
Abstract
Superparamagnetic iron oxide nanoparticles have diverse diagnostic and potential therapeutic applications in the central nervous system (CNS). They are useful as magnetic resonance imaging (MRI) contrast agents to evaluate: areas of blood–brain barrier (BBB) dysfunction related to tumors and other neuroinflammatory pathologies, the cerebrovasculature using perfusion-weighted MRI sequences, and
Keywords
Introduction
The diagnosis and treatment of pathologies that affect the central nervous system (CNS) are currently undergoing a renaissance because of the marked proliferation of ‘nanoscale’ technologies. Nanotechnology, as it relates to biomedicine, can broadly be defined as ‘nano-sized structures that contain at least one dimension between 1 to 100 nm in size … and possess new or enhanced properties that are unattainable at both smaller (quantum) [and] larger (macromolecular) levels’ (Hartman et al, 2008).
Superparamagnetic iron oxide nanoparticles are based on magnetite (Fe3O4), which has received the most attention for biomedical applications, or maghemite (γFe2O3) molecules encased in polysaccharide, synthetic polymers, or monomer coatings (Laurent et al, 2008; Thorek et al, 2006). The utility of superparamagnetic iron oxides as magnetic resonance imaging (MRI) contrast agents has been studied for more than two decades (Weissleder et al, 1990) and the list of available agents is rapidly expanding (Table 1). These particles can be organized according to their hydrodynamic diameter into several categories (Corot et al, 2006): standard superparamagnetic iron oxide particles (SPIOs) (50 to 180 nm), ultrasmall superparamagnetic iron oxide particles (USPIOs) (10 to 50 nm), and very small superparamagnetic iron oxide particles (VSPIOs) (< 10 nm). Most contemporary investigations use USPIOs; therefore, for the sake of consistency we will refer to superparamagnetic iron oxide nanoparticles, in general, as USPIOs unless specifically discussing SPIOs or VSPIOs.
Available superparamagnetic iron oxide agents and prohance (Gd-based agent) for comparison
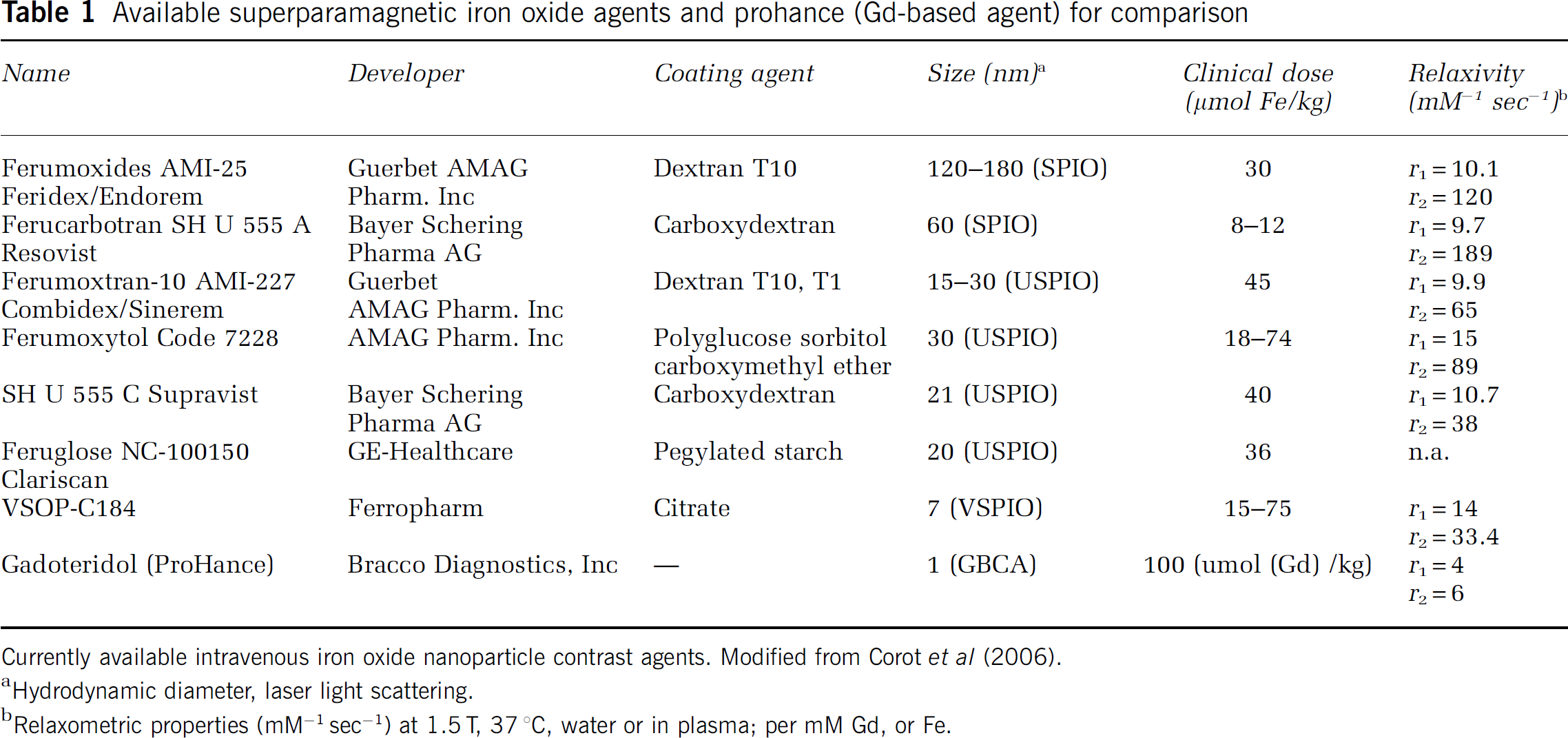
Currently available intravenous iron oxide nanoparticle contrast agents. Modified from Corot et al (2006).
Hydrodynamic diameter, laser light scattering.
Relaxometric properties (mM−1sec−1) at 1.5T, 37 °C, water or in plasma; per mM Gd, or Fe.
