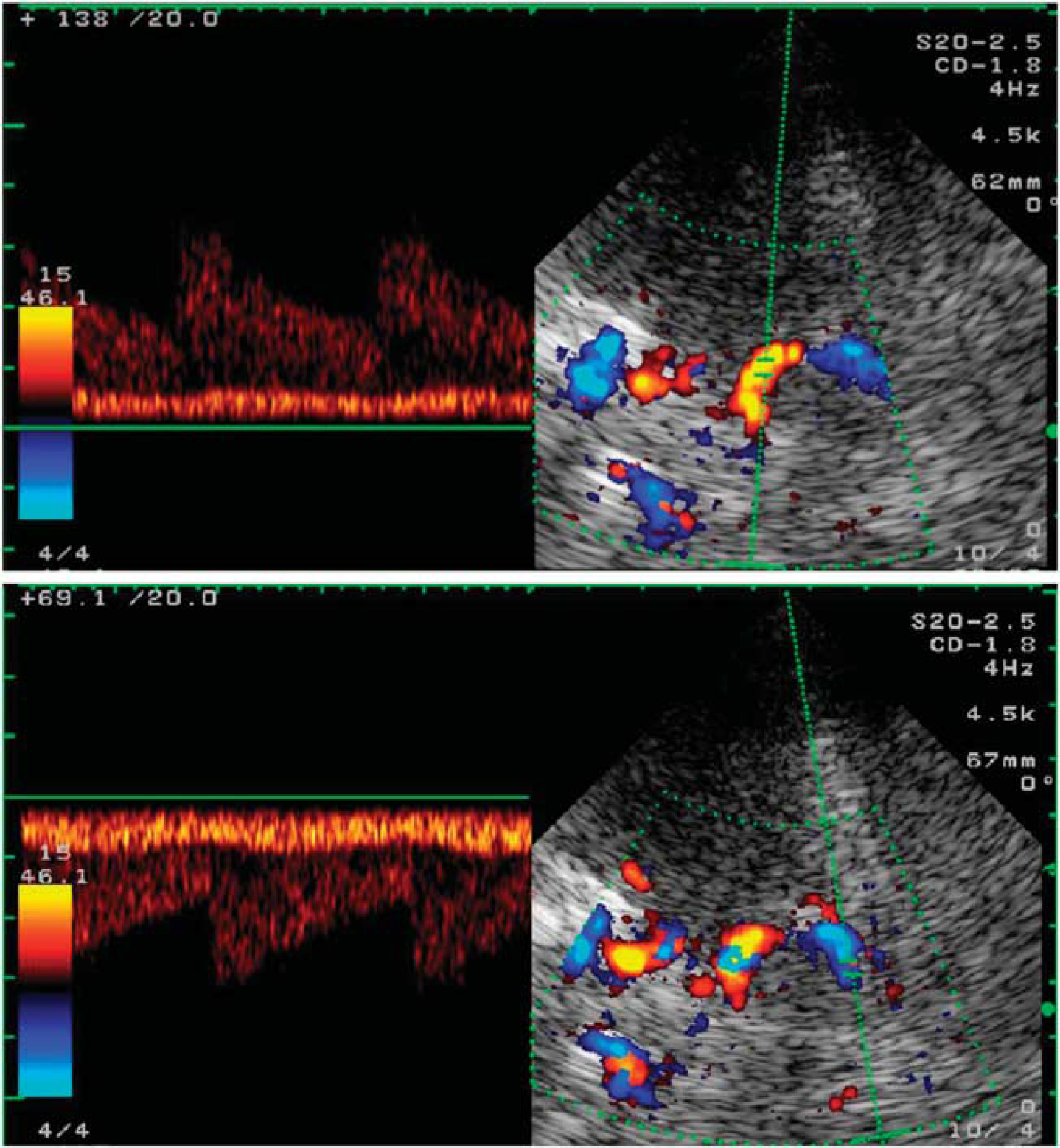
Transcranial color-coded duplex sonography of the basal vein of Rosenthal (BVR) with low flow velocity and pulsatility together with the posterior cerebral artery (PCA) with high flow velocity and pulsatility using a transtemporal axial approach at the mesencephalic plane. Notice the physiologic change of blood flow direction with a red-coded flow toward the probe (top) in the proximal and blue-coded away from the probe (bottom) in the distal part of the BVR as well as in the PCA.
Another crucial question regards Zamboni's definition of intracranial reflux as a retrograde flow of longer than 0.5 second. This threshold derives from studies on venous insufficiency of the legs, in which a reflux of at least 0.5 second after deflating a compression cuff was defined as pathologic. 56 Although we do agree that a spontaneous or induced retrograde flow of half a second in the deep venous system is probably not physiologic, a direct transfer from legs onto a different anatomic environment, namely intracranial drainage remains problematic.
(2) Extracranial reflux in the internal jugular vein and the vertebral vein. In the 2009 study, Zamboni et al 7 defined a retrograde flow in the IJV or VV as lasting >0.88 second. The Methods section states that ‘For each assessment the direction of flow is [analyzed either with the pulsed wave mode and the sample placed in the vessel, at a 60° angle, or with the color-coded mode, by comparing the color of the flow in the IJV/VV with that of the satellite carotid and/or vertebral artery, respectively. Either the IJVs or the VVs can be examined by using both the transversal and/or the longitudinal cervical access'. Again, from the methodological point of view, we strongly recommend assessment by pulsed-wave Doppler mode in addition to color-coded mode. The longitudinal oriented cervical veins have to be examined by ultrasound in longitudinal planes in each case, as due to the Doppler formula, reliable measurements are dependent on the ultrasound angle, and ultrasound application at 90° can misleadingly suggest zero flow. The presented figure in this paper only shows a transversal section through the IJV and the common carotid artery, which both show a red signal, thereby suggesting a retrograde flow in the IJV. Transversal IJV examination may be adequate for determining flow direction in hurried routine examinations especially as using this method the probe can be adjusted to improve the angle of the ultrasound beam. In clinical research, stringent methodological standards have to be fulfilled, and the cervical veins definitely have to be assessed to determine the longitudinal flow direction.
