
Abstract
We evaluated cortical damages following traumatic brain injury (TBI) in the acute phase with [123I] iomazenil (IMZ) single photon emission computed tomography (SPECT). In all, 12 patients with cerebral contusion following TBI were recruited. All patients underwent IMZ SPECT within 1 week after TBI. To investigate the changes in distribution of IMZ in the cortex in the chronic phase, after conventional treatment, patients underwent IMZ SPECT again. A decrease in the accumulation of radioligand for the central benzodiazepine receptor in the cortex corresponding to the contusion revealed with computed tomography (CT) scans and magnetic resonance imaging (MRI) were shown on IMZ SPECT in the acute phase in all patients. In 9 of 12 patients (75%), images of IMZ SPECT obtained in the chronic phase of TBI showed that areas with a decreased distribution of IMZ were remarkably reduced in comparison with those obtained in the acute phase. Both CT scans and MRI showed a normal appearance of the cortex morphologically, where the binding potential of IMZ recovered in the chronic phase. Reduced binding potential of radioligand for the central benzodiazepine receptor is considered to be an irreversible reaction; however, in this study, IMZ accumulation in the cortex following TBI was recovered in the chronic phase in several patients. [123I] iomazenil SPECT may have a potential to disclose a reversible vulnerability of neurons following TBI.
Introduction
[123I] iomazenil (IMZ) is a specific radioligand for the central benzodiazepine receptor and has been developed as a tracer for single photon emission computed tomography (SPECT) (Beer et al, 1990; Dey et al, 1994). As a decrease in the density of the central benzodiazepine receptor labeled with IMZ in SPECT images was also found to be associated with a decrease in the density of neurons in the gray matter according to the pathologic study in traumatic brain injury (TBI) (Benavides et al, 1989), the usefulness of IMZ SPECT in detecting incomplete cerebral infarction in the acute phase and epileptogenic foci has been investigated (Umeoka et al, 2007). These lesions detected with IMZ SPECT are visualized as a region where IMZ accumulations are decreased, whereas computed tomography (CT) and magnetic resonance imaging (MRI) showed normal regions morphologically. Moreover, in case of severe TBI, there is a case, in the clinical settings, head-CT scans and MR images examined immediately after the induction of head trauma, failed to find any abnormalities morphologically. In such cases, sometimes, gradually progressive global cerebral atrophies were shown in the course of the treatment in the chronic stage (Anderson et al, 1996; Gale et al, 1995). As far as these cases are concerned, conventional morphologic images are no longer valid. In recent years, several trials using functional images to visualize early changes reflecting brain damages in the acute phase after induction of TBI, which are not detected in CT scans and MRI, have been reported. Garnett et al (2000) have shown, using proton magnetic resonance spectroscopy techniques, that metabolic abnormalities exist in the morphologically normal-appearing white matter of patients with TBI by conventional MRI. Goetz et al (2004) have reported that there was a correlation between injury severity and increasing apparent diffusion coefficient (ADC), suggesting that ADC was a sensitive and independent marker of diffuse white matter tissue damage following traumatic insult. These new approaches to visualize brain damages, which are not detected in CT scans and MR images morphologically, are characteristic and worthy of note. However, in their manner, it is required to sample regions of interest, and detection of brain damages depends on targeting regions. Therefore, these approaches are unsuited for searching lesions of the whole brain. Gowda et al (2006) examined Tc-99m ECD (Ethyl Cysteinate Dimer) SPECT for patients with mild TBI in the acute phase. They have shown that the power of Tc-99m ECD SPECT to detect perfusion abnormalities is considerably sensitive, and that this sensitivity for detecting an organic basis in patients was much higher than CT scans. In their study, Tc-99m ECD SPECT visualized abnormal findings in the whole brain; however, it is not clear whether these perfusion abnormalities are reversible or irreversible and also whether these findings represent irreversible structural brain damage, and furthermore, it is questionable whether there is a causal relationship between these perfusion disorders and the eloquent neurologic deficits of the patients. As mentioned above, these trials of brain functional imaging for patients with TBI have become the focus of attention; however, at present, there is still no widespread useful functional imaging for patients with TBI. In this study, we used IMZ SPECT, which was able to visualize the viability of neurons distributed in the gray matter, to evaluate brain damage after TBI in the acute phase. As considerable abnormalities in cerebral metabolisms occurred in the acute phase after brain trauma (Bergsneider et al, 1997, 2000; Hattori et al, 2003, 2004; Wu et al, 2004a, b ), we examined IMZ SPECT again in the chronic stage to investigate the changes in IMZ accumulation in the gray matter. As a result, we obtained a remarkable phenomenon; therefore, we report the usefulness of IMZ SPECT with literary consideration.