Particles of iron oxide have been administered intravenously (IV) for over 50 years, initially for the treatment of anemia (Cameron et al, 1951). Emerging experimental and clinical applications in the CNS capitalize on both the physical and magnetic properties of iron oxide nanoparticles; the list of biomedical imaging applications for these nanoparticles continues to expand. There are a number of important qualities of USPIOs that make them attractive as complimentary or alternative MRI contrast agents compared with gadolinium-based contrast agents (GBCAs). These can be summarized as follows: USPIOs are virus-sized molecules with a very long circulating half-life (∼14h for ferumoxytol); USPIOs are avidly taken up by phagocytic cells such as the Kupffer cell fraction of the liver, circulating monocytes/macrophages and mononuclear T cells, as well as reactive astrocytes, microglia, and dendritic cells within the brain. Neutrophils have not been found to take up USPIO. The USPIOs are cleared from the circulation primarily by the reticuloendothelial system (Bourrinet et al, 2006); these properties (i.e., degree of cellular labeling and rate of clearance) are dependent on size, coating, and method of delivery and will be discussed in detail below. Limitations of these agents for current CNS imaging applications are primarily related to the inability to reliably differentiate USPIO signal from resident brain iron signal (i.e., in the setting of hemorrhage related to stroke or trauma). There are also very little data in humans regarding the long-term clearance of these agents from the brain.
Ferumoxides (Endorem, Guerbet in Europe; Feridex, AMAG Pharmaceuticals Inc in the USA and Japan) and ferucarbotran (Resovist, Schering Bayer in Europe and Japan) are commercially available SPIOs approved for MR imaging of liver tumors (Ros et al, 1995). Clinical CNS imaging studies have also been performed with these compounds (Rose et al, 2006; Varallyay et al, 2002). The USPIO, ferumoxytol (Feraheme, AMAG Pharmaceuticals Inc, Cambridge MA, USA) is approved for iron-replacement therapy in patients with chronic renal failure (Kidney Daily, 6/30/2009). Ferumoxtran-10 (Manninger et al, 2005; Saleh et al, 2007), SHU555C (Vellinga et al, 2008), and ferumoxytol (Neuwelt et al, 2007) have been investigated in humans for various CNS imaging applications. Preliminary studies using ferumoxides, ferumoxtran-10 (Combidex), and ferumoxytol have not revealed significant toxicities (Muldoon et al, 2006; Neuwelt et al, 2007). Ferumoxytol, in particular, is attractive as an MRI contrast agent because it can be given as a bolus for first-pass perfusion imaging and appears to be safe in patients with chronic kidney disease; at later time points (i.e., 24 h), ferumoxytol accumulation is evident in areas of blood–brain barrier (BBB) dysfunction that may be fundamentally related to inflammation from any cause.
This review will focus primarily on USPIOs, specifically ferumoxtran-10 and ferumoxytol, for diagnostic applications in the CNS with an emphasis on their utility as MRI contrast agents in the setting of CNS tumors. It will also highlight the utility of USPIOs for imaging tumor neovasculature and assessing therapeutic response to antiangiogenic chemotherapeutic agents.
Basic science review
Ultrasmall Superparamagnetic Iron Oxide Particle Synthesis and Pharmacology
The most common methods of USPIO synthesis for biomedical applications are coprecipitation of ferric and ferrous salts in an alkaline medium, with or without surface complexing agents such as dextran or polyethylene glycol, or microemulsion techniques with small amounts of iron ions trapped inside surfactant bubbles in an oil medium (Hartman et al, 2008; Laurent et al, 2008). The USPIOs consist of two components: an iron oxide core and a hydrophilic coating. It is the combination of these two components that determines their pharmacology. Passive targeting is perhaps most dependent on the hydrodynamic radius and the surface charge (factors related to the coating material), as these characteristics determine circulation time, accessibility to tissues, opsonization, and rate of cell-type uptake (Thorek et al, 2006). Active targeting in the CNS takes advantage of nanoparticle surface modifications (e.g., the addition of monoclonal antibodies or peptides) such as chlorotoxin, for glioma imaging. Current clinical trials primarily involve passive targeting.
With respect to passive targeting, USPIOs behave differently than GBCAs for a number of reasons. First, because of their larger molecular size—up to 50 nm (compared with the 1 nm gadolinium chelate), USPIOs extravasate much more slowly than standard GBCA, even in areas of severe BBB dysfunction (i.e., malignant glioma). Most GBCAs, in comparison, rapidly extravasate into the extravascular space in areas of BBB dysfunction and are rapidly cleared from the circulation via the kidneys. There are numerous formulations based on the gadolinium ion [Gd(III)], each with unique properties and safety profiles (Harpur et al, 1993).
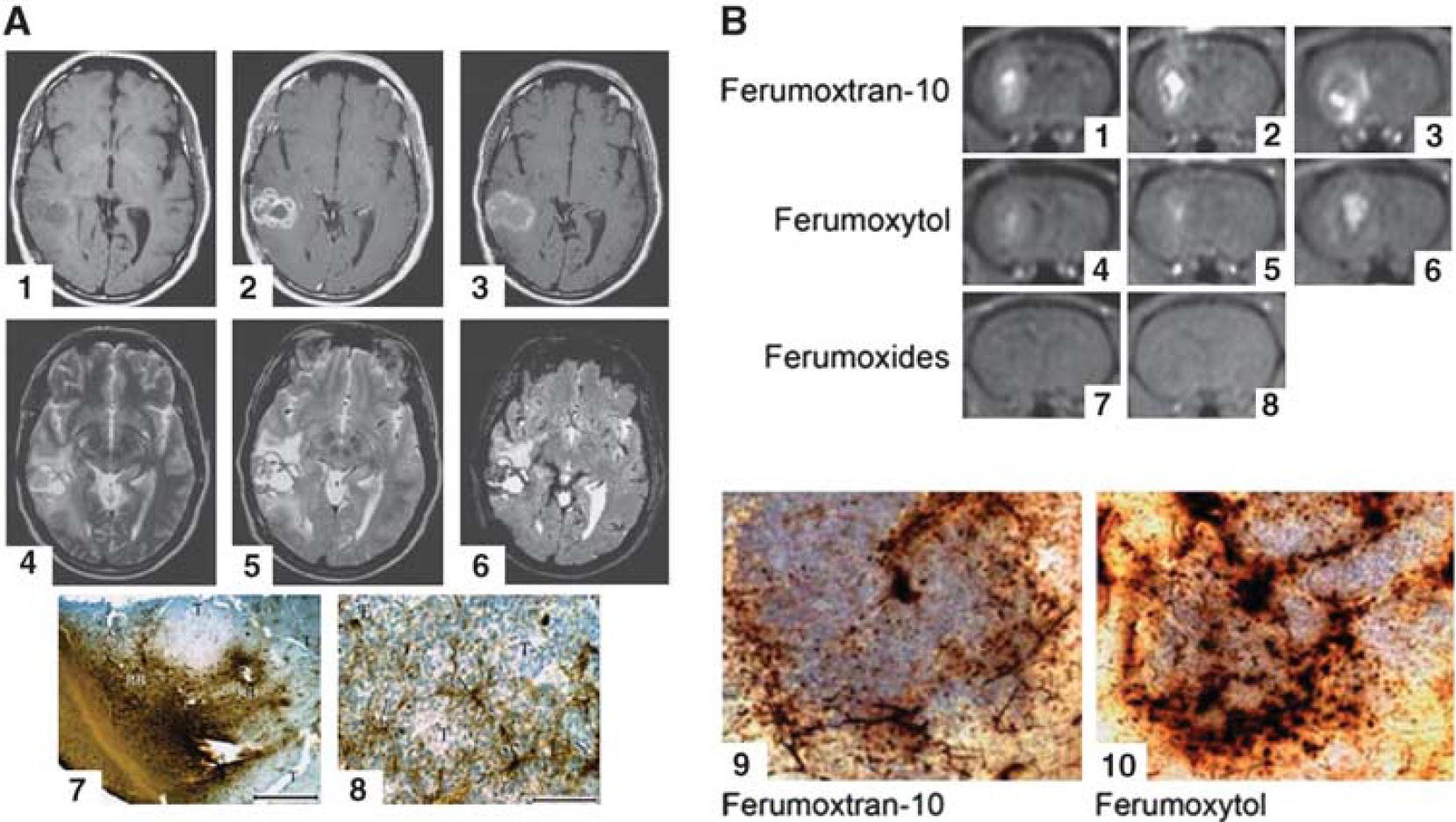
