
Abstract
Positron emission tomography with O-15-labeled water was used to study at rest the neurophysiological effects of bilateral external globus pallidus (GPe) deep brain stimulation in patients with Huntington's disease (HD). Five patients were compared with a control group in the on and off states of the stimulator. External globus pallidus stimulation decreased neuronal activity and modulated cerebral connectivity within the basal ganglia-thalamocortical circuitry, the sensorimotor, and the default-mode networks. These data indicate that GPe stimulation modulates functional integration in HD patients in accordance with the basal ganglia-thalamocortical circuit model.
Keywords
Introduction
Huntington's disease (HD) is an autosomal dominant neurodegenerative disease resulting in progressive impairments in motor function, cognition, and behavior. A characteristic feature of HD is the presence of chorea, which is related to striatal neuron degeneration. A standard model proposes that the striatum forms the input nucleus of a basal ganglia-thalamocortical circuitry integrating cortical and thalamic afferents (Alexander et al, 1986). Striatal projection neurons target either the external globus pallidus (GPe) (indirect pathway) or the internal globus pallidus (direct pathway), projecting to the motor cortex through the thalamus. Activation of the direct pathway disinhibits the thalamus, thereby increasing thalamocortical activity, whereas activation of the indirect pathway further inhibits thalamocortical neurons. In HD, the preferential loss of striatal neurons contributing to the indirect pathway leads to reduced inhibition of GPe and excessive inhibition of the subthalamic nucleus, thus concurring to hyperstimulation of the motor network and chorea (DeLong, 2000). Therefore, a potential therapeutic approach for HD hyperkinetic symptoms could consist in GPe inhibitory stimulation to indirectly reduce thalamocortical hyperactivity, as already suggested by animal experiments (Temel et al, 2006). This stimulation is also expected to alleviate disturbances in the dorsolateral prefrontal and lateral orbitofrontal circuits responsible for the cognitive and behavioral symptoms in HD (Alexander et al, 1986; DeLong, 2000; Temel et al, 2006).
In a group of HD patients included in a clinical trial on bilateral high-frequency deep brain stimulation (DBS) of GPe (GPe-DBS), we used positron emission tomography (PET) with oxygen-15-labeled water (H2 150) to study the neurophysiological effects of GPe-DBS at rest. We characterized the changes in brain perfusion and effective connectivity associated with GPe-DBS.
Materials and methods
Patients
Five right-handed symptomatic HD patients with GPe-DBS (3 women; age range: 41 to 60 years) and 15 right-handed healthy adult volunteers (10 women; mean age: 40.3 years; range: 25 to 60 years) gave informed consent to participate in the clinical and imaging studies approved by the institutional ethics committees. Patients with HD were genetically confirmed (range of CAG repeats: 41 to 53), their symptoms appeared 2 to 5 years before the present investigation, and the time between electrode implantation and PET ranged from 12 to 19 months. Patients' total functional capacity scores ranged from 10 to 12 (Shoulson and Fahn, 1979) (Supplementary Information).
Positron Emission Tomography Data Acquisition and Analysis
Subjects were scanned with a Siemens ECAT EXACT HR+ tomograph using automatic administration of repetitive H2150 bolus injection and image acquisition procedure as described elsewhere (Lipschutz et al, 2002). Control participants were scanned twice in eye-closed rest during a single imaging session. Patients with HD had two imaging sessions in identical conditions (two scans in eye-closed rest) with a time interval of 7 days, respectively, with the GPe stimulator switched on (on state) and switched off (off state). Patient and PET investigators were blinded to the stimulator status, which was randomly set 7 days before each PET session to ensure investigation in stabilized motor and cognitive status, based on known physiologic effects of DBS (Temperli et al, 2003). Random design was used to control for test–retest effects. Clinical stimulation parameters were kept unchanged (frequency: 130 Hz; voltage: 1 to 3 V; pulse width: 60 to 90 microseconds).
Positron emission tomography data were preprocessed and analyzed using the voxel-based statistical parametric mapping method (SPM8, Wellcome Department of Imaging Neuroscience, London, UK). Images were spatially realigned, normalized, and smoothed using a 16-mm full-width half-maximum isotropic Gaussian kernel. Global flow adjustment was performed by proportional scaling.
First, group-level subtractive analyses compared patients in the on and off states, and each state with control PET data. For these analyses, t-contrasts identified brain regions showing a significant decrease or increase in regional cerebral blood flow (rCBF). Thereafter, rCBF changes characterizing the on state in HD patients were identified in the comparison between on state and controls, masked exclusively by the comparison between off state and controls.