Additionally, the IJV can also exhibit a nonpathologic oscillating signal with a positive and negative flow that is often observed, especially in the elderly. This is instantly identifiable in the longitudinal and transverse imaging analyzing the Doppler spectrum in the pulsed wave mode, but which can suggest reflux using only a snap shot with the color-coded US (Figure 2).
Zamboni et al 35 define extracranial reflux as having a duration of >0.88 second, in contrast to intracranial reflux, which is assigned a duration of >0.5 second. The different threshold for intracranial and extracranial reflux remains unanswered. They argue that the value of >0.88 second allows to differentiate between a physiologic and pathologic reflux, adopting this threshold value from a study that examined IJVVI during a Valsalva maneuver (VM). 57 The validity of this approach is questionable, because reference values gained during a VM do likely not apply to situations where flow measurements take place in resting conditions. The reference to the VM is relevant to the extent that to date only the presence of IJVVI has been evaluated as criterion of compromised venous drainage. Apart from the 0.88 second proposed by the research group of Nedelmann as reflux threshold, other methods have been proposed to define IJVVI.20,58,59 An increased prevalence of IJVVI has been found for several neurologic (transient global amnesia, amaurosis fugax, and leucoaraiosis)13–17 and non neurologic diseases (primary pulmonary hypertension, chronic obstructive pulmonary disease, and primary exertional headache).18,20 The sole publication on MS patients reported no significant difference to the control group. 31 Despite the fact that neurologists debate the significance of valve insufficiency for several years, the Zamboni group has not yet addressed this in MS patients, not even in the form of a critical discussion of the literature available to date.
Second, it seems inconsistent to define pathologic reflux in the intracranial and extracranial veins by two different time values. Despite these methodical problems, similarly to the intracranial system, a retrograde flow in the IJV or VV during resting conditions should be interpreted as a sign of a compromised venous system. Pathologic retrograde IJV flow has been described for innominate vein occlusion. 60 However, this does not necessarily have a clinical consequence, as the literature also includes a description of a postural retrograde IJV flow in response to compression of the left brachiocephalic vein in the supine position. 61 We recently observed such a case, in which the ipsilateral VV exhibited a retrograde flow in the supine position, turning in an orthograd flow in the upright position (Figure 3).
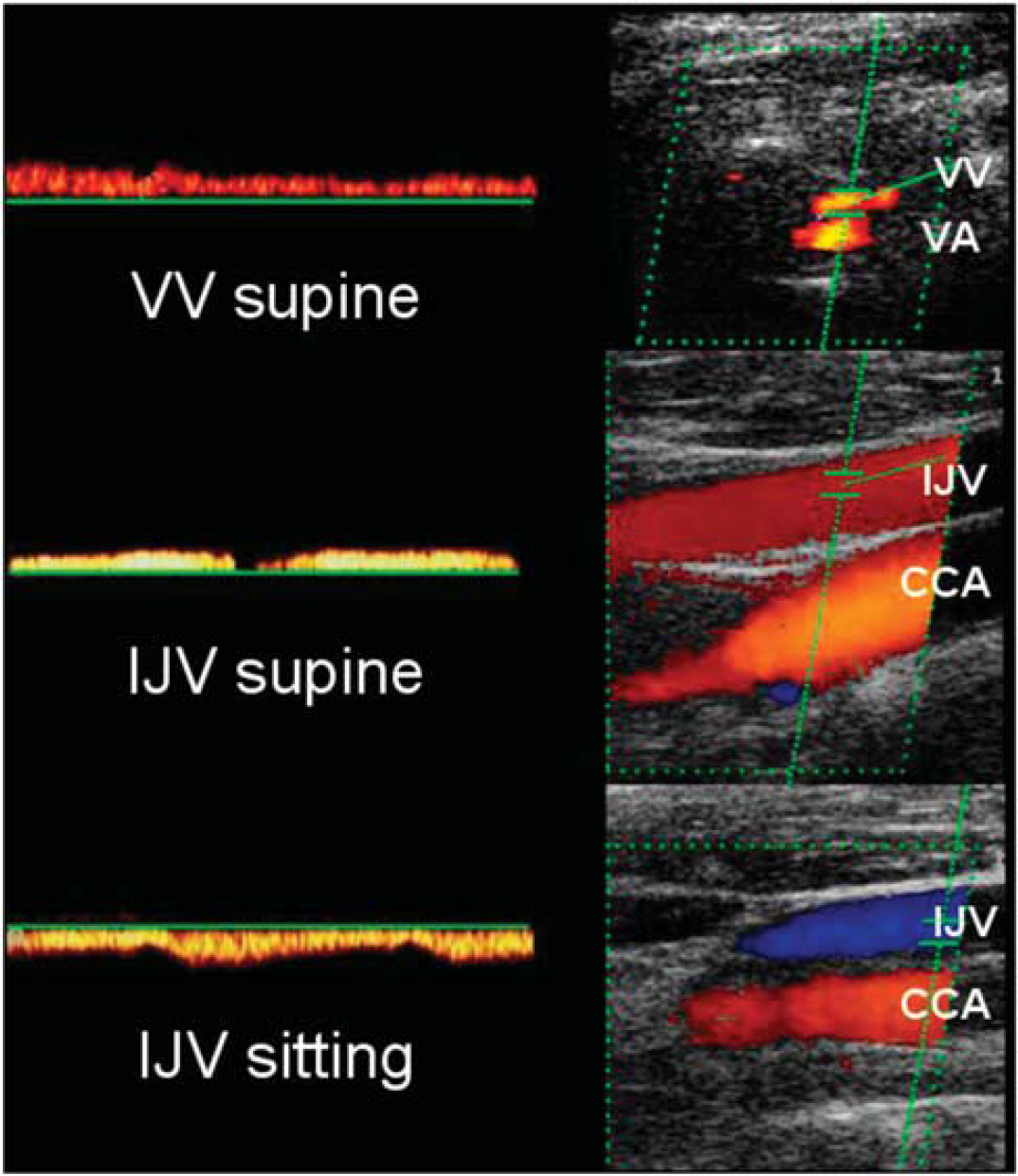
Postural changes of blood flow direction in the vertebral vein (VV) and internal jugular vein (IJV) in a healthy subject. Retrograde blood flow in the VV (top) and IJV (central) in supine position turning into an orthograd flow in both vessels after postural change toward the sitting position (bottom) (VV not shown). Note the orthograd flow in the vertebral artery (VA) and common carotid artery (CCA).
(3) Proximal stenosis of the internal jugular veins. Zamboni introduced two different criteria of proximal IJV stenosis in 2009. An at least 50% reduction in the vascular CSA of the IJV was his first suggestion. 7 Shortly after, he considered a threshold of 0.3 cm2 of the CSA of the IJV as a stenosis. 8 Both criteria can be refuted based on methodological and anatomic considerations. The IJV is significantly wider at its point of origin in the upper bulb and its confluence into the subclavian vein in the lower bulb. 62 The crosssection of the medium section, which unlike the cranial sections can always be imaged using duplex sonography, varies greatly depending on the position of the head, posture, and the central venous pressure. Defining stenosis as a 50% reduction in the vein's CSA is therefore not practical. Additionally, the location of the designated normal reference lumen has never been defined.
