
Abstract
The effect of carbon dioxide (CO2) on cerebral metabolism is of tremendous interest to functional imaging. In particular, mild-to-moderate hypercapnia is routinely used in calibrated blood oxygen-level dependent (BOLD)-functional magnetic resonance imaging (fMRI)-based quantification of cerebral oxidative metabolism changes (ΔCMRO2), and relies on the assumption of a stable CMRO2 during CO2 challenges. However, this assumption has been challenged by certain animal studies, necessitating its verification in humans and under conditions customary to fMRI. We report, for the first time, on global ΔCMRO2 measurements made noninvasively in humans during graded hypercapnia and hypocapnia. We used computerized end-tidal CO2 modulation to minimize undesired concurrent changes in oxygen pressure, and our findings suggest that no significant change in global CMRO2 is expected at the levels of end-tidal CO2 changes customary to calibrated BOLD.
Keywords
Introduction
Carbon dioxide (CO2) is a potent vasodilator, and its effect on cerebral metabolism is of great interest. Notably, hypercapnia is routinely used in calibrated blood oxygen-level dependent (BOLD) functional magnetic resonance imaging (fMRI) for estimating changes in cerebral oxygen metabolism (ΔCMRO2), but this methodology is contingent upon the assumption of negligible ΔCMRO2 during hypercapnia-induced cerebral blood flow (CBF) increases (Davis et al, 1998; Hoge et al, 1999). Although CMRO2 behavior under manipulations of end-tidal partial pressure of CO2 (PETCO2) has been investigated previously in animals (Hino et al, 2000; Horvath et al, 1994; Jones et al, 2005; Martin et al, 2006; McPherson et al, 1991; Yang and Krasney, 1995; Zappe et al, 2008), the wide range of anesthetic agents used, compounded by the diverging levels of PETCO2 perturbations involved, has made it difficult to draw definitive conclusions regarding the CMRO2 response during hypercapnia and hypocapnia with regard to human fMRI. Furthermore, the sampling intervals in these experiments were largely inadequate to capture the dynamic CMRO2 changes related to transient metabolic responses, and the PETCO2 manipulations were too severe to be directly interpreted for human fMRI.