Finally, we performed effective connectivity analyses using pathophysiological interaction (PPI), adapted from psychophysiological interaction (De Tiege et al, 2004). In this study, PPI analyses were used to search in HD patients for GPe stimulation-induced changes in the contribution of a brain area to the level of rCBF in another brain area. Pathophysiological interaction analyses were conducted under the
All results of SPM analyses were considered significant at
Results
Regional Cerebral Blood Flow Changes During Resting State in Huntington's Disease Patients
Compared with controls, the off state was characterized by a significant relative rCBF decrease in the basal ganglia (GP, putamen, and thalamus) and in the fronto-parieto-temporal cortical regions involving primary sensori-motor cortices, supplementary motor areas, premotor cortices, dorsolateral prefrontal cortices, superior temporal gyri, insula, precuneus, and anterior and posterior (PCC) cingulate cortices (Figure 1A). A significant relative increase in rCBF was found in the cerebellum.
Exclusive masking analyses revealed in the on state a further significant rCBF decrease in the sensori-motor network (primary sensori-motor cortices, supplementary motor areas, premotor cortices), the anterior cingulate cortex, and in other regions of the default-mode network (DMN) (precuneus and PCC), the superior temporal gyri, and prefrontal regions (dorsolateral prefrontal cortices, frontal eye fields) (Figures 1B and 1C). Masking analyses revealed no significant rCBF increase in the on state compared with the off state. Direct comparisons of HD patients in the on and off states did not reach significance.
External Globus Pallidus Stimulation-Induced Changes in Cerebral Connectivity in Huntington's Disease Patients
Pathophysiological interaction analyses using thalamic seed voxels showed significant GPe-DBS-induced changes in effective connectivity with the PMC and the cerebellum. Indeed, GPe-DBS reversed the correlation directionality between the thalami and PMC from negative in the off state to positive in the on state, and conversely for the thalami and cerebellum (Table 1, Figure 1D).
Pathophysiological interaction (PPI) analyses showing GPe stimulation-induced changes in cerebral connectivity in Huntington's disease patients
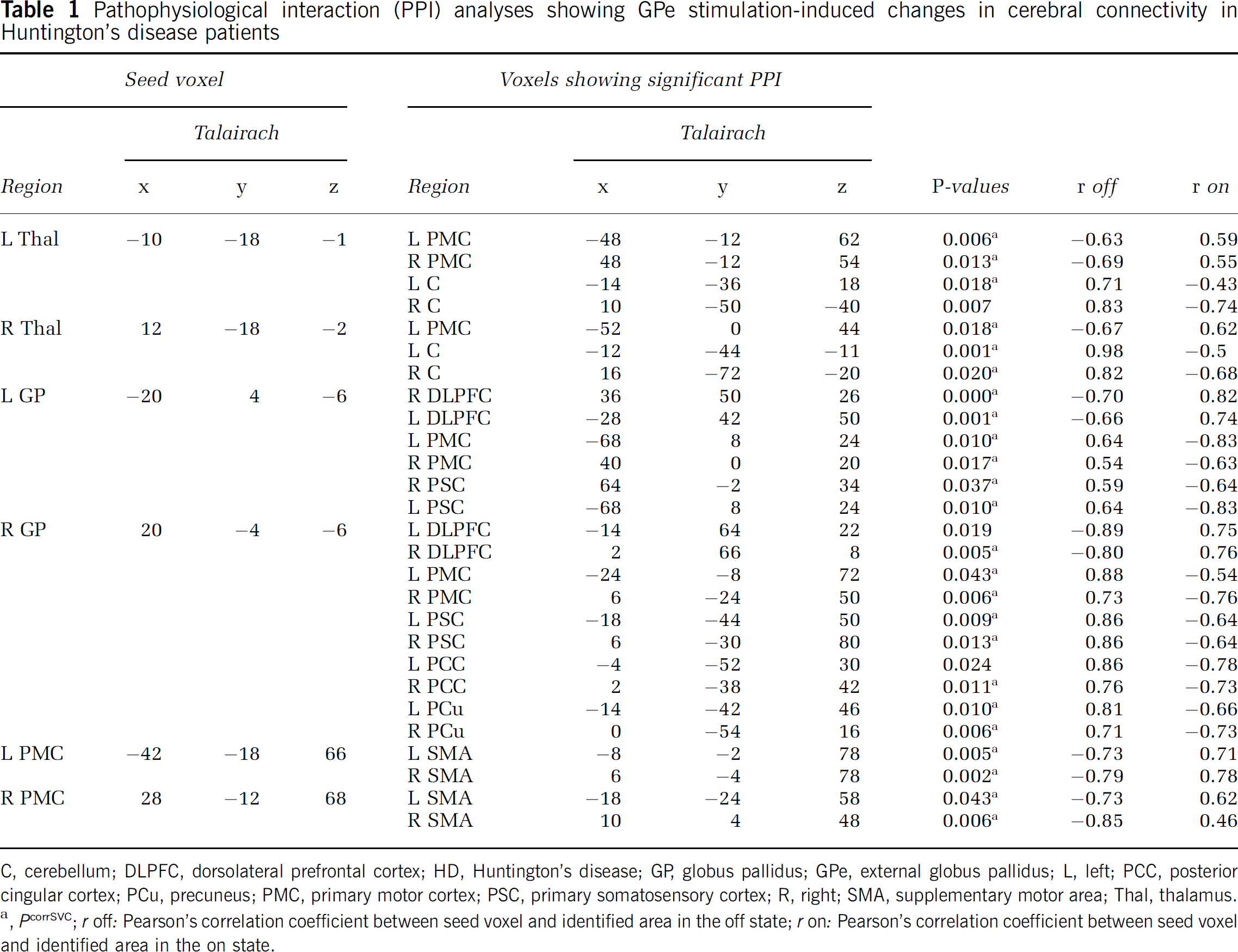
C, cerebellum; DLPFC, dorsolateral prefrontal cortex; HD, Huntington's disease; GP, globus pallidus; GPe, external globus pallidus; L, left; PCC, posterior cingular cortex; PCu, precuneus; PMC, primary motor cortex; PSC, primary somatosensory cortex; R, right; SMA, supplementary motor area; Thal, thalamus.
