
Abstract
Cerebral stroke continues to be a major cause of death and the leading cause of long-term disability in developed countries. Evidence reviewed here suggests that gender influences various aspects of the clinical spectrum of ischemic stroke, in terms of influencing how a patients present with ischemic stroke through to how they respond to treatment. In addition, this review focuses on discussing the various pathologic mechanisms of ischemic stroke that may differ according to gender and compares how intrinsic and hormonal mechanisms may account for such gender differences. All clinical trials to date investigating putative neuroprotective treatments for ischemic stroke have failed, and it may be that our understanding of the injury cascade initiated after ischemic injury is incomplete. Revealing aspects of the pathophysiological consequences of ischemic stroke that are gender specific may enable gender relevant and effective neuroprotective strategies to be identified. Thus, it is possible to conclude that gender does, in fact, have an important role in ischemic stroke and must be factored into experimental and clinical investigations of ischemic stroke.
INTRODUCTION
Cerebral stroke is a leading cause of death and the main cause of adult long-term disability in developed countries. The majority (~ 85%) of cerebral strokes are ischemic in nature and result from the occlusion of a major cerebral artery by a thrombus or an embolism, which leads to loss of blood flow and subsequent tissue death in the affected region. There is an increasing recognition of differences between men and women in relation to stroke, not only in terms of stroke risk but also in terms of influencing the etiology, symptoms, and outcomes. Women appear to have a higher overall lifetime risk of stroke in addition to higher rates of poststroke mortality, disability, depression, and dementia, compared with men. Such gender differences have largely been attributed to the longer life expectancy of women, consistent with the fact that age is the strongest independent risk factor for stroke 1 and also a negative predictor for clinical outcome. 2 Such a detrimental impact of age upon stroke risk and outcome, initially observed in white populations, has been consistently reported across studies involving participants of varying race and ethnicity. 3
In the general population, men have been found to experience more ischemic strokes4–6 whereas women tend to have more infarctions involving the anterior circulation and experience more subarachnoid hemorrhages.5,7 In terms of stroke onset, women tend to be, on average, approximately 4 years older than men at the age of ischemic stroke onset. A recent meta-analysis on data from 2,566 patients revealed that the mean age of onset of first ischemic stroke was 66.6 years in men compared with 70.0 years in women. 8 As age is a significant risk factor and predictor of outcome after ischemic stroke, it is reported that elderly women carry the major burden associated with ischemic stroke. 9 However, it is reported that in the premenopausal years, women benefit from a native cerebrovascular protection provided by reproductive hormones. For example, The Framingham study reported that the incidence of ischemic stroke is lower in women than men within the 45- to 54-year-old age cohort, composed mainly of premenopausal and preimenopausal women, but is equalized in the 55- to 64-year-old cohort. 10 However, non-hormonal factors also contribute to the sexual dimorphic risk of ischemic stroke as gender differences not only extend well beyond the menopausal years but are also clearly present in neonatal and childhood populations where circulating hormones are equivalent between the sexes.11,12 Interestingly, although some studies do report a higher incidence of stroke recurrence in females compared with males 13 it seems that actually, after comparing for age, medical history, and other relevant risk factors, no gender differences are observed in stroke recurrence. 14
Gender may also influence both the mechanisms of injury and outcome after ischemic stroke and thus, gender should be considered in both experimental and clinical stroke studies. There is an urgent need for the development of effective pharmacological therapies to counter the deleterious effects of ischemic stroke. The only current treatment available is thrombolysis with tissue plasminogen activator, but because of its narrow therapeutic window (<4.5 hours) and safety concerns, less than 5% of stroke patients receive tissue plasminogen activator and the majority of stroke patients only receive supportive care. 15 The development of safe and effective treatments is, therefore, a major challenge to experimental and clinical stroke research. This review discusses the various aspects of ischemic stroke (risk, symptoms, outcome, etc.), which are beginning to emerge as being sexually dimorphic. In addition, it is discussed how knowledge of the influence of gender on the pathologic mechanisms after ischemic stroke may reveal potential treatment targets.