The second approach seemed more plausible, as it claimed to be based on a published US study by Lichtenstein et al, 63 in which an IJV crosssection of ≤0.3 cm2 apparently ‘was not found in any examined subject’ . However, the study in fact stated that 23% of the subjects had an IJV area of ≤0.4 cm2 and the included diagram shows 21 measurements with a CSA of ≤0.3 cm2 without pathologic meaning. Furthermore, interpretation was already limited as the study focused on patients in intensive care and did not include healthy subjects. Therefore, Zamboni et al based their conclusions on misinterpretation of a previous study. It has also to be mentioned that in this work the area of the IJV was measured 15 mm above the cricoid cartilage which does not exclude smaller areas at more proximal or distal locations. Moreover, one other ultrasound study performed in 10 healthy volunteers measuring CSA of the IJV just above the carotid bifurcation showed a range of CSA on the right IJV between 0.11 and 0.77 cm2 and on the left IJV between 0.13 and 0.5 cm2 again refusing the proposal of the Zamboni group. 64 This is not surprising, as central venous drainage is not only dependent on posture, but as mentioned above, shows a preference for the right side.46,47,63 This has a physiologic basis, in that the blood of both hemispheres primarily flows via the unpaired superior sagittalis sinus into one transverse sinus, preferentially the right, and finally enters the ipsilateral IJV. In contrast, the unpaired straight sinus collects the blood of the centrally located DCVs (temporomesial, basal ganglia, and thalamus) and flows preferable into the left IJV primarily via the left transverse sinus. The real flow conditions and vascular diameter of the IJVs at least depend on the anatomic configuration of the confluens sinuum. In the simplest case seen in an autopsy study on 600 adult cadavers, in ~25% of cases the confluens sinuum forms a complete connection between the superior sagittal sinus and straight sinus with a similar distribution of venous blood to both IJVs. However, in ~10% of cases the confluens sinuum is missing, such that hemispheres drain completely separately. 65 Venous drainage is dominated by the right side in ~50% of cases and is dominated by the left side or is distributed evenly across both sides in ~25% of cases. Consequently, particularly in the left IJV, a low blood flow volume with small vessel diameter should be considered as physiologic, rather than pathologic.
(4) Absence of blood flow in otherwise detectable internal jugular or vertebral veins in lying and/or upright posture. The question arising here is whether this criterion reflects a pathologic condition. The fact that normal cerebral venous drainage is strongly dependent on posture was already mentioned above. Whereas the IJVs dominate in most subjects in the lying position, the extrajugular drainage pathway, including the VVs, has an important role in the upright position, while the IJV collapses to various degrees. In this posture-dependent interplay between the IJVs and the extrajugular veins, it is physiologically comprehensible that one of them may display no flow even if lumens are visible. In a first study, we examined 23 young healthy subjects with duplex sonography in different body positions. 44 While in the supine position at 0°, venous blood outflow was found in at least one IJV in all subjects. In the upright position, nine subjects showed complete cessation of blood flow in both IJVs. In two subjects, flow already ceased at 15° with visible lumens. Thus, 39% of the subjects showed bilateral zero flow in the IJVs in at least one posture. A concomitant flow increase was found in the VVs, not compensating the complete difference of blood flow in the IJVs. An absent flow in the IJV even in the supine position has been described in a further investigation of our group. 45 The postural dependency of cerebro-venous outflow has also been shown in MRI investigations 41 and was already observed using a conventional catheter approach.66,67
Zamboni et al 35 used these results to support their arguments, but substantially misrepresented these findings: ‘We assessed the lack of a Doppler detectable venous flow in the IJVs and/or VVs despite numerous deep inspirations. In normal subjects, this finding was never observed with the head in any position [Valdueza et al 2000]’ It is crucial to clarify that a cessation of blood flow in one or both IJVs in supine or upright position cannot be considered to be clinically relevant.