Materials and methods
The subjects of this study were 12 patients whose CT and MRI images of the head showed cortical damage associated with cerebral contusions as a result of TBI. There were seven men and five women, and their average age was 51.8 ± 22.9 years. Detailed information about these 12 patients is provided in Table 1. In 6 of the 12 cases, cerebral contusion was complicated by an acute subdural hematoma, and diffuse axonal injury was observed in another case (case no. 12). The distribution of benzodiazepine receptors in the cortical areas was evaluated by IMZ SPECT in the acute stage within 1 week after injury in every case. Conventional treatment for cranial trauma was administered, and an IMZ SPECT reevaluation was performed within a period of 1 to 3 months later. In both the examinations in the acute stage and 1 to 3 months later, benzodiazepine receptor distribution was evaluated by SPECT images obtained 180 minutes after injection of the tracer. In 7 of the 12 cases, the mass effect produced by cerebral contusions caused an increase in intracranial pressure, and decompressive hemicraniectomy was performed because it reached a critical level. In all seven cases in which decompressive craniectomy was performed, both the IMZ SPECT examination in the acute stage and 1 to 3 months later were acquired in the state of decompressive craniectomy, and cranioplasty was not performed in any of them in the follow-up period. Thus, changes in imaging findings associated with cranioplasty in comparison with the images acquired in the acute stage did not appear to be worth taking into consideration. No drugs that act on benzodiazepine receptors were administered in the IMZ SPECT examinations in the acute stage and 1 to 3 months later. This study followed the Declaration of Helsinki principles. Written informed consent to participate in this study was obtained from the patient or from a family member.
Clinical features of the patients
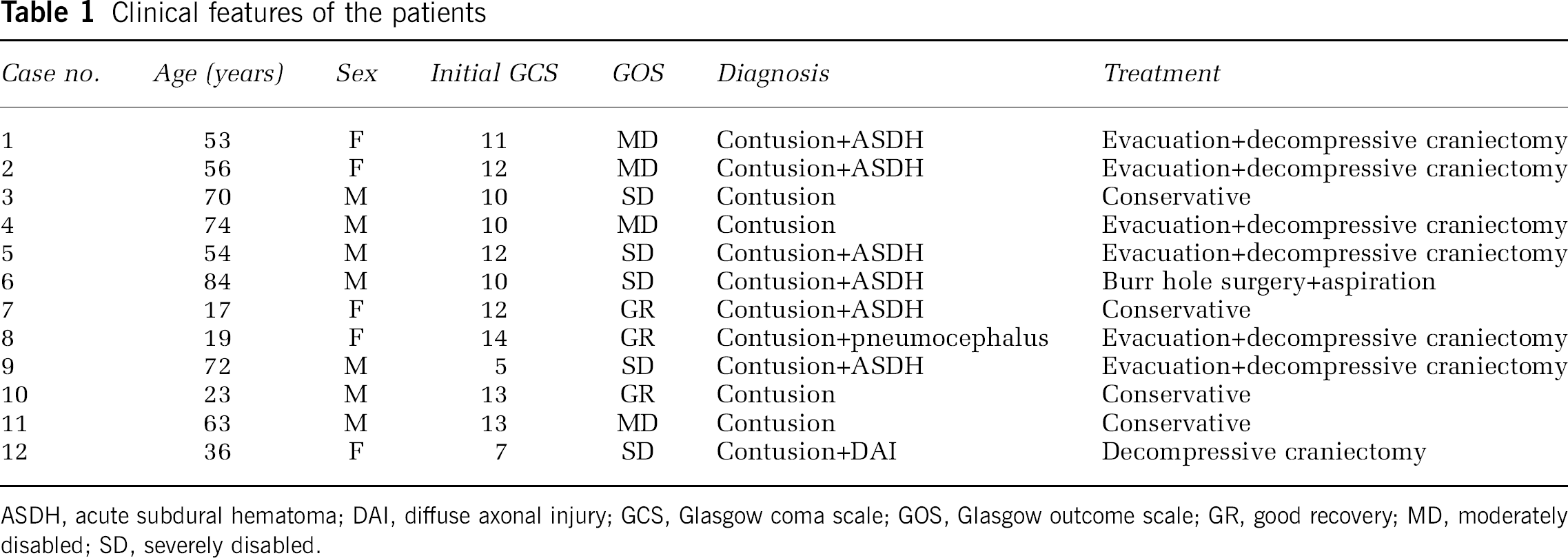
ASDH, acute subdural hematoma; DAI, diffuse axonal injury; GCS, Glasgow coma scale; GOS, Glasgow outcome scale; GR, good recovery; MD, moderately disabled; SD, severely disabled.
Morphologic Evaluation of the Brain Damage
Cranial CT (Siemens Somatom Sensation, Munich, Germany; 64-row multirow detector CT machine, Siemens) or cranial MRI (General Electric, Fairfield, CT, USA; Signa CV 1.5T) was performed on every patient on arrival at our department, and the presence of cerebral contusions was confirmed. In addition, cranial CT or cranial MRI was performed 1 month later at almost the same time as the IMZ SPECT examination, and images acquired were compared with SPECT images.