Ferumoxtran-10 is a first-generation USPIO that may have a slight advantage over ferumoxtyol for anatomic imaging of inflammatory lesions; however, it is not safe for angiographic imaging procedures, which require a rapid infusion. Ferumoxytol was developed as an IV iron-replacement therapy, specifically for anemic patients with chronic kidney disease; after bolus IV administration, it follows a useful distribution that is conceptionally based on the conservation of mass. Over time, a combination of events occur leading to contrast enhancement: USPIOs slowly leak across the BBB (mechanism incompletely understood); there may also be uptake of USPIO by circulating monocytes/macrophage, which then cross the BBB in response to inflammation and injury. Histologic samples from resected brain tumors of patients, who received USPIOs, reveal that part of the extravasated iron oxide particles are taken up by parenchymal cells. Thus, their localization is both intracellular and interstitial (Figure 1A) (Varallyay et al, 2002).
(
Measurable T1-weighted signal enhancement (hyperintensity) in brain tumors is seen as early as 4 to 6h after USPIO injection; contrast enhancement intensity peaks ∼24h after injection and can generally be visualized even 72h after injection, although it is usually faint and more diffuse (Neuwelt et al, 2007). In contrast to GBCAs, there is no renal elimination of USPIO, which accounts for the enhanced safety profile in patients with renal dysfunction who appear to be at increased risk for contrast-induced nephropathy or nephrogenic systemic fibrosis (Neuwelt et al, 2008).
Unlike USPIOs, the plasma half-life of SPIOs is on the order of minutes. This is due to their larger particle size (>50 nm) and negative surface charge, which lead to rapid elimination. Iron-loaded mononuclear cells can actively cross a relatively intact BBB in cases of an active inflammatory process (Oude Engberink et al, 2007), but because of their large size, SPIOs do not leak across BBB defects like free USPIOs (as in malignant gliomas). In the clinical setting, FDA-approved doses of ferumoxides (SPIOs) were given to 20 patients with intrinsic or metastatic brain tumors. No enhancement was visualized in any patient at 30 mins or 4 h (Varallyay et al, 2002).
The safety profile of clinically useful USPIOs varies based on their molecular structure. After cellular internalization, iron oxide nanoparticles accumulate in lysosomes in which the low pH breaks the iron oxide core down into iron ions. These ions are then incorporated back into the hemoglobin pool (Thorek et al, 2006). The type of coating used has a significant impact on the immunologic response to USPIOs; to date, studies have shown that polymer-coated nanoparticles have minimal impact on cell viability and function (Bourrinet et al, 2006; Thorek et al, 2006). Trypan blue exclusion-based toxicity studies, using high concentrations of USPIOs, show good tolerance with minimal cell death. However, there have been reports of free radical generation, decreased cell proliferation, and even cell death with some formulations, highlighting the uniqueness of different nanoparticle configurations (Modo et al, 2005). Whereas earlier agents, such as ferumoxtran-10, were administered via slow infusion to avoid mast cell degranulation, newer agents, such as SHU 555 C and ferumoxytol can be safely given as a rapid IV bolus.
Ferumoxytol has been tested as an iron supplement therapy in patients with renal failure up to the dose of 510 mg (Landry et al, 2005; Spinowitz et al, 2005). For MRI contrast agent applications, the amount of iron administered (typically < 4 mg/kg) is much lower than doses resulting in acute systemic toxicity (above 60 mg/kg) or chronic iron overload (above 20g stored iron). Over 1700 patients have received ferumoxytol in its clinical development program, and at least 1500 of these were patients with chronic kidney disease in Phase 3 iron-replacement studies. To date, only one patient, with a history of multiple drug allergies, has experienced an anaphylactoid reaction (hot flashes and itching, without respiratory compromise) and severe hypotension a few minutes after receiving ferumoxytol. There have been no deaths that were considered to be related to ferumoxytol treatment (Neuwelt et al, 2008). The long-term fate of iron from ferumoxytol in the brain remains unknown, however. There is growing evidence that iron accumulation in the brain, as in nigrostriatal dopaminergic neurons associated with Parkinson's disease for example, is not merely an epiphenomenon but a result of misregulation of iron homeostasis within the brain (Ke and Ming Qian, 2003). Preclinical studies of USPIOs injected directly into the rat brain, or delivered transvascularly, have not revealed any acute or midterm toxicity. As early as 7 days after transvascular delivery of ferumoxytol, no iron was detectable in the brain using MRI and histology (Muldoon et al, 2005). After direct intracerebral injection of USPIO or SPIO, iron was still easily detected in brain parenchyma by MRI and histology, with no sign of pathology at 3 months.
Magnetic Resonance Imaging Physics
Magnetic resonance imaging is a noninvasive technique that uses magnetic fields to produce high resolution and high-contrast images of tissue structure and function. The principal tissue signal of interest in essentially all clinical MRI arises from water protons. Water concentration can vary significantly between biological tissues and this property is exploited to produce a fundamental contrast in MRI that is known as ‘proton density contrast’. In proton density-weighted MRI, the signal intensity of each voxel is proportional to the local proton concentration. Another fundamental class of MRI contrast relies on spatial differences in the relaxation properties of the MR signal.