GENDER INFLUENCES THE CLINICAL CHARACTERISTICS ASSOCIATED WITH ISCHEMIC STROKE
Important modifiable risk factors for ischemic stroke include hypertension, high blood cholesterol, diabetes, cigarette smoking, obesity, and lack of physical activity.16–19 Data on sex-specific risk factors in ischemic stroke have initially revealed that men report a higher prevalence of current smoking, history of smoking, coronary artery disease, and peripheral artery disease.20–22 Such variations in risk factors, according to gender, were also confirmed by others 23 who reported that although women diagnosed with ischemic stroke were older than men, the history of hyperlipidemia, smoking, and coronary heart disease were less frequent. However, a systematic review and meta-analysis revealed that women with stroke are more likely than men to have a parental history of stroke, which is accounted for by an excess maternal history of stroke. 24 Such a finding could be explained by sex-specific genetic, epigenetic, or non-genetic mechanisms.
It is also important to consider whether gender differences occur in the clinical presentation of a patient experiencing an ischemic stroke, as this may impact upon the prompt recognition, diagnostic testing, and receipt of appropriate treatment. In general terms, the symptoms of ischemic stroke can be separated into classic symptoms, which include hemibody numbness, hemiparesis, aphasia, dysarthria, visual disturbance, diplopia, facial weakness, discoordination/ataxia, and vertigo, and non-specific to stroke symptoms including pain, light headedness, mental status change, headache, and other neurologic or non-neurologic symptoms. Data on gender differences in acute stroke presentation are somewhat limited and few population-based studies exist. However, some studies report that women present with more non-specific stroke symptoms such as pain or altered mental status8,25–27 whereas others report that women are as likely as men to report weakness and clumsiness, as well as both classic and non-specific symptoms that include pain, disorientation, and altered consciousness. 28 In one of the few population-based studies, men were found to be more likely to present with classic focal neurologic symptoms such as sensory abnormalities, ataxia, and diplopia whereas women tended to present with diffuse symptoms such as disorientation, generalized weakness, fatigue, and mental status change. 29 However, it is reported that women delay up to three times longer than men in seeking care for stroke symptoms, 30 which of course may contribute to variations in the presentation of symptoms.
If women do clinically present differently with ischemic stroke than men, then there may be significant public health implications. Recognition of potential gender differences in stroke symptoms through education aimed at both the public and health care professionals could result in decreased out-of-hospital and in-hospital delays, thus increasing access to acute stroke therapy in women. Many public health campaigns, for example ‘Give me 5’in the United States and ‘FAST’ in the United Kingdom, are aimed primarily at targeting the classic symptoms of ischemic stroke. 31 It may be that public health campaigns and stroke intervention efforts should be modified to address the possibility that women, experiencing an ischemic stroke, may experience a number of non-specific symptoms. However, in the first instance, data from a large multicenter trial could determine whether gender differences in presentation of symptoms occur across a representative population of stroke cases and importantly, whether differences in symptom presentation have any clinical consequences.