Actual Performance of 123I-Iomazenil Single Photon Emission Computed Tomography
In cases in which the patient was awake and able to respond to instructions, we acquired SPECT images without administering a sedative, and in all of the cases in which sedation was required, we used barbiturate anesthesia and essentially conducted the examination by endotracheal intubation with the patient connected to a respirator. Before the examination, the patient was administered potassium iodide orally or by infusion through a nasogastric tube, and exposure of the thyroid gland to radioactivity was prevented. The acquisition system used was a model GCA-9300a/pi (Triple-headed SPECT system, Toshiba Medical Systems, Ohtawara, Tochigi, Japan), and the image processing system used was a GMS-5500A/PI unit (Toshiba Medical Systems). Patients were injected intravenously with a 167 to 222MBq bolus dose of IMZ, and images were acquired 15 and 180minutes after the injection.
Evaluation of Benzodiazepine Receptor Distribution
In IMZ SPECT examinations, early images taken 15 minutes after tracer injection are obtained, and the delayed images acquired 180 minutes after administration can be used to evaluate the distribution of central benzodiazepine receptors. In cerebral contusions, decreased uptake is observed in delayed IMZ SPECT images in areas where benzodiazepine receptors are believed to have been lost at damaged sites in cortical areas. In this study, we conducted a statistical analysis using a normal database obtained from healthy subjects and identified sites where the distribution of central benzodiazepine receptors was significantly reduced by three-dimensional stereotactic surface projection (3D-SSP) analysis images (Minoshima et al, 1994). The location and extent of the areas where the distribution of the receptors projected to the surface was decreased were displayed and could be seen at a glance. We investigated how the location and extent of the areas where the distribution of benzodiazepine receptors had decreased had changed by comparing the IMZ SPECT examinations performed in the acute period and those performed 1 to 3 months later.
Image Analysis
We evaluated the difference of IMZ uptake between the acute and chronic stages stereotactically and quantitatively by 3D-SSP analysis.
We calculated the number of pixels for which the Z-score was > 2 in the cerebral hemisphere.
Three-dimensional stereotactic surface projections created using the Neurological Statistical Image Analysis Software (NEUROSTAT), developed by Minoshima et al (1994), was used to evaluate the spatial distribution of abnormal function. Each image set was realigned to the standard Talairach space. Differences in individual brain size were removed by linear scaling, and regional anatomic differences were minimized using a nonlinear warping technique. Subsequently, maximum cortical activity was extracted to adjacent predefined surface pixels on a pixel-by-pixel basis using a 3D-SSP technique. To quantify function deficits, normalized brain activity of each patient was compared with that of 18 normal controls (12 men and 6 women, mean age 27.2 ± 6.0 years) using Z-score analysis: (normal mean-individual value)/normal s.d. To measure the volume of Z-score change of the cerebral hemisphere, we used the stereotactic extraction estimation method developed by Mizumura et al (2003), which is an analytical method using a stereotactic region of interest template from the Talairach daemon (Talairach (Lancaster et al, 2000).
For 12 cases, we performed stereotactic extraction estimation analysis in the delayed images of IMZ in the acute and chronic stages. By stereotactic extraction estimation analysis, we calculated a ratio of accumulation decrease of a delayed image of IMZ for the whole cerebral hemisphere and compared it between the acute and chronic stages. Similarly, we calculated a ratio of accumulation decrease for a one-sided cerebral hemisphere. We investigated whether a one-sided cerebral hemisphere with a visual change shows significant improvement between the acute and chronic stages.
Results
Areas showing decreased iomazenil uptake were observed on the delayed images of all patients in the acute-stage IMZ SPECT examination performed within 1 week after TBI (Table 2). Areas showing decreased IMZ uptake that matched the locations of all of the sites where cerebral contusions were present on cranial CT images or MRI images were observed. Areas that showed decreased uptake on the delayed images also showed significantly decreased uptake in the 3D-SSP statistical analysis images. Areas showing decreased uptake in the delayed images similar to the acute-stage findings were seen on the IMZ SPECT examination performed in the chronic stage 1 to 3 months later. However, in 9 of 12 cases, areas that showed decreased iomazenil uptake in the delayed images of the acute-stage IMZ SPECT examination had clearly decreased in size on the same delayed images in the chronic stage.