There are two principal relaxation processes that characterize MR signals, one that relates how rapidly magnetization parallel to the strong static magnetic field recovers after a perturbation, and the other that describes how rapidly magnetization transverse to the static magnetic field decays after it has been produced by a series of radiofrequency pulses. The constants that characterize these two kinetic processes are referred to as longitudinal and transverse relaxation time constants, T1, and T2, respectively. In general, T1 relaxation processes are sensitive to fluctuating magnetic fields at or about the MRI operational frequency (i.e., the Larmor frequency). Transverse relaxation processes are sensitive to magnetic fields that fluctuate at the Larmor frequency, but also are significantly determined by fluctuations at low frequency. In complex samples such as tissues, the ‘density’ of low-frequency fluctuating fields is much greater than those at or near the Larmor frequency. This is why 1H2O T2 values are typically much smaller than T1 values in tissue. An apparent transverse relaxation time constant (T2*) can also be defined. In addition to contributions from T2 mechanisms, T2* relaxation processes are sensitive to microscopic magnetic field distributions. Such magnetic field distributions can be produced by compartmental differences in magnetic susceptibility, such as occurs in areas proximal to blood vessels with significant deoxyhemoglobin concentration and is exploited in functional MRI experiments. Therefore, T2* values are always smaller than T2 values.
For most MRI studies, the intrinsic contrast provided by spatial differences in proton density and relaxation times is sufficient. However, it is important to appreciate that most MRI acquisitions, although strongly weighted to a particular type of contrast, are invariably sensitive to more than one type of contrast. The amount of mixed weighting in an MRI acquisition depends on a number of factors, but becomes important when discussing contrast agent applications.
Magnetic Resonance Imaging Contrast Agents
Although intrinsic contrast is sufficient for most MRI applications, exogenous contrast agents are used in ∼40% of all clinical MRI studies. Typically, these agents are used to increase lesion conspicuity and to improve characterization of blood vessels. Unlike tracers used in x-ray or nuclear medicine imaging, MRI contrast agents are detected indirectly through their ability to catalyze water proton relaxation and perturb MRI signal intensity. By far, the most widely used MRI contrast agents are those based on the paramagnetic gadolinium [Gd(III)] ion. The Gd(III) ion has seven unpaired electrons and favorable electronic spin relaxation properties that make for very efficient catalysis of water proton relaxation. The Gd(III) ion is chelated to a low-molecular weight ligand to reduce toxicity. These low-molecular weight GBCAs are injected IV, most will distribute rapidly into all accessible extracellular spaces, and are eliminated from the body through the kidneys with a typical elimination half-life of ∼1.6h. Contrast agents catalyze relaxation rate constants (the inverse of the time constants described above) in a concentration-dependent manner. In simple solutions, the 1H2O T1−1 increases linearly with contrast agent concentration. The slope of this dependence is known as the relaxivity, typically reported in units of mmol−1 sec−1, and is a measure of how potent the agent is for catalyzing relaxation. Relaxivities typically differ for longitudinal and transverse