GENDER EFFECTS ON OUTCOME AFTER ISCHEMIC STROKE
Numerous studies report gender differences in both mortality and morbidity after ischemic stroke. Typically, female stroke patients present at an older age than male stroke patients thus, older female patients are likely to comprise the majority of stroke-related mortality and disability.3,32 Data on gender differences in mortality rates after ischemic stroke are conflicting with some reporting higher in-hospital mortality rates in women, 33 whereas others report no gender differences in mortality rates both in-hospital 5 and at 3 months after ischemic stroke. 4
However, the general consensus seems to be that women have poorer functional outcomes, than men, after ischemic stroke.5,33,34 Such a gender difference appears to be sustained even after making adjustments for age and other sex differences in medical history and presentation. In fact, one study 34 found that at 6 months poststroke, female sex is still an independent predictor of poor prognosis even when adjusting for other predictors of functional outcome. Others have reported that at 3 months poststroke, women are more likely to have a poorer functional outcome 4 and, in addition, women show significantly worse locomotor function than men at both 1- and 5-year-follow-up after ischemic stroke. 14 After ischemic stroke, women are less likely to be discharged home 35 and more likely to have impairments and activity limitations on followup. 5 It is reported that poststroke women experience more mental impairment, 35 depression, 36 fatigue, 37 and have a lower overall quality of life38–40 than men. It may be though that if women are more likely to delay in seeking care for stroke symptoms, 30 this could result in treatment delays, which would contribute to worse outcomes. However, it needs also to be considered whether gender influences the treatment a patient receives both during and after the diagnosis of ischemic stroke.
GENDER EFFECTS ON THE TREATMENT RECEIVED AND RESPONSE TO TREATMENT
During diagnosis of ischemic stroke, several studies report gender differences in the use of echocardiography, carotid imaging, and endarterectomy.2,41,42 In addition, data from different national registers indicate that women are less likely to be seen by a stroke team or have their lipids investigated.5,43 In terms of in-hospital treatment, the use of antiplatelet drugs and statins is reported to be lower among women than men and some report that women are less likely to receive thrombolytic treatment.6,43 However, it must be noted that any differences in treatment may be as a direct consequence of sex differences in symptoms at presentation.
In addition to influencing the treatment a patient may actually receive, gender probably also influences the response to certain pharmacological treatments. Such a notion is largely overlooked in experimental stroke studies (discussed below) and only a few clinical trials to date have specifically investigated whether sex-specific responses to treatment exist. The Physicians Health Study found that aspirin substantially reduced the risk of cardiovascular disease, but not stroke, in men. 44 By contrast, in the Women’s Health Study, aspirin reduced the risk of stroke by 24% but had no effect on cardiovascular disease in women.45,46 A subsequent sex-specific meta-analysis confirmed the differential effects of aspirin in men and women with respect to stroke and coronary artery disease risk. 44 Oral anticoagulation with warfarin also seems to be affected by gender as shown in a prospective study of atrial fibrillation patients. 47 In that study, men and women were anticoagulated to equal degrees but anticoagulated women had a relative risk of 2.0 for ischemic stroke versus anticoagulated men, even after age correction. Biologic sex may also affect the response to thrombolytic therapy as, after stroke, women have worse functional outcomes compared with men yet several studies have demonstrated an absence of sex differences in functional outcome after acute thrombolytic therapy.48–50 This normalization of baseline differences in functional outcome suggests that women may experience a greater benefit from tissue plasminogen activator than men. 49 Thus, gender differences do seem to exist across many clinical aspects of ischemic stroke from affecting how the patient may present in the clinic through to how they may respond to a treatment. Although the current American Heart Association/American Stroke Association guidelines for acute stroke treatment 51 make no distinction between genders in terms of presentation of symptoms or possible therapeutic approaches. However, the influence of gender is often overlooked in the design of experimental stroke studies and the investigation of the pathologic mechanisms influenced by gender may inform the design of potential treatment strategies.
THE IMPACT OF GENDER—INTRINSIC VERSUS HORMONAL MECHANISMS
Although it would appear that many aspects of ischemic stroke are sexually dimorphic, it is relevant to consider the reasons behind such dimorphism. Differences according to biologic sex may be due to intrinsic factors, i.e., the sex chromosomes, which are consistent throughout the lifespan, or caused by sex steroid hormones, which vary between the genders and fluctuate at various stages of the lifespan. The influence of biologic sex has both organizational, i.e., occurs at a particular period, for example during development, and persists even after the hormonal exposure is removed, and activational effects, which are reversible and persist only while the influencing sex steroid hormone is present. As discussed below, gender differences in the outcome after ischemic stroke can be explained by both hormone-independent and hormone-dependent mechanisms (reviewed also elsewhere52,53).