In spite of this need for verification, CMRO2 invariability has yet to be established for the range of PETCO2 values relevant for functional imaging, as the corresponding experiments are technically demanding. Conventionally, human cerebral oxidative metabolism has been assessed invasively through arteriovenous blood oxygenation differences, obtained through internal jugular catheterization. In this study, we build on this well-established concept, and estimate CMRO2 changes from flow and oxygenation data using a magnetic resonance-equivalent of the Kety–Schmidt technique. In particular, we use pulsed arterial-spin labeling (PASL), phase-contrast (PC) flow imaging, as well as
Materials and methods
All acquisitions were performed using a Siemens Trio 3-T system (Siemens, Erlangen, Germany) on 10 healthy adult subjects (age = 25.3 ± 3.6 years, 5 women) who gave informed consent according to the protocols specified by our Institutional Review Board. The body coil was used for radio frequency transmission and a phased-array neurovascular coil for reception. A three-dimensional 1-mm isotropic resolution
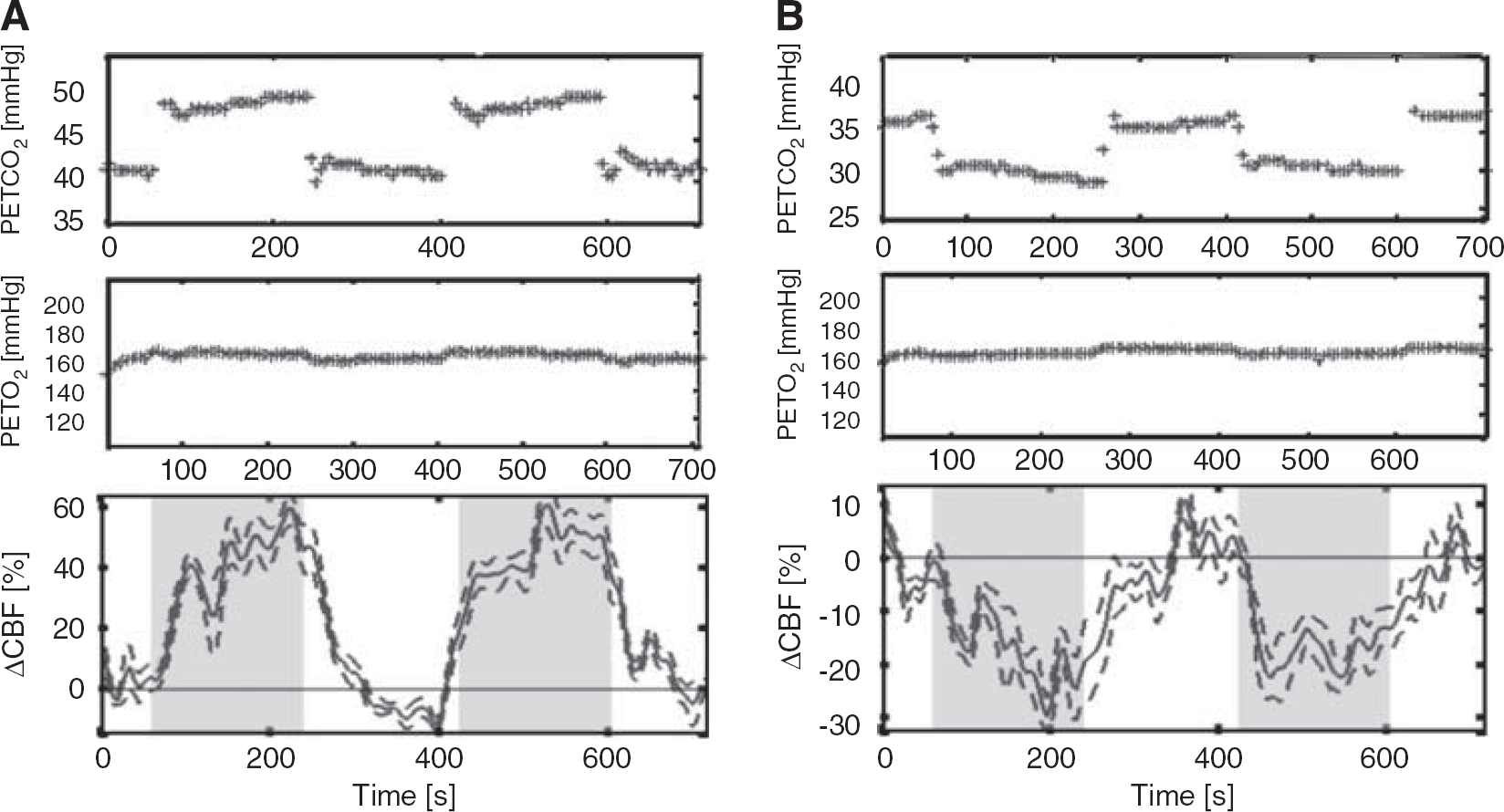
Mild and moderate levels of hypercapnia and hypocapnia were induced through the administration of mixtures of CO2 and medical air using the RespirAct breathing circuit (Thornhill Research, Toronto, ON, Canada), which provided computerized and independent targeting of PETCO2 and PETO2 (partial pressure of end-tidal oxygen) based on sequential gas delivery (Slessarev et al, 2007). This device provided high stability in PETCO2 targeting, while maintaining significantly more constant PETO2 levels than manual methods, both of which are crucial to the accurate quantification of CMRO2 changes due solely to PETCO2 changes. Each 12-minute PASL measurement consisted of three (60 seconds off:180 seconds on:120 seconds off) paradigms. In addition, two-dimensional cine PC flow data were obtained from five subjects in the internal carotid and vertebral arteries. These vessels account for the majority of cerebral inflow, and the corresponding PC acquisition (2.5 minutes) was used for cross-validation with the PASL data as a measure of global CBF. A finger pulse oximeter provided cardiac triggering and arterial oxygen data.