relaxation and vary with magnetic field strength. The GBCAs typically are used in combination with T1-weighted MRI acquisitions and produce a hyperintense (bright) signal in tissue regions in which the agent accumulates. The low-molecular weight and weak protein binding characteristics of most GBCAs lead to avid extravasation of GBCAs from normal blood vessels in most tissue and abnormal blood vessels in the CNS. These agents have found widespread use for investigations of blood–CNS barrier disruption found in many disease pathologies.
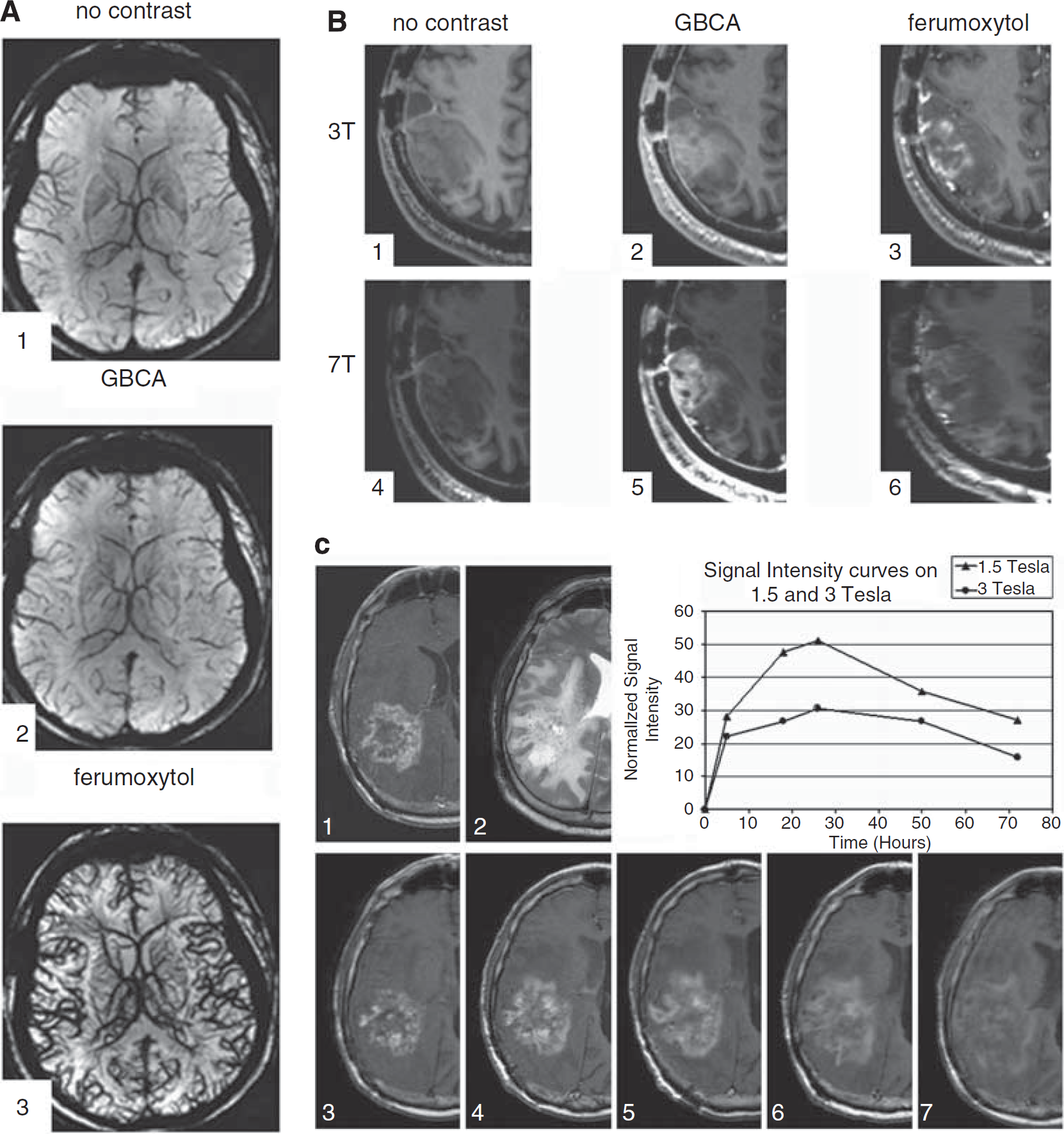
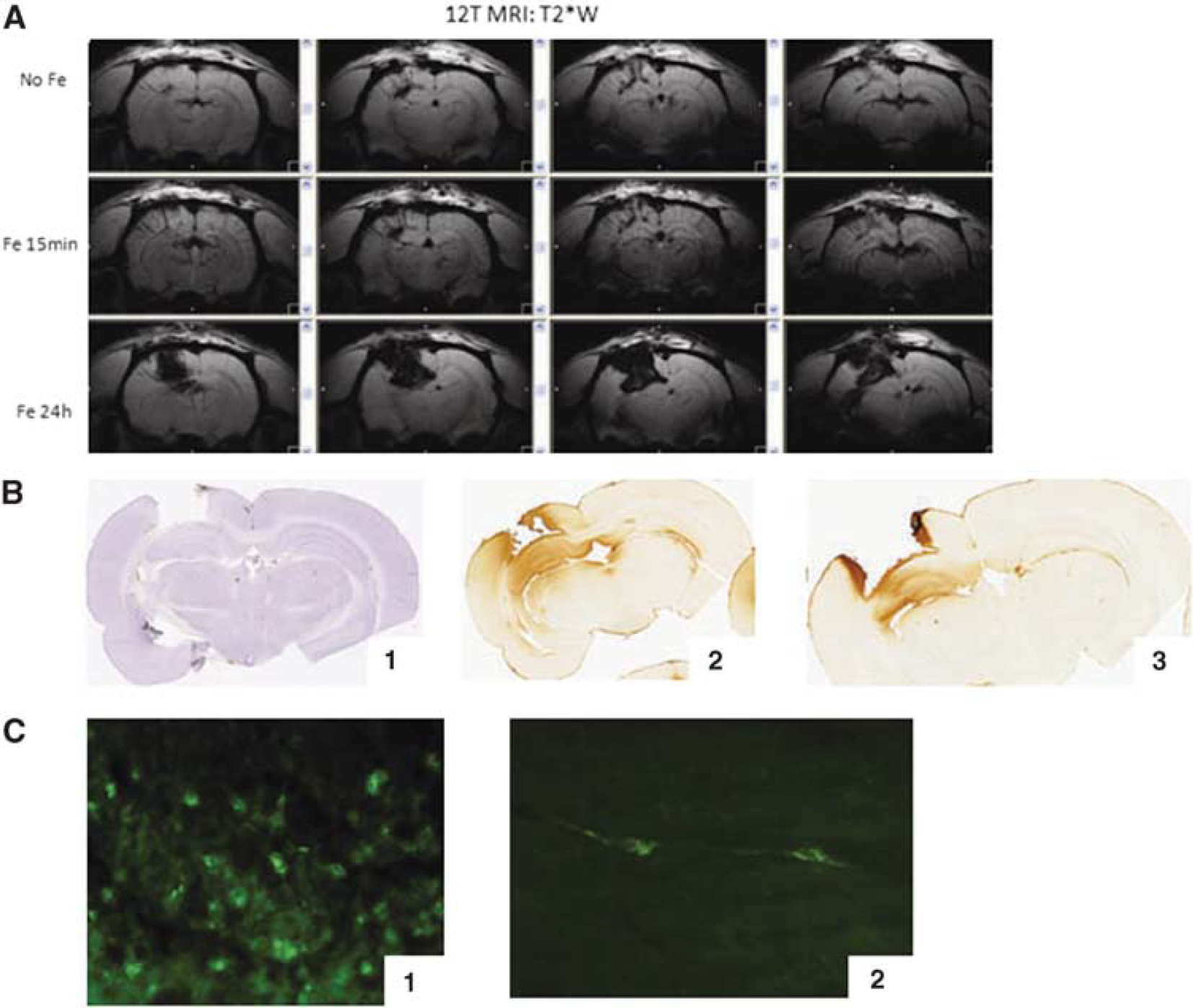
The USPIOs are based on magnetite (Fe3O4) nanocrystals and are classified as superparamagnetic compounds because the net magnetic dipole moment realized exceeds that expected from the unpaired [Fe(II), Fe(III)] electrons alone. Like GBCAs, the USPIOs do not retain any net magnetism once removed from the strong magnetic field; thermal energy is sufficient to destroy the net magnetic order within the nanocrystal established by the strong magnetic field. The USPIOs have excellent relaxivities and on a per iron-atom basis compare very favorably with GBCAs (Table 1). Unlike the GBCAs, which have similar transverse and longitudinal relaxivities at clinically relevant magnetic fields, the USPIOs have significantly greater transverse relaxivities compared with longitudinal relaxivities (Table 1). Thus, USPIOs tend to find greater application on magnetic susceptibility-based acquisitions in T2-weighted or T2*-weighted MRI, in which they produce a hypointense (dark) signal (Figure 2A). The strong magnetic susceptibilities of these compounds can result in a significant distribution of microscopic magnetic fields and severe MR signal quenching. This can be appreciated in Figure 2A that compares minimum intensity projection susceptibility-weighted images obtained without exogeneous contrast, with a standard dose GBCA, and with 4 mg/kg ferumoxytol. The image collected after ferumoxytol shows significantly greater MR signal quenching (hypointensity) in areas in and surrounding blood vessels than either the GBCA or no exogeneous contrast agent conditions. Nevertheless, USPIOs do have significant longitudinal relaxivities and have been used as agents in T1-weighted and even dynamic contrast-enhanced acquisitions, in which tissue regions that accumulate the agent appear hyperintense. It should be noted that the transverse relaxivities increase supralinearly with magnetic field strength, whereas the longitudinal relaxivities typically decrease slightly (Blockley et al, 2008). Therefore, the hyperintense T1-weighted enhancement is more readily achieved at lower magnetic field strengths and the potential for mixed weighting effects in USPIO-based MRI applications increases markedly with magnetic field strength (Muldoon et al, 2005; Neuwelt et al, 1994). Comparing postcontrast T1-enhancement at 3T and 7T in the same subject at similar times reveals improved sensitivity for GBCA detection but reduced sensitivity for USPIO detection at 7 T (Figure 2B). The observation of increasing GBCA detection sensitivity with magnetic field is consistent with predictions based on increased nominal brain tissue T1 relaxation time constants with increasing magnetic field (Rooney et al, 2007). Increased nominal T1 values imparts increased sensitivity for detecting lower concentration of GBCA despite a slight decrease in longitudinal relaxivity and increase in transverse relaxivity with increasing magnetic field (Chang et al, 1994; Rohrer et al, 2005).