Results of 123I-iomazenil SPECT
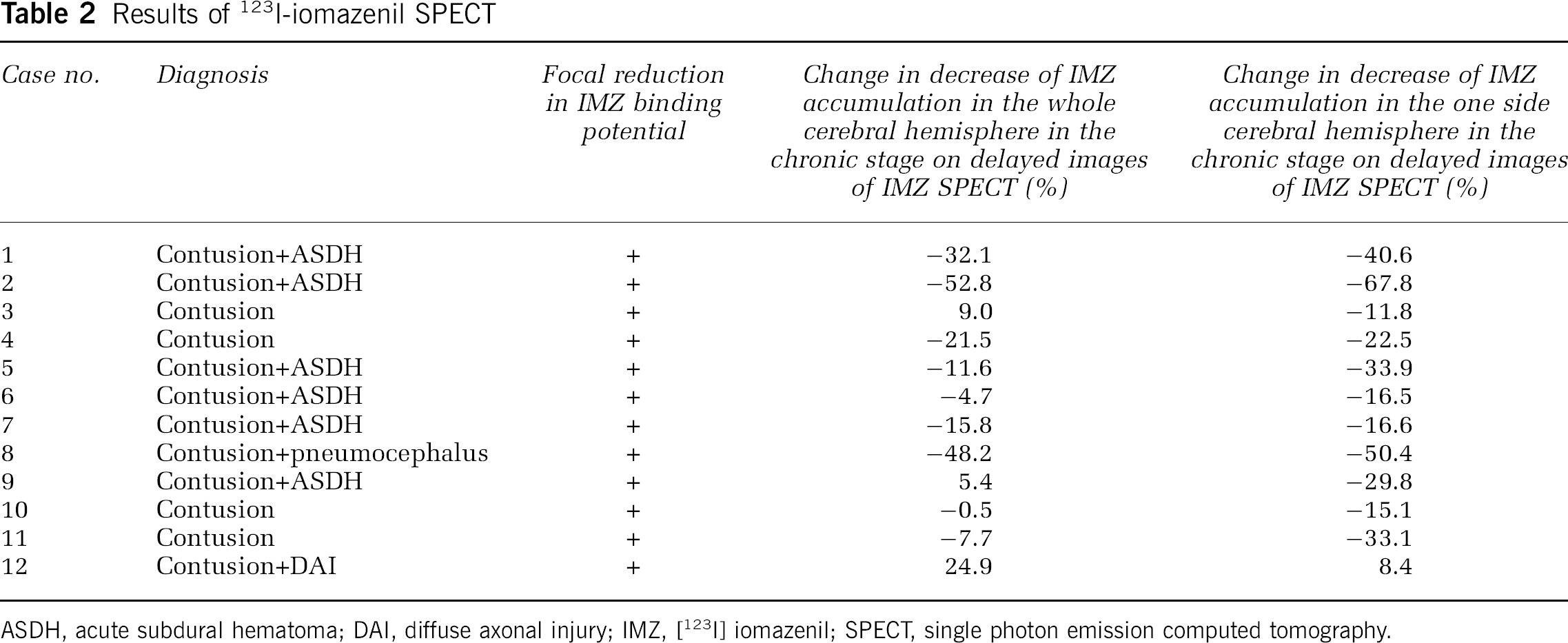
ASDH, acute subdural hematoma; DAI, diffuse axonal injury; IMZ, [123I] iomazenil; SPECT, single photon emission computed tomography.
The whole cerebral hemisphere did not show any significant change between the acute and chronic stages. The one-sided cerebral hemisphere which visually changed showed significant improvement (by paired t-test, P = 0.00203) of accumulation decrease between the acute and chronic stages (Figure 1).

This shows a change in the accumulation decrease ratio of one-sided cerebral hemisphere between an acute phase and chronic stages. The mean decrease ratio of one-sided cerebral hemisphere was 0.216 ± 0.087 (mean ± s.d.) in the acute stage, whereas it was 0.152 ± 0.069 in the chronic stage. A decrease ratio of one-sided cerebral hemisphere was improved between the acute and chronic stages significantly (P=0.00203).
A representative case is shown in Figures 2 to 4.
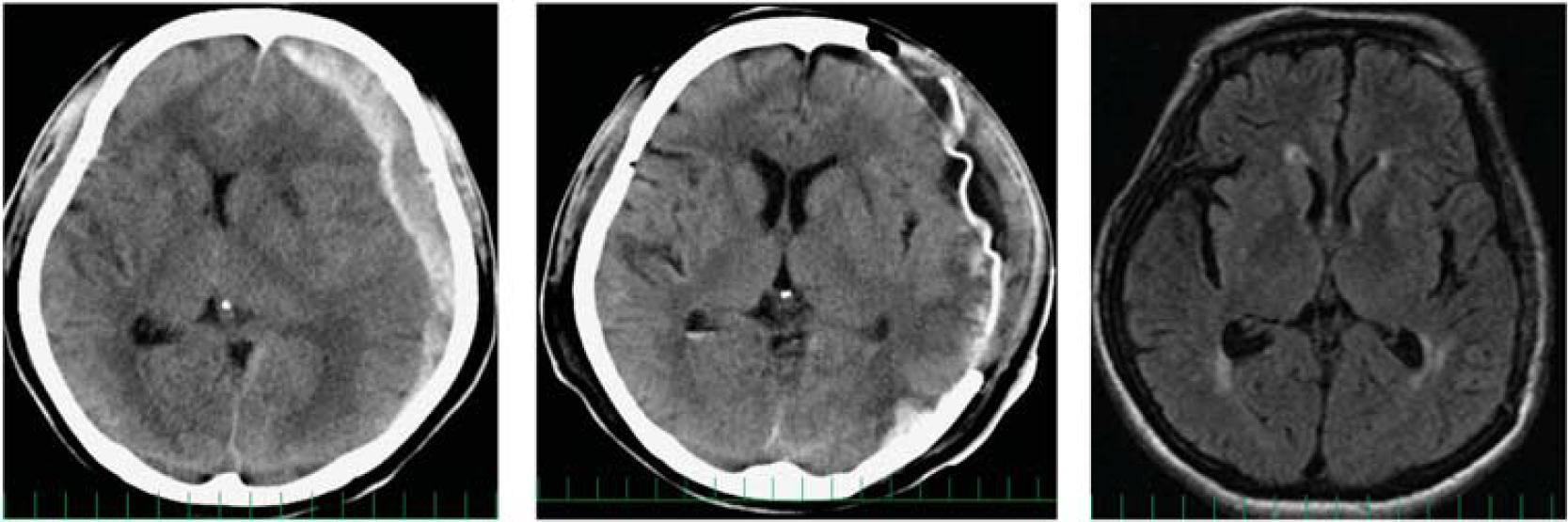
Cranial plain computed tomography (CT) image acquired immediately after the injury (left). A left acute subdural hematoma is visible, and a midline shift toward the opposite side can be seen. Postoperatively, the hematoma has been evacuated, and the midline shift has improved (middle). Cranial magnetic resonance imaging (MRI) image acquired in the chronic stage (1 month after the trauma) (left). With the exception of part of the white matter, no prominent damage is seen.