The VVs also warrant particular attention. In early anatomic studies, the VV was not considered to be a relevant vessel, but instead as a venous plexus around the vertebral artery. In contrast to the IJVs, which have been the focus of anatomic and physiologic research since the first days of duplex sonography,68,69 up to now only one paper has been published reporting detection rates and flow velocities of 138 healthy subjects (mean age ± s.d. 42.1 ± 14.5 years) in supine position. 70
A bilateral flow was seen in 62% of the subjects, while 17% showed unilateral flow. Twenty-one percent showed no flow bilaterally, although the VV lumens were generally visible proximal to the vertebral artery. The prevalence of blood flow changes in the VVs seems to be age related. In a younger population (mean age ± s.d. 27 ± 7 years), only 4% presented no flow in the VVs. 45
These results underline that the cerebral venous drainage is strongly dependent on the postural status, in which the IJVs usually assume the main role in supine position, whereas its significance decreased as the posture becomes more upright due to IJV collapse and blood flow in the VVs increases as partial compensation. Thus, a lack of flow in the VV in supine posture in a noncollapsed vessel is not pathologic. In contrast, a lack of a compensatory flow increase in the VVs in upright position seems to be unusual in our experience, and a lack of VV flow in standing position when the lumens are visible would be practically impossible.
As a side note, the criterion of zero flow in a visible vein has been a key source of uncertainty for research groups that have applied the Zamboni ultrasound protocol, as it was unclear whether the definition referred to a lack of flow unilateral or bilateral, in one or both postures or on both sides in both postures. Our initial interpretation of his argument was that a lack of flow had to present in both IJVs or both VVs in both positions. This would explain why our application of this Zamboni criterion found much lower prevalence than Zamboni himself. Only the accidental discovery of a reference to our publication on the internet brought to our attention that Zamboni considers zero flow in a single vein, independently of posture, to be a pathologic symptom. 71
It should also be pointed out that ultrasound examinations of the VVs often lead to an unintentional compression of the IJVs and thus to a compensatory increase in the VV flow. We observed a similar phenomenon in patients with a postoperative status after neck dissection with resection of an IJV. 72 It seems very likely to us that groups unable to find a lack of flow in the VV fell victim to false-positive results. Even experienced investigators might find positive blood flow in the VVs due to accidental compression of the IJVs when the subject changes posture. But, again, we must emphasize that the absence of blood flow is not a pathologic condition per se.
(5) Lack of collapse of the V. jugularis interna in upright posture. Collapse of the IJVs in upright position is a physiologic effect of the decrease in hydrostatic pressure and should not be considered as a pathologic phenomenon. Therefore, lack of postural-dependent IJV collapse may indicate proximal venous obstruction and has been observed in a few cases in one of our own studies. 30 However, in subsequent examinations we found that we had probably mistaken other veins for the IJV in the upright position, as the IJV was frequently completely collapsed. To identify the IJV with certainty, researchers should either continue ultrasound monitoring of the IJV as the subject stands or sits up or perform a short VM to dilate the IJV. Furthermore, to assess the real hemodynamic relevance in cases of absent venous postural collapse the differences of blood flow volume between the supine and sitting body position should be analyzed. In the only one published work using blood flow volume measurements, we found a significant higher decrease in blood volume flow in the sitting position in normal subjects, suggesting an even better venous drainage via the IJVs in this position in MS patients. 30
What Remains of the Zamboni Criteria?
Both the number of criteria (5) and the idea that two positive criteria suffice for the diagnosis of ‘CCSVI’ seem quite arbitrary. There is some evidence that a retrograde flow in clearly defined intracranial venous vessels of the deep system should be considered as pathologic criterion. The same is true for reflux in the extracranial veins of the neck, although in some cases the effect could be due to a nonpathologic, posture-dependent compression of the brachiocephalic vein. Of course, any application of the reflux criteria should be based on definitions which are actually not available. Both reflux criteria of Zamboni are insufficient and methodologically inadequate. Research groups with long-standing scientific expertise in ultrasonic vein analysis of cerebral drainage, such as the group of Nedelmann/Mayer and our own group, have not been able to show extracranial or intracranial reflux in MS patients or healthy controls.30,31 This suggests that the phenomenon does not exist in MS.
As outlined, the absence of blood flow and that what Zamboni called stenosis are in fact physiologic and not pathologic. Their inclusion in the criteria was based on misinterpretations of former studies.
As at least two of the five criteria (proximal IJV stenosis and absence of blood flow in the IJV(s) and/or VV(s)) are in fact a nonpathologic phenomenon, it does not surprise that their prevalence can surely be observed widespread. The proportion of cases meeting at least two of the criteria would have been higher also in our study, if we had interpreted Zamboni's fourth criterion in the above-mentioned manner.