(
Generally, the
Diagnostic and potential therapeutic applications
Imaging Central Nervous System Tumors with Ultrasmall Superparamagnetic Iron Oxide Particles
There are ∼16,900 new cases of primary CNS tumors diagnosed in the United States each year. Contrast-enhanced MRI of CNS malignancies is a crucial diagnostic tool and a key parameter for follow-up imaging of tumor response to therapy (Macdonald et al, 1990). Enhancement of residual or recurrent tumors using standard GBCAs reflect both cerebral blood flow (CBF) and alterations in the BBB appearing as increased signal on T1-weighted images within minutes after injection (Akeson et al, 1997). Unlike GBCAs, USPIO enhancement at early time points after administration is not a clear marker of BBB deficiency. The mechanism of USPIO tissue accumulation is not fully understood but is likely related to its prolonged circulation time and as a cellular label following uptake by inflammatory cells within and around tumors. For CNS tumor imaging, T1-weighted scans have proven to be superior for the evaluation of low concentrations of iron oxide nanoparticles traversing the BBB (Muldoon et al, 2005; Neuwelt et al, 1994; Varallyay et al, 2002). But as discussed above, this observation is dependent on details of the MRI acquisition including the magnetic field strength.
The BBB is a special feature of CNS capillaries that results from a continuous layer of endothelial cells bound together with tight junctions that allow very little transcellular or pericellular transport of blood borne molecules (Banks, 1999). Micrometastases that lack neovascularity remain protected by the BBB and may be undetectable using GBCAs. In contrast to the normal BBB, the blood–tumor barrier (BTB) may be highly permeable and allows conventional contrast agents to leak from the vessels into the perivascular space (Groothuis et al, 1991; Long, 1979). The permeability of the BTB may be variable not only in different histologic types of tumors but also within one tumor mass (Barnett et al, 1995; Kraemer et al, 2001; Kroll and Neuwelt, 1998; Varallyay et al, 2002), increasing the difficulty of accurately determining tumor size and type. Furthermore, any of a variety of inflammatory or infectious CNS lesions may show similar patterns of GBCA enhancement complicating the differential diagnosis (Enochs et al, 1999).
The USPIOs, which can be used both as intravascular contrast agents and as a cellular imaging agent, may be useful in the reduction of the above-mentioned problems (Corot et al, 2004). In animal studies, ferumoxtran-10 shows slightly better tumor imaging at the same dose as ferumoxytol; however, it must be administered over ∼30 mins to limit adverse reactions (Figure 1B) (Neuwelt et al, 2004). Enhancement after IV infusion of ferumoxtran-10 increases slowly and peaks at ∼24h after administration; then declines during the next several days (Figure 2C) (Manninger et al, 2005; Neuwelt et al, 2004; Varallyay et al, 2002). Indeed, after resection, our group found that residual lesions were still readily visible on the T1-weighted postoperative MRI at 48h. This property of ferumoxtran-10 allows for assessment of residual tumor without the need to re-administer a contrast material during intraoperative MRI (0.15T) or on postoperative MRI (Hunt et al, 2005). In additional clinical trials, three patients with glioblastoma multiforme (GBM) who received earlier radiation showed fewer areas of enhancement with ferumoxytol than with GBCA. When compared with ferumoxtran-10, ferumoxytol seemed to provide somewhat less enhancement. In another study, 6 out of 14 patients with GBM had MRIs, which revealed more intense enhancement with ferumoxtran-10 than with GBCA, whereas our group found 1 patient out of 5 with GBM had an MRI showing slightly increased enhancement with ferumoxytol versus GBCA (Neuwelt et al, 2007).
In an attempt to improve diagnostic specificity, multifunctional modifications are increasingly used to more specifically target USPIOs to the intended target. One example of this involves attachment of chlorotoxin, a 4-kDa peptide purified from the
Early clinical applications of USPIOs as MRI contrast agents focused on investigations of blood–CNS barrier breakdown in neuroinflammation and neoplasm. More recently, these agents have found widespread use in dynamic MRI examinations, including dynamic susceptibility contrast (DSC). The DSC techniques are useful for quantifying tissue perfusion (blood volume and blood flow) and are accomplished with time-series T2*-weighted MRI data that are collected during the bolus administration of a contrast agent. Dynamic contrast enhancement measurements are collected using a T1-weighted MRI time series, and are useful for quantifying contrast agent's vascular permeability and tissue distribution volumes. Early experimental data suggest that the combination of GBCA-enhanced T1-weighted MRI and USPIO-enhanced T2-weighted MRI reveals complimentary information in patients with CNS tumors (Neuwelt et al, 2007).
Perfusion-weighted imaging (PWI) is generally performed using first-pass, dynamic susceptibility-weighted contrast-enhanced (DSC) MRI echo-planar imaging approaches (Cha et al, 2002). The basic principle of PWI using DSC MRI is as follows: the first-pass effect of a contrast bolus in brain tissue is monitored using a series of T2*-weighted MR images from the same brain regions, which are scanned repeatedly. The susceptibility effect of a paramagnetic (GBCA) or superparamagnetic (USPIO) contrast agent causes signal loss that can be converted into a contrast agent concentration (Essig et al, 2006).