For each functional run of each subject, subject-specific brain masks were derived by applying an intensity threshold to the PASL control images. The resultant masks were manually verified to ensure exclusion of extracerebral structures, and applied to the PASL data to assess global flow changes. Using the venous

where Ψ = ΔCMRO2/ΔCBF,
Results and Discussion
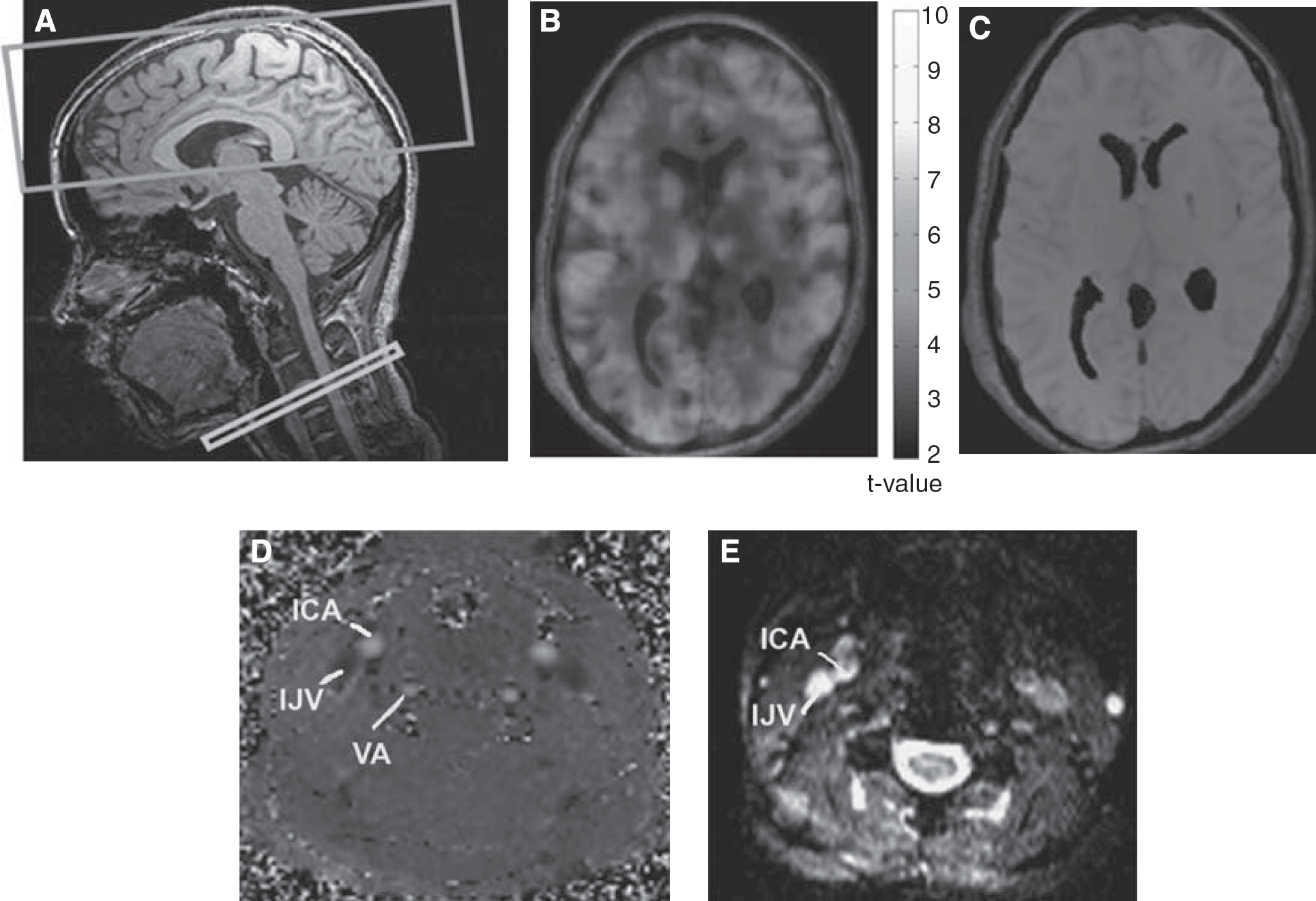