Following the above explanations, the 2009 ‘CCSVI’ concept of the Zamboni group is in fact not salvable. Very recently, Zamboni published a so-called consensus manuscript, in which the early ‘CCSVI’ protocol for venous analysis was newly adapted. 73 A detailed discussion of all alterations would be out of frame for the current manuscript. Concerning the extracranial and intracranial reflux the new criteria now also include a bidirectional flow as a pathologic pattern. To our opinion, this phenomenon is rather indicative for an IJVVI and should therefore also be a possible finding in the healthy population. Considering the intracranial veins, an unusual and so far nonvalidated insonation approach is being introduced. The ≤0.3 cm2 ‘stenosis’ criterion is modified to a mandatory missing CSA increase during a standard VM. They added an additional alternative criterion including ‘and/or other B-mode anomalies', like intraluminal defects such as flaps, septa, or malformed valves combined with hemodynamic changes (block, reflux, and increased blood flow velocity). Furthermore, the zero-flow criterion on one side in the IJVs and/or VVs in both body positions permits now a bidirectional flow in one position and a zero flow in the other position. Finally, while the early criterion 5 required CSA increase in the sitting position, now a position-independent CSA is sufficient as a pathologic criterion.
With the ‘old’ ‘CCSVI’ criteria being refuted, the ‘new’ criteria seem to call for new confirmatory studies to confirm or refuse the new results. 73 However, the scientific quality appears unaltered low, as the core statements of our critical discussion also apply to the new modified criteria.
Venous obstruction in neurologic diseases is an exciting area of research and misleading hypotheses should not be allowed to compromise future investigations. Therefore, we are concerned that Zamboni's concept of ‘CCSVI’ will be adopted by himself or other groups for investigations in other fields in neurology.
OTHER IMAGING STUDIES
Magnetic Resonance Venography
Substantial points of criticism of ultrasound methodology are operator dependency and the limited options in terms of operator blinding. Magnetic resonance venography (MRV) is a well-established and robust method for the evaluation of the intracranial and extracranial (neck) venous system in vivo.74–76
A first study using a 3D contrast-enhanced MRV and 2D phase-contrast flow quantification in 21 patients with RR MS and 20 healthy controls subjects showed no substantial differences between MS patients and healthy controls in terms of blood flow or a possible reflux in the IJV. A narrowing of the IJV was observed in three patients who also showed a corresponding lower blood flow in the IJV. 77 Similar results were obtained in a second study using 3D contrast-enhanced and 3D phase-contrast MRV in combination with a 2D phase-contrast flow quantification of the internal cerebral veins and straight sinus. Anomalies of the extracranial (neck) and/or intracranial venous system could be observed in 50% of the MS patients and 40% of the healthy controls. An additional associated anomaly of the venous drainage (e.g., compensatory collateral drainage) was found in six MS patients and five healthy controls. Interestingly, none of the MS patients and healthy controls (regardless whether they had a venous anomaly or not) showed a venous backflow in the internal cerebral veins or straight sinus. 78 These findings underscore once again the assumption that the venous anomalies in terms stenosis are not pathophysiologically relevant and rather reflect anatomic variants than pathologic conditions.78,79 Magnetic resonance venography seems also more sensitive to detect IJV narrowing compared with color-coded duplex US. 80
Even in terms of IJV morphology and the presence of a prominent/collateral extracranial venous drainage, no significant differences between MS patients and control subjects could be detected in a study including 57 MS patients and 21 controls. 81 In this context, it is worth noting that venous anomalies (narrowing) can more frequently be found in older MS patients with a longer disease duration, suggesting that these findings may be age related. 82
A substantial criticism regarding the assessment of the venous systems with MRV is the limited value of conventional MRV compared with US in the detection of venous pathology particularly in terms of specificity. 83 The IJV narrowing or occlusion assessed by MRV in supine position does not need to be considered as pathologic at all since these findings are not reproducible in the upright position using positional MRV. 84 In addition, advanced MRI techniques such as phase-contrast flow studies and magnetic resonance perfusion are well suited to investigate whether venous outflow changes in terms of ‘CCSVI’ do have any impact on intracranial venous blood flow. As mentioned above, a combined MRV and phase-contrast flow study did not show any intracranial reflux in MS patients and healthy controls with or without venous abnormalities on MRV. 79 Another study found flow changes in MS patients with and without venous narrowing in the extracranial venous systems. 85 However, it remains questionable whether these changes are relevant since the intracranial part has to be considered as the crucial part in terms of venous backflow and pressure.
Recent studies using high-field MRI and susceptibility-weighted imaging have nicely shown the perivascular inflammation pattern in MS by sensitively visualizing the small venous vessels in the periventricular and deep white matter. 86 It has been conclusively showed that MS patients show a reduced visibility of cerebral veins. This finding seems to be inversely correlated with the periventricular and whole-brain T2-lesion load suggestive of chronic inflammatory changes including gliosis and fibrinoid deposition.87,88 One single study found a link between the decreased visibility of venous vessels and venous outflow changes suggestive of CCSVI. 89 However, based on the CCSVI theory, we would expect the opposite since venous obstruction would rather lead to an increased diameter and visibility of cerebral veins. The findings on cerebral veins are also reflected by low magnetic resonance perfusion measures (cerebral venous blood flow and cerebral venous blood volume) and other measures suggesting an underutilization of oxygen in MS brain tissue.90,91 Magnetic resonance perfusion examinations (dynamic susceptibility contrast-enhanced) in MS patients and control subjects with or without fulfilling ‘CCSVI’ criteria did not show any substantial relationship between MS and ‘CCSVI’ in terms of cerebral perfusion parameters. Moreover, no relationship between perfusion parameters in ‘CCSVI’ subjects and clinical outcome measures could be observed. 90 This once again underscores the implausibility of the ‘CCSVI’ concept in terms of pathophysiology.