INTRINSIC MECHANISMS
Aside from adult males experiencing a higher incidence of ischemic stroke, this ‘male sensitivity’ to ischemic stroke can also be observed in childhood populations (for example, see references 11,12). As levels of steroid hormones are low in childhood populations, this suggests that other factors, i.e,. non-hormonal, have a role in mediating this sensitivity to ischemic stroke in males. Emerging evidence suggests that the sexually dimorphic response seen to ischemic stroke is partly due to the genetic complement of cells. Sex-specific cultures, in terms of both hippocampal neurons54,55 and astrocytes56,57 have shown that male-derived cells are more sensitive to ischemic injury than female-derived cells. Such cells are derived from neonatal populations and cultured in the absence of hormonal influences thus, confirming that intrinsic cell differences exist between males and females. In addition, several molecular mechanisms of injury, not linked to sexual development or function, have been shown to act dimorphically under ischemic conditions including nitric oxide synthase, 58 poly-ADP ribose polymerase (PARP), 59 and caspases.60,61 However, the role of sex-specific hormones must also be considered, as revealing their role in determining the effects of ischemic stroke has also identified potential neuroprotective candidates for ischemic stroke treatment.
BIOLOGIC MECHANISMS
Experimental studies, using both
SOCIOCULTURAL FACTORS
In recent years, a considerable amount of attention has been focused on the importance of considering social and cultural factors when considering differences in stroke epidemiology. For example, although it is often stated that men are at overall higher risk of ischemic stroke than females, a recent meta-analysis reported that there was a significantly larger male predominance in studies from Australasia and the Americas compared with studies from Europe. 29 However, that same review highlighted the fact that the distribution of contributing studies to such meta-analyses is uneven with regions such as Africa, Asia, and South America being underrepresented. Racial and ethnic disparities in stroke incidence and outcome are well documented with, for example, age-adjusted stroke hospitalization rates for blacks being over three times higher than for whites. 73 In terms of social factors, a number of studies have shown that the incidence of ischemic stroke increases with lower socioeconomic status in both men and women.74,75 Although, interestingly, adjustment for a variety of classic lifestyle and psychosocial risk factors did not alter the impact of socioeconomic status on stroke risk in men whereas some attenuation of socioeconomic differential was seen after adjustment for risk factors in women. 76
MECHANISMS OF INJURY MAY DIFFER ACCORDING TO GENDER
Cerebral ischemia triggers a cascade of pathologic events including excitotoxicity, cell necrosis, apoptosis, inflammation, blood–brain barrier breakdown etc., which ultimately culminate in cellular dysfunction and death. Although much progress has been made in dissecting the molecular pathways of pathologic processes such as excitotoxicity, oxidative stress, inflammation, and apoptosis after ischemic stroke, this has largely failed to translate into effective therapies. However, emerging evidence suggests that gender differences occur in certain aspects of the pathologic cascade, induced after cerebral ischemia, including molecular pathways activated, which culminate in cell death and various aspects of the peripheral and brain inflammatory response (reviewed elsewhere 77 ) although gender (and age) are largely overlooked in the design of experimental studies.