Typical PASL, internal jugular venous relaxometry, and internal-carotid PC flowmetry images are shown in Figure 1. The average estimated baseline venous oxygenation (
(
(
Physiologic measurements at all four levels of PETCO2 manipulation (mean ± s.d.); statistically significant differences are denoted by asterisks (*)
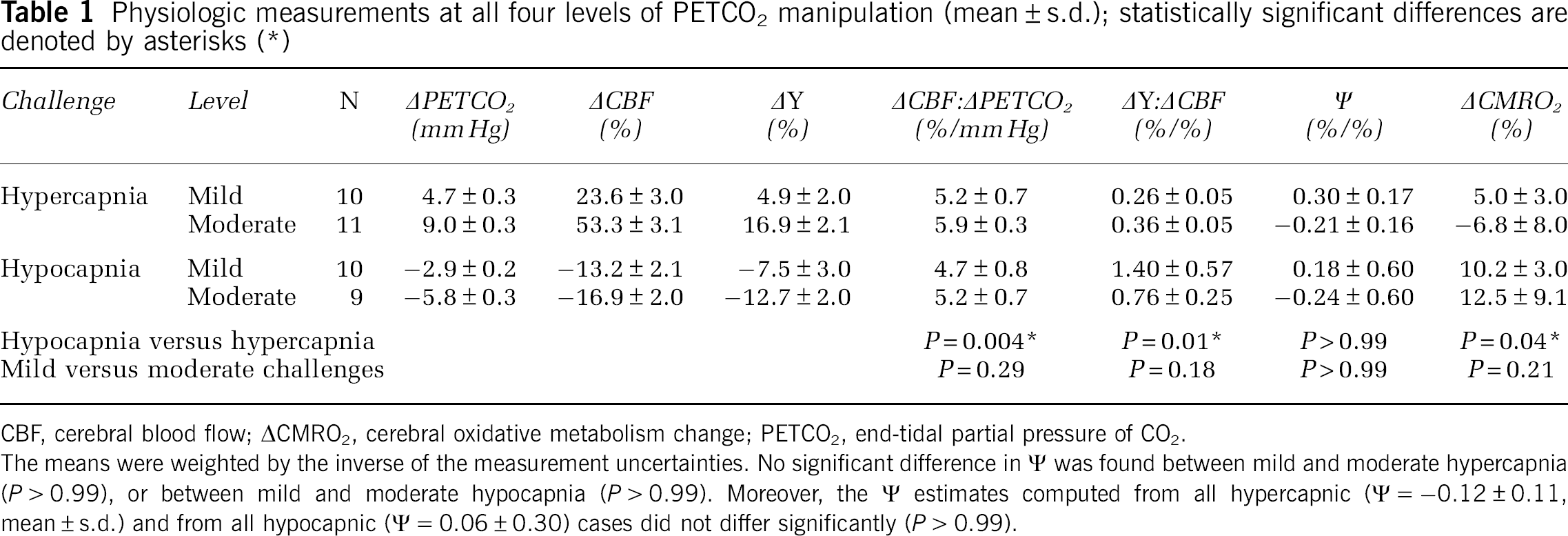
CBF, cerebral blood flow; ΔCMRO2, cerebral oxidative metabolism change; PETCO2, end-tidal partial pressure of CO2.