Selective Venography
There is currently limited data on selective catheter venography addressing the issue of venous abnormalities/anomalies in MS patients. In accordance to the above-mentioned MRV study, a study using selective venography on 42 MS patients with different disease courses and disease duration showed that the occurrence of venous anomalies might be depending on the age and disease duration. A low prevalence was observed in early disease courses such as clinically isolated syndrome and early RR-MS (24%). Only one of the included clinically isolated syndrome patients showed an extracranial venous stenosis. In contrast, the prevalence increases substantially in patients with longer disease durations of >10 years (92%). 92
TREATMENT STUDIES
Notwithstanding the questionable scientific basis, many patients with MS decide not to wait until the scientific dispute has come to an end and have percutaneous transluminal angioplasty (PTA; ‘liberation treatment’) performed. Some of them report the results of their treatment in social media, sometimes in structured databases (e.g., http://www.ccsvi-tracking.com). Even respected MS clinics have opened a registry, which obviously will never answer the question whether the treatment is effective or not (e.g., British Columbia CCSVI Registry).
There is still discussion whether the current state of knowledge justifies the allocation of money and other resources to trials of PTA in patients with MS and whether those trials are ethical.93,94 Nevertheless, some institutes are planning trials and others are already recruiting patients (http://clinicaltrials.gov/ct2/results?term=ccsvi).
EFFICACY OF PERCUTANEOUS TRANSLUMINAL ANGIOPLASTY FOR MULTIPLE SCLEROSIS/‘CHRONIC CEREBROSPINAL VENOUS INSUFFICIENCY’
So far, a few reports on open-label treatment results have been published, the first in 2009. In this open-label study, patients with RR (n = 35), secondary progressive (n = 20) and primary progressive (n = 10) MS were treated with PTA. 9 In RR patients, the annualized relapse rate did not change after PTA (0.9 versus 0.7), but the number of relapse-free patients (27% versus 50%), gadolinium-enhancing MRI scans (50% versus 12%), and scales of disability and quality of life (MSFC and Multiple Sclerosis Quality of Life) improved. There is no mention of the results of MRI studies in patients with progressive MS. It is not clear whether all 65 treated patients contribute to the 18-month follow-up (only percentages of patients who reach a certain end point are given, no absolute numbers). Quality of life scales improved in primary progressive but not in secondary progressive patients, the MSFC did not change in either group. In the RR group, 33 of 35 patients were on immunomodulatory or immunosuppressive treatment, with only limited data on treatment available. 95
In a later publication, Zamboni et al 35 try to address some of the concerns mentioned above. 96 This is a case control study of 15 patients with RR-MS followed for 12 months. Eight patients received immediate PTA and seven patients with a delay of 6 months. All patients were on immunomodulatory medication. Unblinded clinical data show one relapse in the immediate treatment group and four in the delayed group. Whether the four relapses in the delayed treatment group occurred before or after treatment is not clear. No Expanded Disability Status Scale 97 changes were seen, but the MSFC had improved in both treatment groups after 6 and 12 months. Regarding the blindly assessed MRI data, the 8 patients in the immediate treatment group accumulated 12 new T2 lesions (an average of 1.5 per patient) compared with 5 new T2 lesions in the 6 remaining patients (an average of 0.83 per patient; one dropout because of ‘familial reason’) in the delayed treatment group after 6 months; after 12 months (end of study), the immediate treatment group had accumulated 34 new T2 lesions (an average of 4.5 per patient) compared with 12 new T2 lesions in the delayed treatment group (an average of 2.0 per patient). The delayed treatment group accumulated more new lesions in the 6 months after PTA than in the six preceding PTA (7 versus 5). Although delayed treatment patients accumulated fewer lesions, the authors report a far higher median change in T2 lesion volume after 6 and 12 months in this group compared with the immediate treatment group. This seems to be a contradiction, but this is not discussed in the publication. Striking reductions in T1 hypointense lesion volumes were seen in all groups and are not discussed or explained. In the abstract, the authors present data that appear to support their hypothesis, leaving out data indicating the opposite. Data in the abstract can be found in the main text, but differ from those provided in the main table. There are calculation errors and inconsistencies between text and tables.
Malagoni et al 98 studied the effect of open-label PTA on measures of fatigue in 31 patients with MS. Five patients did not complete the study. They found statistically significant and clinically relevant improvements on the Modified Fatigue Impact Scale 99 and the Fatigue Severity Scale 100 after 1, 6, and 12 months, with a tendency to decline in the year after treatment. In addition, the 6-minute walking distance improved 1 month after treatment, but the authors do not report the results after 6 and 12 months. The authors concluded that PTA treatment was effective.
Kipshidze reports treatment of 4 MS patients with PTA, and concludes that this treatment is effective, but does not provide the underlying data. 101
Kostecki presents 6 month follow-up data on 36 MS patients treated by PTA. 102 Quality of life scales such as the Multiple Sclerosis Impact Scale (MSIS-29) 103 improved temporarily at month 3, whereas the Heat Intolerance scale and Fatigue Severity Scale were still improved at the end of follow-up. The Expanded Disability Status Scale did not respond to the treatment, so that the authors concluded that the treatment ‘did not have an influence on the patient's neurologic condition; however, in the midterm follow-up, an improvement in some quality-of-life parameters was observed’ .