Ischemic cell death is triggered by an influx of calcium, with subsequent oxidative damage and mitochondrial dysfunction activating several distinct cell death pathways. 78 The immediate energy failure seen in the ischemic core leads to swelling of the mitochondria and loss of membrane integrity, typical of necrotic cell death. Reducing necrotic cell death is extremely difficult and likely requires reperfusion during the ischemic insult. However, a delayed apoptotic cell death also occurs in the penumbral region of the ischemic brain. Over the past decade, both caspase-dependent and caspase-independent cell-death pathways have been recognized, adding considerable complexity to studies of ischemic cell death. 79 Although cell death and apoptosis occur after ischemic injury, it is relevant to consider that the mechanism of injury between the genders could differ. Previous studies have shown that ischemic cell death pathways are different in the male and female brains, females often showing caspase-mediated cell death of individual neurons, whereas males are more sensitive to caspase-independent cell death. 77
Apoptotic pathology involves at least two signaling cascades, one initiated through intrinsic, mitochondria-mediated mechanisms involving cytochrome C release, apoptosome assembly, and caspase cleavage, and hence is known as a ‘caspase-dependent’ pathway. An alternative caspase-independent pathway is triggered by postischemic DNA damage and involves the activation of PARP, release of apoptosis-inducing factor (AIF) from the mitochondria, and translocation of AIF to the nucleus to induce chromatin condensation and large scale DNA fragmentation. Both pathways of apoptosis involve multiple molecular signals, and there are numerous examples of such molecules that have sexually dimorphic roles in cerebral ischemic injury (see Table 1) including; AIF, 80 caspase 3,60,80 PARP, 55 nitric oxide synthase, 81 glutathione, 82 Akt, 83 astrocytic aromatase, 57 glial fibrillary acidic protein, 84 angiotensin II type 2 receptor, 85 and the P450 enzyme, soluble epoxide hydrolase. 86
Molecular components of cell death pathways, which are proposed to show sexually dimorphic patterns of expression and/or function
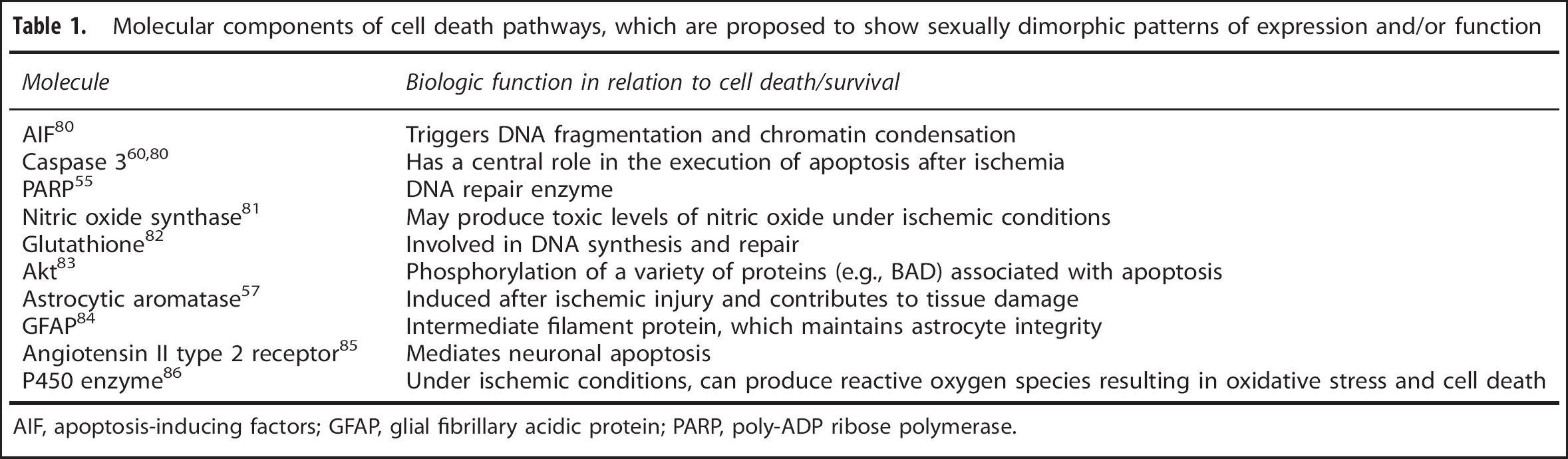
AIF, apoptosis-inducing factors; GFAP, glial fibrillary acidic protein; PARP, poly-ADP ribose polymerase.