a
,
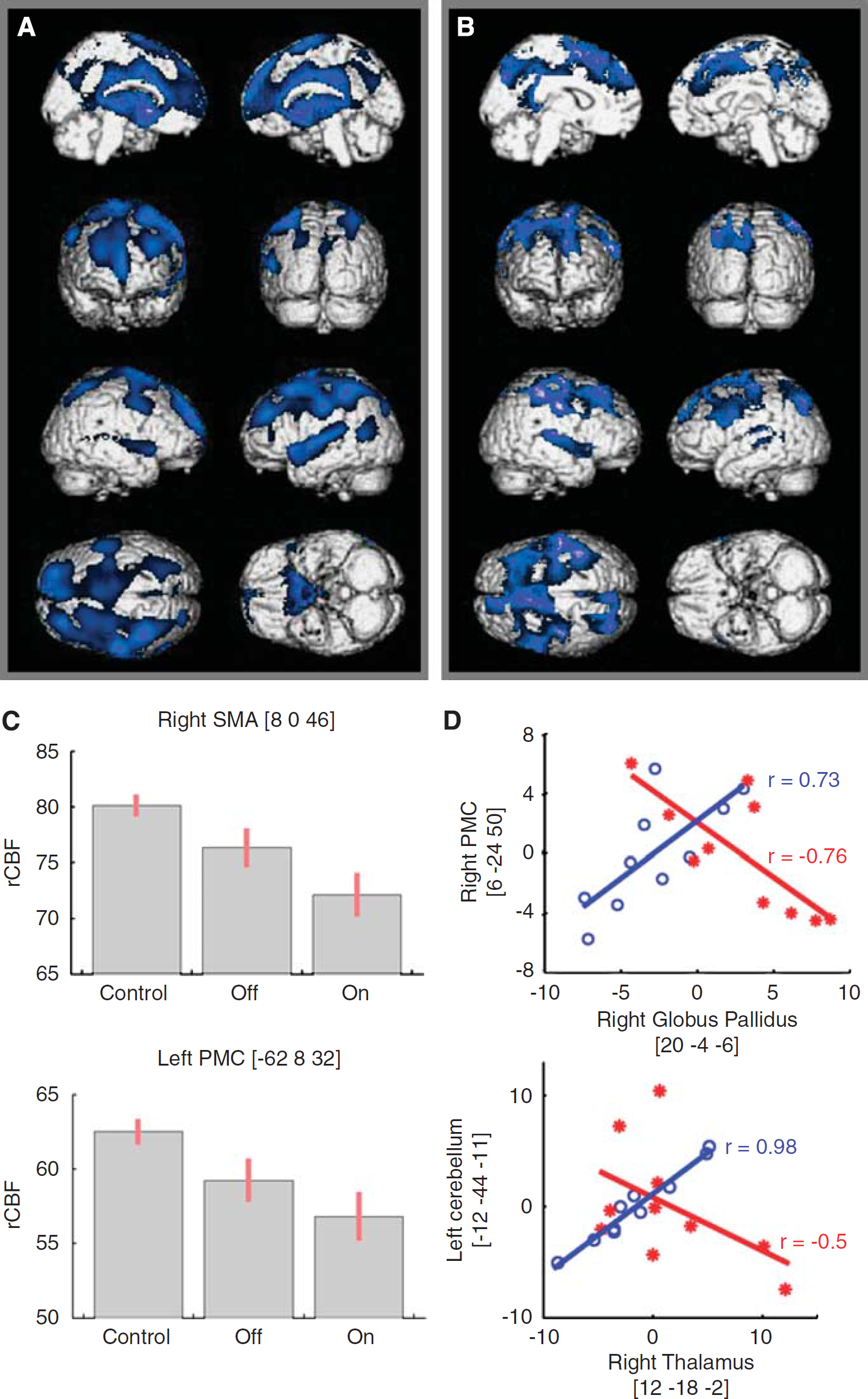
Regional cerebral blood flow and effective connectivity changes induced by GPe stimulation in patients with Huntington's disease. (
Pathophysiological interaction analyses using GP seed voxels showed significant GPe-DBS-induced changes in effective connectivity with the dorsolateral prefrontal cortices and primary sensori-motor cortices bilaterally (Figure 1D). Moreover, with the seed voxel in the right GP, PPI analyses additionally disclosed a significant change in effective connectivity with PCC and precuneus bilaterally. Indeed, GPe-DBS reversed the correlation directionality between GP and dorsolateral prefrontal cortices from negative in the off state to positive in the on state, and conversely, for GP and primary sensori-motor cortices, PCC, and precuneus bilaterally (Table 1).