A somewhat larger open-label study assessed the results of PTA in 94 patients with MS after 6 months with MSIS-29, Fatigue Severity Scale, and Epworth sleepiness scale 104 questionnaires and found improvements. No MRI studies were reported. 105
In 2012, Salvi 106 reported a 2-year open-label follow-up of 29 PTA-treated patients, 17 of whom were from the cohort of 65 patients originally reported by Zamboni. 9 These patients were seen every 3 months, both in the 2 years preceding PTA and in the 2 years after treatment. The mean exacerbation frequency in the follow-up years was 0.45 as compared with 0.76 in pretreatment years. The mean Expanded Disability Status Scale was lower after 2 years compared with pretreatment: 1.98 versus 2.3.
Recently, Hubbard et al 107 treated 259 self-referred patients who ‘reported an MS diagnosis from their local neurologist’ in an open-label study. The patients paid for all diagnostic and therapeutic procedures. After informed consent was signed, MRV and selective venography were performed, followed by balloon venoplasty. Apparently, 100% of patients who signed informed consent were found to have stenoses, since all 259 patients were treated. Main outcome measures were MSIS-29 scores after 1 and 6 months. The percentage of questionnaires completed after 1 and 6 months was 73.4 and 70.7, respectively. On the MSIS-29 physical scale, a percentage of 67.9 were improved, 25.8 were unchanged, and 6.3 were worse after 1 month; the percentages were 53.6, 35.5, and 10.9 after 6 months. On the MSIS-29 psychological scale, a percentage of 53.0 were improved, 42.2 were unchanged, and 4.9 were worse after 1 month; the percentages were 44.0, 51.1, and 4.5 after 6 months. Although the authors claim ‘significant clinical improvement’, it appears that the conclusion is not supported by their data. The authors seem to be satisfied with an unverified diagnosis of MS. After signing of informed consent, all 259 patients appeared to have stenoses on selective venography and were found to need treatment. Although similar figures were reported by the cooperating groups of Zamboni and Zivadinov,8,108 others found significantly lower percentages,28,29,92 while reliable data in healthy control groups are lacking. There are no objective outcome measures such as blinded neurologic examination or MRI scans. The primary outcome measure is the subjective MSIS-29 questionnaire. Placebo effects are very likely to occur in any open-label setting. In this specific study, most of the patients were self-referred and paid the costs for the treatment. This will likely have biased the results toward reporting beneficial effects.
In June 2012, preliminary data were presented at a press conference regarding a single blind, nonrandomized study of 30 MS patients who were treated by PTA and 10 untreated control patients with 12-month follow-up. The study was funded by the government of Newfoundland and Labrador (Canada). There was no objective evidence of improvement as measured by neurologic examination and MRI. The unblinded patients reported improvements in physical and psychological well-being in the first 3 months after procedure. By now, there has been no peer reviewed publication of these data (Newfoundland Labrador Multiple Sclerosis Observational Study).
Two recent studies including 45 and 462 patients found no support for a beneficial effect of PTA, although the retrospective design does not permit us to draw any firm conclusions on the basis of these two studies alone.109,110
In summary, all studies discussed in this section experience methodological flaws. They are all of an open-label design and in majority make use of subjective outcome measures. The Newfoundland study appears to have the best methodological design so far, but has not been published. We have to conclude that there is still no evidence at all to support the notion that balloon venoplasty is effective in the treatment of MS. Placebo-controlled trials are now underway. To avoid ongoing uncertainty in the future, it will be extremely important that their design will meet the same quality standards that are required nowadays of potential drug treatments of MS.
SAFETY OF PERCUTANEOUS TRANSLUMINAL ANGIOPLASTY FOR MS/‘CHRONIC CEREBROSPINAL VENOUS INSUFFICIENCY’
Three studies looking at the safety of PTA in ‘CCSVI’ have been reported so far. These data originate from clinics that offer PTA for ‘CCSVI’ to patients willing to pay for this treatment with unproven efficacy.
The largest study is that of Petrov et al 111 who report groin hematomas (1%), cardiac arrhythmias (1.2%), vein rupture (0.4%), vein dissection (3%), and thrombosis (1.6%) in a retrospective cohort of 461 patients (stent placement in 16%) with MS.
Another group reported its experience with PTA (requiring stent placement in ~44%) of 331 patients with ‘CCSVI’ . 34 They found groin hematomas (1.2%), cardiac arrhythmias (0.6%), stent thrombosis (1.2%), technical problems with stents and balloons (2.7%), gastrointestinal bleeding (0.3%), and had to surgically remove one angioplasty balloon (0.3%). It is not mentioned whether this was a prospective or retrospectively examined cohort.