The means were weighted by the inverse of the measurement uncertainties. No significant difference in Ψ was found between mild and moderate hypercapnia (
Whole-brain PASL ΔCBF in the whole-brain masks and PC flow measurements were found to be equivalent, as detailed in Table 2. Using PASL-based global ΔCBF, global ΔCMRO2 and Ψ values were estimated for each challenge. The ΔCMRO2 values computed on the basis of equation (1), did not differ significantly between mild and moderate levels of hypercapnia (
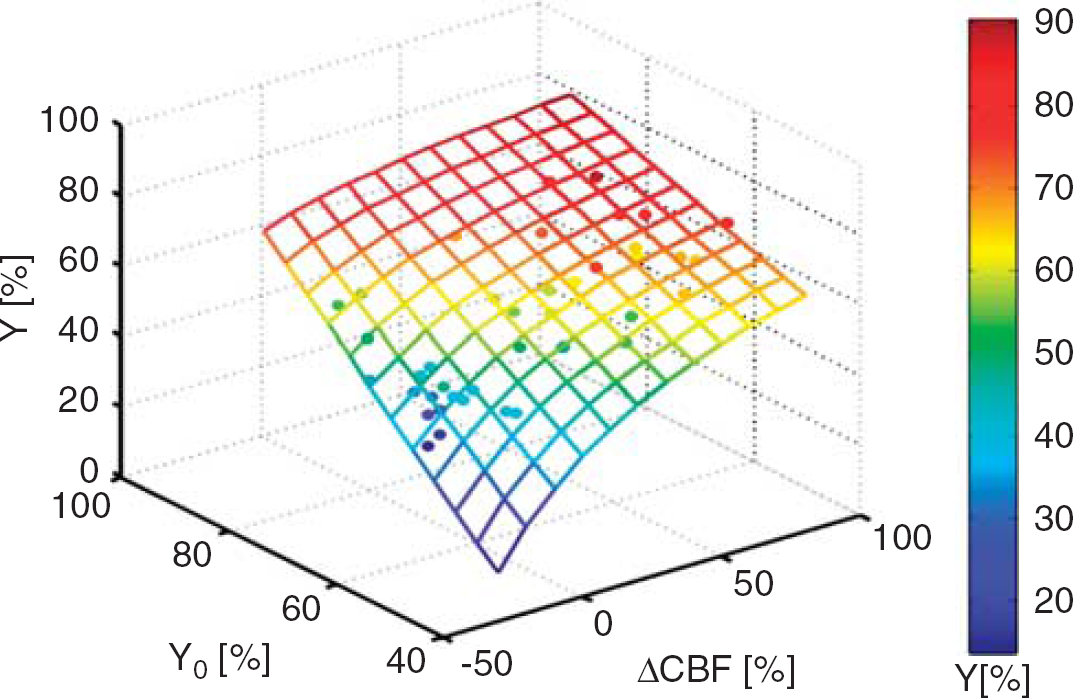
The relationship derived from the nonlinear fit of the data (closed dots) to the model (mesh) are shown, and the model fit was characterized by a correlation coefficient of
Comparison of hypercapnic CBF modulation measured using PASL and PC techniques
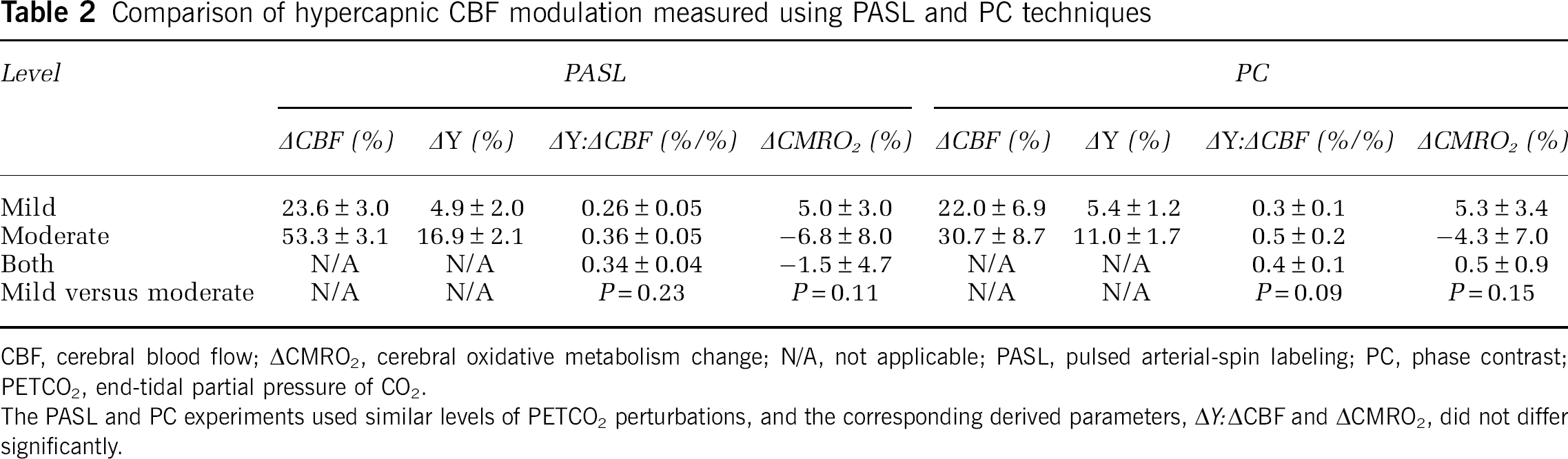
CBF, cerebral blood flow; ΔCMRO2, cerebral oxidative metabolism change; N/A, not applicable; PASL, pulsed arterial-spin labeling; PC, phase contrast; PETCO2, end-tidal partial pressure of CO2.