The DNA repair enzyme PARP-1 induces caspase-independent apoptotic cell death via neuronal nitric oxide synthase (nNOS), PARP-1, and AIF, which all appear to have a key role in regulating cell death in the male brain. For example, although neuronal nitric oxide synthase deletion and inhibition results in neuroprotection in adult male mice, such genetic and pharmacological manipulations of neuronal nitric oxide synthase activity actually exacerbate stroke damage in adult female mice.
58
Such a sexually dimorphic response is not affected by hormone exposure and/or replacement suggesting it is either hormone-independent (a sex-specific effect) or secondary to organizational or epigenetic factors induced by early gonadal steroid exposure. In addition,
A novel cell-death pathway, autophagy, has also been recently implicated in the pathology occurring after ischemic stroke and appears to differ according to gender. Autophagy involves engulfing segments of the cell’s cytoplasm into an autophagosome destined for degradation by the lysosome allowing for recycling of cellular contents. 89 Autophagic cell death occurs after neonatal hypoxic injury in male animals as shown by increases in autophagosome formation and lysosome activity. Inhibitors of autophagy are protective in models of neonatal hypoxic injury but seem to preferentially protect male-derived neuronal populations rather than female-derived ones. 90
It is widely accepted that inflammation has a key role in contributing to the ensuing damage after ischemic stroke. It has been reported that young female rodents exhibit a decreased inflammatory response to ischemic injury compared with males and a considerable body of evidence strongly implicates estrogens as a significant regulator of inflammatory pathways.4,91
Gene expression changes in the blood are a reflection of the immune response and a consequence of both environmental and genetic factors. Interestingly, Tian et
In terms of the pathology produced after cerebral ischemia, attention has traditionally focused on damage to the gray matter, although cerebral white matter is highly vulnerable to the effects of focal ischemia.
95
Pathologic changes in oligodendrocytes and myelinated axons occur early after the onset of ischemia and seems to be concomitant with, but independent of, neuronal perikaryal injury.
96
It is relevant to consider how white matter function may alter, according to gender, after ischemic injury. Although reports of sexual dimorphism in white matter have been reported, these have largely been restricted to gross anatomic differences and numbers of myelinated axons. Previous studies have reported that significant differences occur in the development of white matter between the genders.
97
In the mature nervous system, the average axonal diameter is larger and myelin sheaths are thicker in males than in females.
98
However, a study by Cerghet
HORMONES AND CEREBRAL ISCHEMIA
Numerous experimental studies have identified the contribution of hormonal influences on the outcome after ischemic stroke. For example, ovariectomized female mice have increased stroke volume compared with females with intact ovarian function. 63
Such observations have led researchers to investigate the potential protective role of steroid hormones as a candidate treatment after ischemic stroke. In experimental studies, treatment with estrogens is neuroprotective in most animal models, and estrogen reduces infarct size when acutely administered to males, ovariectomized females, and reproductively senescent females (reviewed elsewhere100,101). Although estrogen confers protection in experimental stroke, clinical translation of estrogen’s protective effect has been unsuccessful to date. 102
Along with estrogens, progesterone levels also dramatically reduce after the menopause and thus, may contribute to the endogenous cardiovascular protection women experience during their premenopausal years. A large number of experimental studies (reviewed elsewhere 70 ) have investigated the neuroprotective potential of progesterone after cerebral ischemia. The majority of these studies have reported a positive effect of progesterone treatment after ischemic stroke and this appears to be consistent across numerous studies including both rats and mice, animals of both genders, and using both transient and permanent models of ischemia. Although as highlighted in a recent systematic review, 103 further studies assessing the effectiveness of progesterone need to examine dose responses, time window of treatment effects, longer-term outcomes, and effects of gender and hormonal status of animals used.
Because of increased incidence of stroke in males, and worse outcome in male animals after experimental stroke, it has been suggested that androgens may be detrimental to the consequence of ischemic stroke. Recent investigations have focused on the role of testosterone in this male ischemic sensitivity largely because of the clinical observation that elevated endogenous testosterone levels correlate with increased stroke risk in young boys but not in young girls.