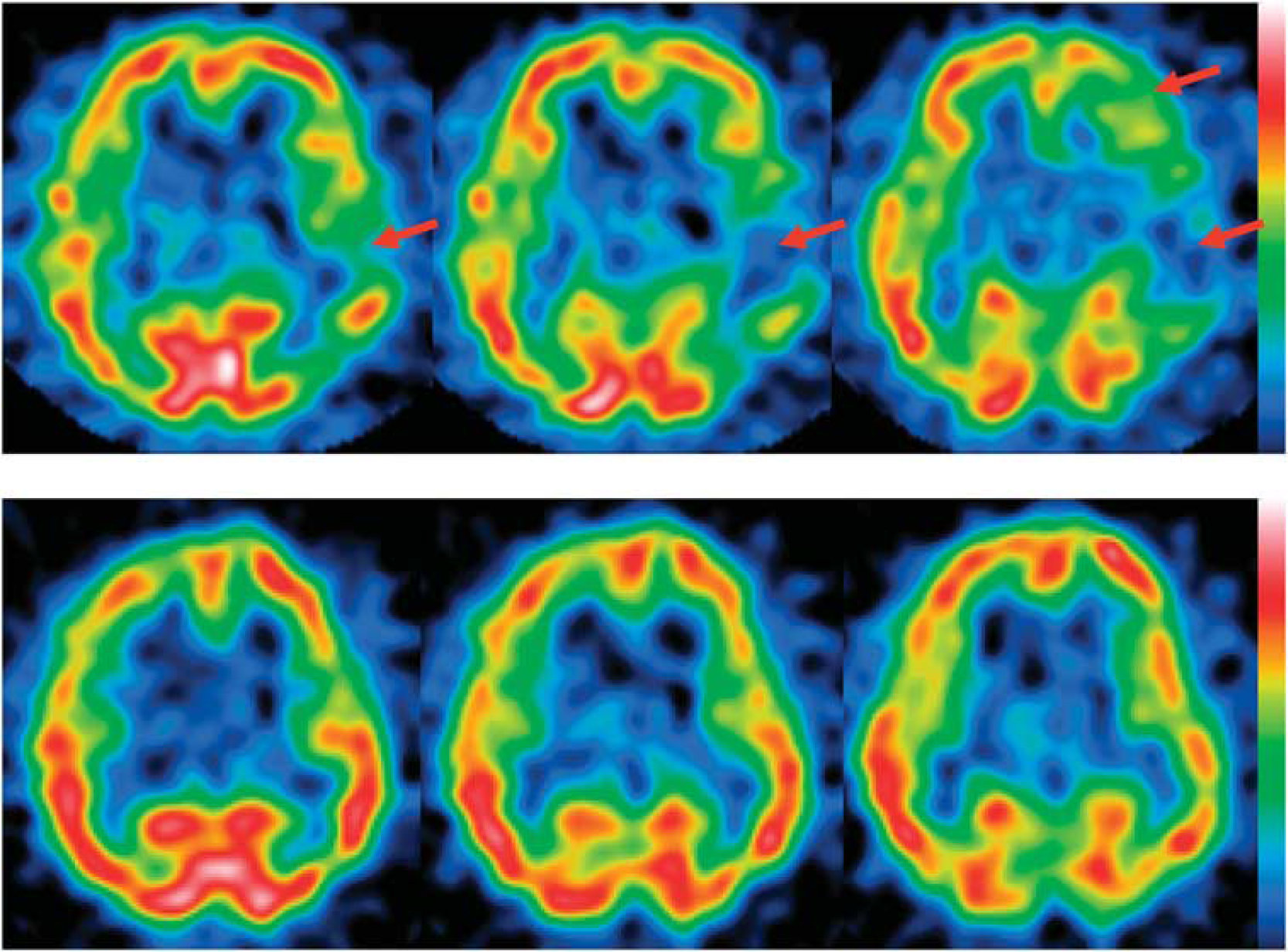
Delayed iomazenil single photon emission computed tomography (SPECT) image acquired in the acute stage after the trauma (upper). Decreased uptake can be seen in part of the left frontal lobe and over a wide expanse of the temporal lobe (arrows). Delayed iomazenil SPECT image acquired 2 months after the trauma (lower). Although areas of decreased uptake persist, marked recovery of uptake can be seen at the sites of the reduced uptake that are indicated by the arrows in the acute stage.