A third group reported a retrospectively observed cohort of 240 patients who had PTA (stent placement in 11%) for ‘CCSVI’, and had groin hematomas (0.8%), cardiac arrhythmias (1.2%), vein thrombosis or dissection (10.1%), transient and persistent headaches (8.2% and 0.4%), transient neck pain (15.2%), and allergic reactions to contrast agent (2.7%). More severe side effects were thrombosis of the IJV (1.2%) and stress-induced cardiomyopathy (‘takotsubo’) requiring intensive care admission. 112
Over the past 2 years there have been several case reports concerning patients who had serious side effects after PTA for ‘CCSVI’ . These include IJV thrombosis requiring open thrombectomy; 113 stent thrombosis and aneurysmal vein dilatation, compression neuropathy of cranial nerves XI and XII, stent migration to a renal vein, persistent extraperitoneal abdominal hematoma, and stent thrombosis possibly extending from the left IJV into the sigmoid sinus and transverse sinus. 114
There are reports of one patient who died of (complications of) PTA for ‘CCSVI’ 115 and media reports of three other MS patients who allegedly died after PTA, but there are no medical publications available (e.g., Details emerge about man who died after MS therapy | CTV News).
In summary, it appears that most patients do not encounter serious side effects of PTA for ‘CCSVI’ . However, side effects do occur, sometimes with serious consequences, and at least one patient, and possibly more, died of the procedure.
Side effects, even lethal, might be acceptable in MS if there is documented aggressive disease that does not react to first-line treatments, such as interferon-beta and glatiramer acetate, 116 and there is a second-line treatment with an established and sufficiently large beneficial effect, as is the case with natalizumab.117–119
In the case of PTA for ‘CCSVI’, there is no evidence for efficacy at all, so that doctors treating MS patients with PTA accept a heavy responsibility for any side effects that will occur, possibly with the exception of patients treated in the setting of well-designed clinical trials.
PATHOPHYSIOLOGIC CONSIDERATIONS
The pathophysiologic concept of CCVSI in MS is based on the assumption that impaired venous outflow with reflux and venous congestion, which leads to perivascular diapedesis of blood cells inducing perivascular inflammation and pathologic iron accumulation associated with an acceleration of neurodegenerative pathology. 120 At first glance, this theory might be logical since perivascular (perivenous) inflammation and neurodegeneration including increased iron deposition in the basal ganglia are important features of MS pathology. However, this proposed pathophysiologic concept of ‘CCSVI’ in MS completely disregards the complexity and heterogeneity of MS pathophysiology as well as epidemiologic and environmental features.121–123
It is completely unclear how to link ‘CCSVI’ to several hallmarks of MS pathophysiology such as a B-cell and T-cell mediated autoimmune response and subsequent neuronal and axonal damage.124–128 In addition, ‘CCSVI’ cannot explain the MS lesion heterogeneity of white and gray matter that show different histopathologic characteristics.129,130 ‘CCSVI’ mainly refers to perivascular inflammation but lacks any explanation of diffuse demyelination in the white and gray matter (white and gray matter pathology). Increased and accelerated iron deposition is an unspecific neurodegenerative marker not exclusively being present in MS but also in many other neurodegenerative disorders such as Alzheimer's dementia, and probably also in the normal aging brain. 131 In addition, based on the CCSVI theory, it could be expected that increased iron deposition can be detected also diffusely in the white matter which has not been described so far.
Venous outflow impairment has not been associated with primary neurodegenerative diseases so far. If ‘CCSVI’ is associated with MS pathology, then we have to consider patients with real pathologic venous outflow. Chronic venous outflow changes like those in postoperative situation in head and neck cancer patients (neck dissection) or in patients with sinus-venous thrombosis or other diseases with an increased central venous pressure have not been linked to MS pathology so far.20,132,133 In other words, higher incidence of MS in these patient groups has not been reported so far. In addition, venous outflow impairment of the central nervous system should lead to an increased intracranial pressure. However, an increased intracranial pressure has not been reported to be frequent in MS patients. If the ‘CCSVI’ theory was plausible, then one would also expect impairment of the drainage in the retinal and ophthalmic venous systems that drain into the IJVs. However, this is obviously not the case, 134 and while retinal nerve fiber layer atrophy as detected by optical coherence tomography is a well-acknowledged feature of MS, 135 no evidence for impaired venous outflow from retinal veins has been reported in thousands of MS patients who have been investigated by this technique despite the excellent visibility of the retinal vessels with modern spectral domain optical coherence tomography technology.136,137
Besides this implausibility of the ‘CCSVI’ theory in terms of pathophysiology, also other important factors that are strongly associated with MS call the ‘CCSVI’ concept into question. Genetic susceptibility factors of MS like the major histocompatibility complex and non major histocompatibility complex loci have not been linked to venous pathology.25,138 Local differences in MS prevalence in terms of geographic distribution should consequently also be associated with different prevalence of venous outflow impairment. However, this has not been reported so far. Multiple sclerosis is more frequent in younger patients and in women.139,140 Arterial and venous vessel pathologies are more likely to occur in older patients and in male patients. In addition, Vitamin D deficiency and Epstein-Barr virus infections, important environmental factors associated with MS, are not likely to be associated with venous outflow pathology.141–144
In conclusion, there is no single convincing pathophysiologic or epidemiologic argument supporting the concept that chronic venous outflow changes in terms of ‘CCSVI’ are associated with MS pathology or higher MS incidence and prevalence.
CONCLUSION
In line with other recent reviews on this topic,79,145 this review article conclusively stresses that the serious methodological limits and misinterpretation of findings should be reason enough to halt the completely unsubstantiated ‘CCSVI’ -based interventional therapy for MS patients. Calling for controlled studies misses the point, because this suggests that the interventional therapies should be continued (possibly over many years) until definitive results are available. The interventions are expensive, thousands of Euros, causing a significant financial burden but more important impose a concrete health risk onto our MS patients. Only a complete halt to the therapy seems sensible.
DISCLOSURE/CONFLICT OF INTEREST
The authors declare no conflict of interest.