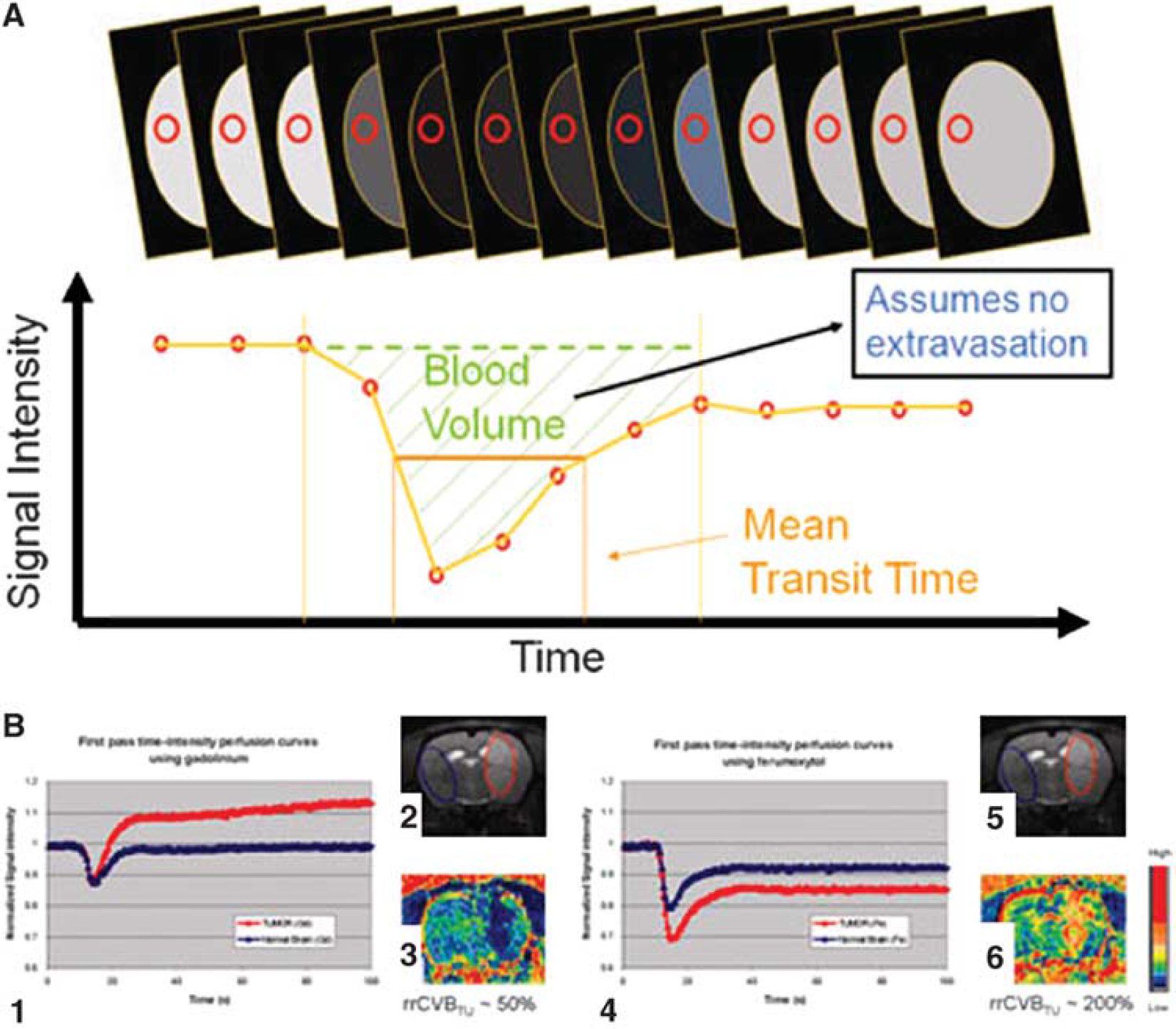
From these data, parametric maps of CBF, cerebral blood volume (CBV), and mean transit time (MTT = CBV/CBF) are calculated in regions of interest (Ostergaard, 2005). The CBF can be defined as the amount of blood delivered to a standard volume of brain per unit time, such as 50 mL/100 gm/mins in gray matter. The CBV is the amount of blood per volume of brain or pathologic lesion. The MTT refers to the time it takes for a bolus of contrast to pass through a region of tissue; it can be calculated by comparing a signal washout curve in the region of interest with the contrast signal in a cerebral artery (Figure 3A). These data parameters, alone or in combination, provide information on cerebral hemodynamics and serve as surrogates to quantify angiogenesis. The USPIOs may provide more accurate measurements of these vascular parameters, compared with GBCAs, because of their propensity to remain intravascular at early time points (Figure 3B).
(
Molecular Imaging of Inflammation with Ultrasmall Superparamagnetic Iron Oxide Particles
Molecular imaging is an important new diagnostic tool for studying
Phagocytic cellular uptake of iron oxides increases with particle size (Daldrup-Link et al, 2003; Matuszewski et al, 2005). SPIOs, with a hydrodynamic diameter of 50 to 180 nm, are more efficiently phagocytosed than USPIOs with sizes of 20 to 50 nm. The maximum intracellular iron oxide concentration of
With respect to contrast-enhancement imaging properties of CNS tumors, besides their vascularity, the number and the distribution of activated inflammatory cells seems to be the most relevant. A large number of macrophages and activated microglia have been reported to be present within and around malignant brain tumors. The microglial infiltration is typically most prominent at the periphery of a lesion and in the surrounding brain tissue. The ability to track USPIO-labeled cells using MRI and then correlate them with histology is an important new technology in the investigation of many CNS pathologies. Our group has tracked ferumoxtran-10 from brain into the cervical lymph nodes of rats (Muldoon et al, 2004). This connection has not been well characterized in humans, but may be implicated in the pathogenesis of diseases such as multiple sclerosis (MS) and Alzheimer's disease through peripheral immune responses to CNS proteins.
Fleige
In another study, fragments of human malignant glioma were orthotopically xenografted into the brains of nude mice. All mice underwent MRI examination 24h after IV administration of ferumoxtran-10. In this study, Kremer
Monitoring Antiangiogenic Therapy in Central Nervous System Tumors with Ultrasmall Superparamagnetic Iron Oxide Particles
The blockade of neoangiogenic signaling pathways is one of the several key strategies in the treatment of high-grade malignant brain tumors. Bevacizumab, which neutralizes the vascular endothelial growth factor-A, is the most commonly used monoclonal antibody for the treatment of high-grade gliomas in humans (Claes et al, 2008). Growing evidence suggests that USPIO-enhanced MRI will be useful in the evaluation of tumor response to antiangiogenic therapy.
Claes
Ongoing clinical trials conducted by our group show that USPIOs, combined with PWI, are an important adjuvant for monitoring tumor response and for discrimination of pseudo-progression from true tumor progression. It is generally accepted that increased malignancy is associated with increased vascularity and tumor growth is correlated with neoangiogenesis. In CNS malignancies, CBV has been one of the most commonly used parameters to estimate microvascular density (Cha et al, 2002). However, in tumors with a disrupted BTB (such as malignant glioma) leakage of GBCAs from tumor vessels causes inaccurate estimation of tumor CBV using PWI (Figure 3B) (Neuwelt et al, 2007; Uematsu and Maeda, 2006). Although the clinical impact of this inaccuracy is not known, it could be significant in cases in which PWI is used to monitor therapeutic response to antiangiogenic chemotherapies, such as bevacizumab. In this scenario, the use of a blood-pool agent, such as the bolus-injectable USPIO ferumoxytol, would be favorable by eliminating the permeability dependence of CBV estimation (Figure 3B).