104
However, in adults it seems that low circulating testosterone levels are associated with increased stroke incidence and worse outcomes after stroke in men.105,106 In animals, low doses of testosterone administered to castrated animals decreases the amount of infarcted tissue after ischemic stroke, whereas infarct damage is exacerbated with higher doses of testosterone.
107
The androgen receptor antagonist, flutamide, blocked these effects, suggesting a key role of the androgen receptor mediating the ischemic response to testosterone.
108
Such results suggest that while testosterone may contribute to the ‘ischemia-sensitive’ phenotype seen in males such effects are both complex and dose dependent
It is now well established that tissues and organs outside of the reproductive system, i.e., the brain, can also synthesize steroid hormones and this extragonadal production of hormones may also influence stroke sensitivity. In female animals, the absence of aromatase, which converts androgens to estrogens, results in increased infarction area after ischemic stroke.
108
CEREBRAL ISCHEMIC STROKE—THE IMPORTANCE OF AGE AND GENDER
The total incidence of stroke is projected to rise substantially over the next 20 years, because of the rising age of the population. Age is the most important independent risk factor with stroke rates doubling every decade after the age of 55. 1 In addition, age is a significant predictor of outcome independent of stroke severity, etiology, efficacy of thrombolysis, gender, and other vascular risk factors. 110 In terms of outcome, older patients tend to have higher in-hospital mortality rates as well as poorer functional outcomes. Despite the importance of age and the knowledge that stroke is sexually dimorphic, experimental studies are largely conducted in healthy, young adult males thus, overlooking the impact of both age and gender. However, it appears that in experimental studies, the impact of both age and gender are not straightforward as the consistency of results in experimental stroke studies using aged animals is dependent upon the gender of the animals used.
In young rodents, the consensus seems to be that males sustain more histologic damage after experimental stroke than females. However, in aging animals, infarct size and functional outcomes can be worse in females than males. 111 Studies involving aging female animals consistently report worse stroke outcome, in terms of increased lesion volume and poorer functional ability, than in younger females regardless of strain and stroke model used (reviewed elsewhere 52 ). However, experimental studies using aged males have produced inconsistent results in terms of determining whether aged males have worse outcomes compared with young males. Some studies report that aged males experience greater ischemic damage, some report smaller ischemic lesions in aged males, and others report that aged males exhibit similar ischemic damage compared with young males. 52
Although the aging process itself is associated with a greater risk of mortality and poorer long-term functional outcomes,52,112,113 these detrimental effects, in terms of mortality and longer-term functional ability, seem to be direct consequences of the aging process
CONCLUSIONS
Evidence exists to suggest that gender influences many aspects of ischemic stroke including stroke risk/incidence, diagnosis, symptoms, treatment and outcomes. It is well documented from epidemiologic studies that during the premenopausal years, female gender is associated with a reduced risk of ischemic stroke and hormonal factors have been investigated as potential protective treatments. However, as discussed in this review, sex differences in ischemic stroke probably result from a combination of factors, including elements intrinsic to the sex chromosomes as well as the effects of sex hormone exposure throughout the lifespan, although we cannot discount the influence also of cultural and social factors. Research investigating the sexual dimorphism of stroke is only beginning to emerge but several studies suggest that different cell pathways are activated in males and females after ischemic stroke. Stroke researchers must consider the translational relevance of such sex differences as many are unaware of the potential confounding factors of sex differences. The majority of experimental stroke studies continue to focus on using young male animals despite the Stroke Therapy Academy Industry Roundtable (STAIR) recommendations that neuroprotective studies be performed in both male and female rodents. 116 A greater understanding of the mechanisms underlying sex differences in stroke and responsiveness to neuroprotection will lead to more appropriate treatment strategies for patients of both sexes.
DISCLOSURE/CONFLICT OF INTEREST
The author declares no conflict of interest.