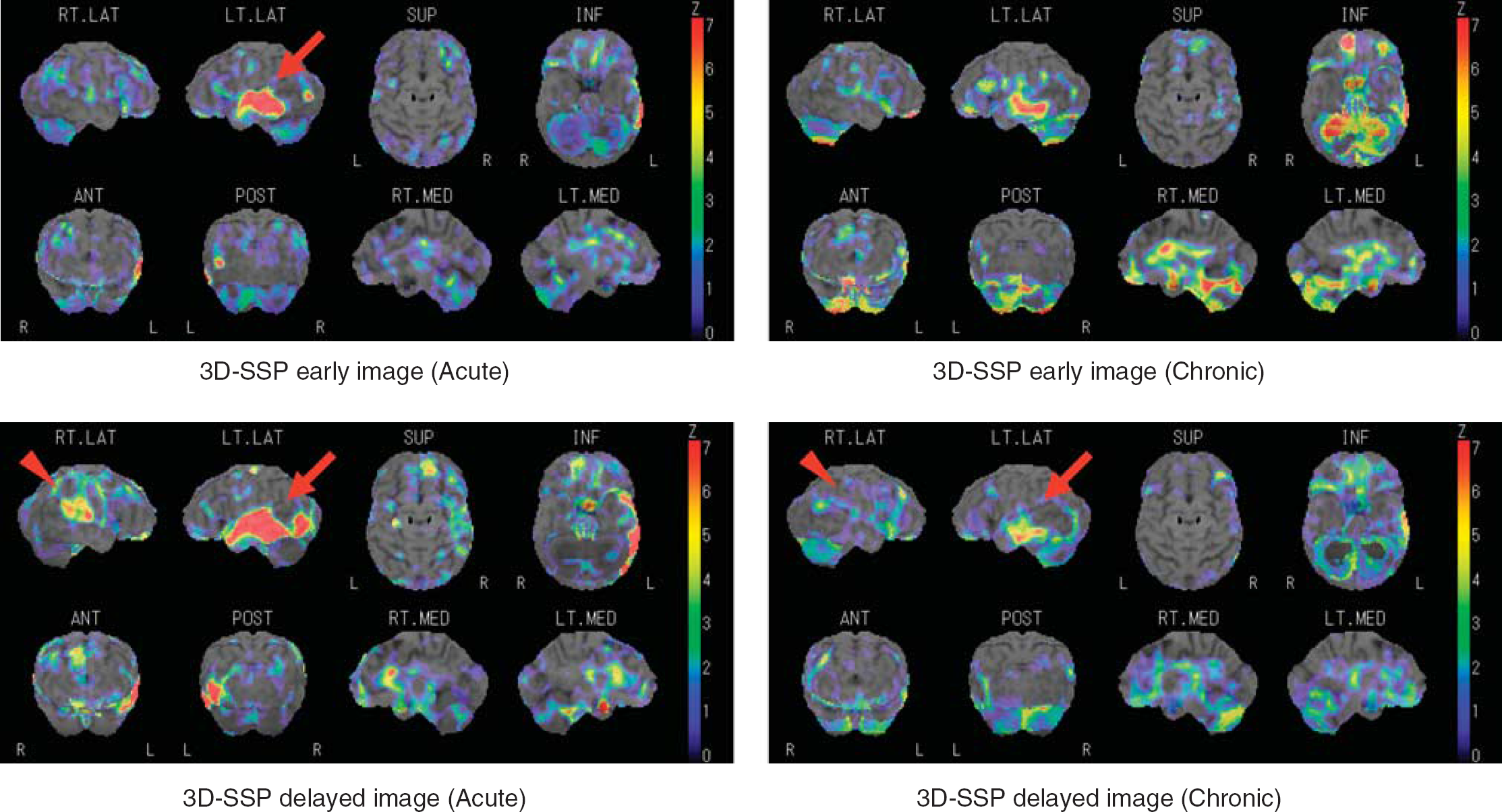
Upper left: early image of Iodine (I)-123 iomazenil single photon emission computed tomography (SPECT) using three-dimensional stereotactic surface projection (3D-SSP) acquired in the acute stage after traumatic brain injury. In the left temporal lobe, a significant decrease in distribution of [123I] iomazenil (IMZ) is detected (arrow). Upper right: early image of I-123 iomazenil SPECT using 3D-SSP 2 months after the trauma shows the changes in areas and expansion of reduced distribution of IMZ in the chronic stage compared with the acute stage. Lower left: delayed image of I-123 iomazenil SPECT using 3D-SSP acquired in the acute stage after the trauma. A significant change in the decreased uptake shown in the left frontal lobe and temporal lobe is clear on the brain surface axial image (arrow). A significant decrease was also shown in the right cerebral hemisphere (arrow). Lower right: delayed image of I-123 iomazenil SPECT using 3D-SSP 2 months after the trauma. The areas of significant reduced uptake have markedly decreased in size in comparison with the acute stage image.