Pathophysiological interaction analyses using seed PMC seed voxels showed that GPe-DBS induced a significant change in effective connectivity with supplementary motor areas bilaterally, with a correlation directionality reversal from negative in the off state to positive in the on state (Table 1).
Discussion
This neuroimaging study shows that GPe-DBS decreases neuronal activity in the resting state and modulates connectivity within the basal ganglia-thalamocortical circuits, the motor network, and the DMN in patients with HD.
With the brain stimulator switched off, patients showed widespread cortico-subcortical rCBF decrease, with an anatomic distribution concordant with previous studies on HD patients (Weeks et al, 1997). Further rCBF decrease induced by GPe-DBS in the sensori-motor network, the anterior cingulate cortex, and the prefrontal regions is in line with the standard model of the basal ganglia-thalamocortical circuits that drove the choice of GPe as a site of therapeutic electrostimulation in HD (Alexander et al, 1986; DeLong, 2000). Thus, this imaging study in HD patients substantiates the physiologic model of the basal ganglia. Moreover, GPe-DBS modulates cerebral connectivity involving three major nodes of the basal ganglia-thalamocortical circuits, namely the thalamus, GPe, and PMC. This modulation leads to a connectivity pattern consistent with the standard model of the basal ganglia-thalamocortical circuits and data obtained in healthy subjects using PET or functional magnetic resonance imaging (Di Martino et al, 2008; Kim et al, 2009; Postuma and Dagher, 2006). These changes in effective connectivity observed in the on state provide some insight into the rCBF decrease found in brain regions under the indirect influence of GPe activity. They further support the choice of GPe as a therapeutic target for inhibitory DBS in HD. Neurologic confirmation within the framework of our clinical trial is required to confirm the actual value of such a therapeutic strategy.
Whatever the state of the stimulator, we found increased cerebellar rCBF, which might be attributed to the normalization process, highlighting variations relative to global cerebral perfusion. Indeed, a diffuse reduction of activity in the cerebral hemispheres, relative to the cerebellum, is expected in HD. Although this normalization effect imposes caution in the interpretation of effective connectivity changes with the cerebellum, it can hardly account for the observed inversion of the correlation between the thalami and the cerebellum from the off to the on state in HD patients. It must be noted that the connectivity pattern found between these structures is in line both with their established anatomic relationship within the cerebello-thalamo-cortical pathway and with a recent connectivity study on this pathway (Krienen and Buckner, 2009).
The DMN is defined as a set of brain regions that manifest greater activity during resting states as compared with goal-directed behaviors. This network prominently includes frontal regions along the midline, lateral, and medial parietal regions extending into the posterior cingulate and retrosplenial cortex, and the medial temporal lobes (Gusnard and Raichle, 2001). Here, we found in the HD framework that GPe-DBS decreased neuronal activity in the PCC and the precuneus that are part of the DMN, in line with previous reports of connectivity between nodes of the basal ganglia-thalamocortical circuitry and the DMN in healthy subjects (Cavanna and Trimble, 2006; Gusnard and Raichle, 2001; Marchand et al, 2007). Moreover, changes in effective connectivity observed between GPe and both PCC and precuneus during GPe stimulation further support some degree of functional integration between these major networks (Marchand et al, 2007). These findings indicate that GPe-DBS effects in HD might extend beyond the motor pathways.
In conclusion, this neuroimaging study provides neurophysiological evidences supporting GPe as a therapeutic target for DBS strategies in HD.
Footnotes
Acknowledgements
Noémie Ligot is ‘clinicien chercheur doctorant’ and Xavier De Tiège is ‘clinicien chercheur spécialiste’ at the ‘Fonds de Recherche Scientifique’ (FRS-FNRS, Belgium).
The authors declare no conflict of interest.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.