The PASL and PC experiments used similar levels of PETCO2 perturbations, and the corresponding derived parameters, Δ
Our measurement of cerebral venous oxygenation (
Although the current measurements show an absence of substantial global CMRO2 modulation by low levels of PETCO2 modulation, they do not preclude the possibility of spatial heterogeneities in the CMRO2 response to capnic challenges. For instance, a slight increase in neuronal activity modulations by fluctuating inhaled CO2 in the pons and medulla may occur, while decreases in motor synaptic synchrony (Biswal et al, 1997) have also been observed, potentially linked to CO2-mediated suspension in oxidative metabolism fluctuations (Hudetz et al, 1998) and slight alterations in the intrathalamic network (Steriade et al, 1996). On the basis of our experimental observations, we expect the spatial distribution and the magnitude of this response to also exhibit sizeable subject dependence. In view of the sources of variation, we sought to assess group trends, and to verify whether the assumption of negligibility of ΔCMRO2 globally is reasonable for the purpose of calibrated BOLD.
Several animal studies, invaluable precursors to similar experiments in humans, document the CMRO2 response during hypercapnic challenges, but thus far, the conclusions have been inconsistent. The CMRO2 invariability was reported by Hino et al (2000), McPherson et al (1991), and Yang and Krasney (1995), in anesthetized lambs and dogs, as well as in awake sheep, respectively, at ΔPETCO2 values of up to 30 mm Hg. In contrast, Horvath et al (1994) showed a ∼30% decrease in CMRO2 in anesthetized rats (ΔPETCO2≈50 mm Hg), whereas Jones et al (2005) found a 30% CMRO2 increase during 10% hypercapnia in anesthetized rats (8 minutes, ΔPETCO2≈50 mm Hg), and negligible ΔCMRO2 at 5% CO2 (ΔPETCO2≈25 mm Hg). The latter result was corroborated by findings in awake rats by Martin et al (2006) (5% CO2), but questioned by data obtained from the study by Zappe et al (2008), which showed a ∼15% CMRO2 reduction during 6% CO2 (ΔPETCO2 = 24 mm Hg) in anesthetized macaques. These variations in outcome can in part be attributed to the substantial methodological differences, because: (1) different types of anesthesia and states of alertness can alter the neuronal response significantly and (2) the levels and durations of PETCO2 manipulations across these studies varied substantially (the duration varying from 60 seconds to 96 hour). More importantly, the comparatively high severity of the above PETCO2 perturbations preclude comparability with commonly used human fMRI paradigms. Further complications stem from evidence in the literature that the general response to inhaled CO2 may be highly species- and subject-dependent, as a 5% CO2 challenge in awake humans rarely produces as much as a 25 mm Hg PETCO2 increase. Given these considerations, we regard the widely varying experimental protocols to be a key potential contributor to the discrepancies among animal and human literature, which must be interpreted with care.
In summary, in this study, we sought to address accurate ΔCMRO2 measurement during hypercapnia and hypocapnia in awake humans, which has traditionally been hindered by nontrivial methodological challenges, particularly, the reproducible targeting of PETCO2 values and in the effective minimization of concurrent PETO2 variations. We explored the persisting question of whether the levels of end-tidal CO2 manipulations commonly used in human calibrated fMRI experiments can be expected to elicit significant changes in global CMRO2. We circumvented some of the key traditional challenges by using computerized PETCO2 and PETO2 targeting, and performed global ΔCMRO2 measurements in awake humans during graded hypercapnia and hypocapnia within a range chosen to address fMRI applications (more specifically, ranging from −6 to + 9 mm Hg). Under such conditions, we found no evidence of significant changes in global CMRO2 during PETCO2 manipulations. Therefore, our findings support the assumption of negligible ΔCMRO2 under the conditions widely used in calibrated fMRI studies of awake humans.
Footnotes
The authors declare no conflict of interest.