Patient 1
In case no. 1, the injury was sustained when the motorcycle the patient was riding fell over. A left acute subdural hematoma was observed on cranial CT images, and because a midline shift to the opposite side as a result of the mass effect of the hematoma was observed, an emergency open evacuation of the hematoma and left decompressive hemicraniectomy were performed on the day of the injury (Figure 2). When IMZ SPECT was performed on postoperative day 4, marked decreases in IMZ uptake were observed in the left frontal lobe and the left temporal lobe cortex (Figure 3). Significant decreases were shown at the same sites in the statistical analysis images (Figure 4). Postoperatively, systemic management was continued, and as a result of physical therapy, improvement in neurologic symptoms was observed, and the patient became capable of performing independent activities of daily living. During the postoperative course, marked recovery of the decreased IMZ uptake in part of the left frontal lobe and temporal lobe was observed by IMZ SPECT performed in the chronic stage before cranioplasty. The recovery was also obvious when the areas of decreased uptake depicted on the 3D-SSP images were compared with the acute stage (Figure 4).
Even when we compared the areas that showed significant decreases in uptake by the statistical analysis images, as is clear from the imaging findings in the representative case as well, the surprising result was the shrinking of areas that showed decreased uptake in the acute-stage examination and examination 1 to 3 months later. A quantitative evaluation of IMZ accumulation in the cortex showed that the decrease in IMZ accumulation reduced in 9 of 12 cases (75%) in the late images of IMZ SPECT. In this study, cases that are not indicated in this assessment must be discussed. A remarkable cranial deformity following TBI is not available for assessment because of the difficulty in the transformation of each pixel for the patient's brain into the anatomic standard brain form with Talairach Atlas. In addition, an excessive deformity of the brain in the acute phase frequently changes shape in the chronic stage. Therefore, assessment of changes in IMZ uptake between the different periods lacks accuracy. Fortunately, the brains of the patients recruited in this study were not deformed after traumatic injury, beyond the limitations of the transformation process.
Discussion
Neuropathological studies have shown that eventual necrosis of the whole-brain tissue after occlusion of the cerebral artery was seen in the center of infarcts, whereas selective neuronal impairment, which was much more sensitive to the decrease in cerebral blood flow and lack of oxygen, was seen in the tissue surrounding infarction (Mies et al, 1983; DeGirolami et al, 1984). This specific neuronal impairment in the perifocal area after ischemic brain injury has not been detected on CT scans and MRI morphologically; therefore, IMZ SPECT has attracted considerable attention since this functional imaging makes it possible to visualize the specific neuronal impairment in the perifocal area in the acute phase. A number of studies have shown the usefulness of functional imaging of central benzodiazepine receptor distribution for patients with cerebral infarction and epilepsy, using radioligands for the receptors, including 11C-flumazenil (FMZ), which had been developed as a tracer for positron emission tomography (PET) (Heiss et al, 1997, 1998; Müller et al, 2002; Rudolf et al, 2000; Saur et al, 2006). However, in the past, there was no report which has shown that the binding potential of radioligand for the central benzodiazepine receptor recovered in the chronic stage after a remarkable decrease in distribution of the ligands in the acute phase of brain damages, and there is no advocacy to support that a decrease in the binding potentials of IMZ and FMZ can be a reversible phenomenon in part.
Heiss et al (2000) assessed cortical blood flow using [15O]H2O and binding potentials of FMZ by PET for patients with acute, hemispheric ischemic stroke at the beginning of thrombolysis with recombinant tissue plasminogen activator. In their study, only distinct areas of decreased FMZ binding within severely hypoperfused regions were correlated with irreversible cortical damages detected on final CT/MRI that are permanent morphologic lesions. According to their result, it was suggested that radioligand for the central benzodiazepine receptor can be used to distinguish the potentially viable cortex from tissue that cannot be salvaged by any treatment.
Nakagawara et al (1997) estimated IMZ binding of the receptor in the reperfused cortex after embolic occlusion of an intracranial artery, using a two-compartment model to compute the distribution volume of IMZ in relative units. They suggested that the reduction in benzodiazepine receptor concentration in the reperfused cortex that remained structurally intact was likely to be the result of injury involving only a limited number of neurons, and that this degree of viability of the ischemic cortex can be quantified by IMZ.
Hatazawa et al (1995a) analyzed IMZ images obtained from patients with middle cerebral artery territory infarction for benzodiazepine receptor binding. They defined the area of cortical infarction as the CT hypodense lesion and the peri-infarct area as the CT normodense area surrounding cortical infarction. [123I] iomazenil uptake in these regions of interest was analyzed by taking the ratio of the lesion to the contralateral mirror region. They have shown that IMZ uptake was significantly decreased in the infarct and peri-infarct areas in comparison with the contralateral mirror region, suggesting that reduced IMZ uptake in the peri-infarct area may be due to a selective neuronal necrosis not previously revealed by other conventional imaging modalities. In their report, as no increase in IMZ binding was found within a 6-month period while all patients showed consistent reduction, authors considered that cortical damages observed by IMZ binding may be irreversible.
Traumatic brain injury is basically different in a category of disease from cerebral infarction; therefore, it may be overextended to discuss about the distribution of decreased cortical IMZ uptake in the traumatically injured brain being classed with that in cerebral infarction. As a thought-provoking study, Hatazawa et al (1995b) also used IMZ SPECT for patients with subcortical hemorrhage to investigate the distribution of the central benzodiazepine receptor in the cortex remote from subcortical hematoma. They have shown that IMZ binding was decreased in the ipsilateral cerebral cortex remote from the subcortical hematoma, and that the magnitude of decline was correlated with the initial volume of hematoma. Authors speculated that compression of the cortical gray matter due to hematoma and surrounding edema, subsequent ischemic injury, and transneuronal degeneration were possible mechanisms of this pathogenesis. In case of TBI, localized mechanical stress to the brain substance leads to tissue destruction accompanied by hemorrhage. It is possible to suppose that compression to the surrounding brain tissue and perifocal brain edema secondary to this hemorrhage following TBI are in common with spontaneous subcortical hemorrhage. Furthermore, it is equally important to the argument described above that there is no report detecting the recovery of reduced binding potential of radioligand for the central benzodiazepine receptor in the cortex, and this decrease in radioligand uptake has been considered to be an irreversible phenomenon entirely. Unfortunately, in the study investigated by Hatazawa et al, it has not been investigated how the decreased distribution of IMZ would turn out in the chronic phase when the hematoma would be in progress of absorption and the mechanical compression effect of hematoma and perifocal brain edema would disappear.
Considering the fragile plasticity of neurons, it may be still open to question to think that neurons come back to life after their loss of viability. However, we may have a clue to help solve the mechanisms of this phenomenon with changes in cerebral metabolism.
The study investigated by Shiga et al (2006) partially accounts for the relationship between the viability of cortical neurons and cerebral metabolism. They recruited patients with some symptoms after TBI who underwent FMZ PET to investigate the relationship between the distribution of central benzodiazepine receptor and cerebral metabolism. None of the patients had abnormal findings on MRI, whereas all of them showed areas with abnormally low CMRO2. It was noteworthy that low uptake on the binding potential of FMZ was observed in 60% of the patients and no lesions that showed low uptake on binding potential images were without low CMRO2; conversely, there were 14 lesions with low CMRO2 but without abnormalities in the binding potentials of FMZ. Consistent with their report, Kaneko et al (2006) examined IMZ SPECT, 123I-IMP SPECT, and 18F-FDG PET for patients with temporal lobe epilepsy to discover the localization of epileptogenic foci. In consequence, in their study, although FDG PET and IMP SPECT showed widespread decreased uptake in the entire left temporal lobe, the extent of the decreased uptake area on IMZ SPECT was restricted to the left medial temporal lobe.
It is beyond dispute that areas with abnormalities in brain metabolisms exist in the cortex in the acute phase following TBI (Bergsneider et al, 1997, 2000; Hattori et al, 2003, 2004; Wu et al, 2004a, b ). It may be possible to assume that in part of these areas with metabolic abnormalities, the affinity of central benzodiazepine receptor binding is supposed to be reduced in the acute phase reversibly. Thereafter, in part of the areas with reduced distribution of IMZ within which cerebral metabolism would be normalized, binding potential may be recovered in the chronic phase. In this case, decreased affinity of central benzodiazepine receptor binding may not lead to selective neuronal death, excluding irreversible reactions. Consequently, in the area where brain metabolism would not be normalized, reduced binding potential of IMZ in relation to the selective neuronal death would remain permanently. As far as we look the literature over, no significant intrinsic neurotransmitter is known to bind to central benzodiazepine receptors. To show the validity of these hypotheses, it would be required to evaluate the regional cerebral metabolism in the acute and chronic phases, respectively, and to investigate the changes. These matters are assignments, which now confronts us.
Conclusions
In this study, we used IMZ SPECT to evaluate cortical damages following TBI. Although a decrease in the binding potentials of radioligand for the central benzodiazepine receptors has been considered to be an irreversible reaction, however, accumulation of IMZ recovered in the chronic phase following TBI at pericontusional region where binding potentials of IMZ were remarkably decreased in the acute phase. The mechanisms of this phenomenon reflecting regained viability of neurons were supposed to be related to the changes in cerebral metabolism. [123I] iomazenil SPECT may have a potential to disclose a reversible vulnerability of neurons following TBI.
Footnotes
The authors declare no conflict of interest.