The evidence regarding CBV normalization and survival of patients with brain tumors is not straightforward, however. One clinical study involving 19 patients with grades 2, 3, and 4 gliomas revealed a stronger correlation of survival with normalized CBV than with intensity of GBCA enhancement (Lev et al, 2004). Another study investigating 28 patients with GBM found no significant relationship between median CBV and survival (Oh et al, 2004). However, one must consider that median CBV ignores the intrinsic heterogeneity of tumor perfusion (Aronen et al, 1994; Donahue et al, 2000; Knopp et al, 1999; Kremer et al, 2002; Lev et al, 2004; Sugahara et al, 1998). In 23 patients with high-grade gliomas, the fractional tumor volume of high CBV, which accounts for the heterogeneity of CBV, was analyzed before radiotherapy and it predicted survival. Subsequent changes in CBV during conformal radiotherapy were also predictive (Cao et al, 2006). More accurate CBV maps, generated using USPIOs, may also be useful in the evaluation of treatment response and helpful in the differentiation of recurrent tumor from postsurgical/postirradiation changes.
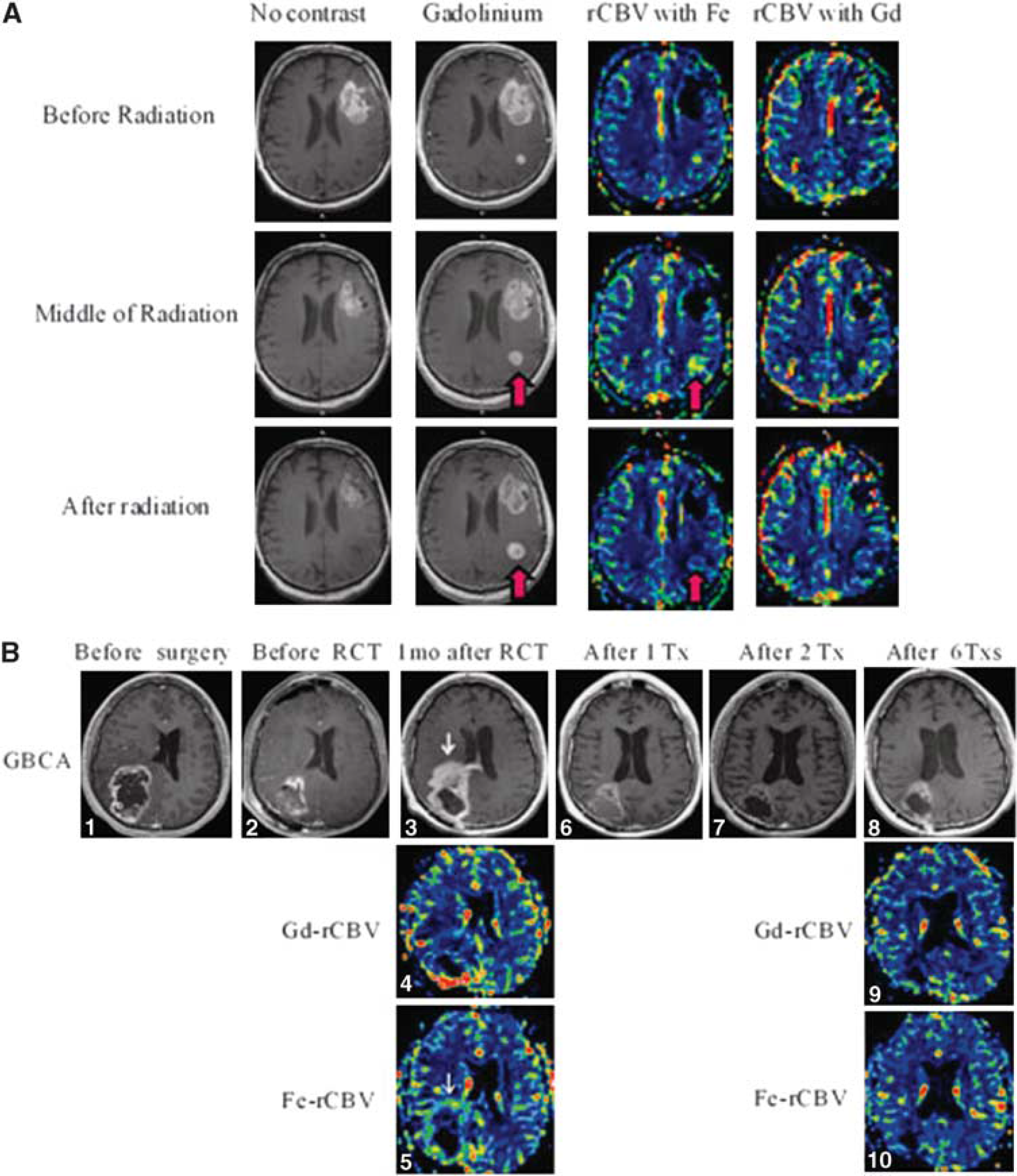
It is hypothesized that CBV measurements may provide a mechanism to distinguish pseudoprogression versus true progression of malignant gliomas after chemoradiotherapy using temozolomide. Up to 50% of patients treated with temozolomide have increased areas of GBCA enhancement in the first 3 months after completion of radiation (Brandsma et al, 2008). The PWI using blood-pool agents (USPIOs, such as ferumoxytol) may allow differentiation of true tumor progression from pseudoprogression based on increased versus decreased CBV, respectively (Figure 4) (unpublished data).
(
Imaging Stroke with Ultrasmall Superparamagnetic Iron Oxide Particles
Imaging ischemic CNS lesions is time dependent. In the past, parenchymal ischemic injury could only be detected 6 to 12h after the onset of symptoms using standard MRI sequences (Yuh et al, 1991). Diffusion- and perfusion-weighted MRI, using USPIOs or GBCAs, allows for the identification of ischemic lesions earlier and may permit the monitoring of the effects of therapeutic strategies (Chenevert et al, 1991; Moseley et al, 1990; Rosen et al, 1990; Stroke, 1989. Recommendations on stroke prevention, diagnosis, and therapy. Report of the WHO Task Force on Stroke and Other Cerebrovascular Disorders, 1989). Contrast agents that cause a regional signal loss because of magnetic susceptibility-induced T2* shortening (e.g., USPIOs) have been shown to provide substantial contrast between ischemic and normally perfused brain areas (Gore and Majumdar, 1990; Villringer et al, 1988). The MTT abnormalities, taken together with areas of restricted diffusion on diffusion-weighted imaging, are the preferred techniques for determining regions of infarction versus penumbra (Schaefer et al, 2008).
In addition to ischemic changes, according to experimental data, brain inflammation is present during the acute stage of an ischemic stroke, which may be optimally imaged using MRI in combination with USPIOs (del Zoppo et al, 2000; Stoll et al, 1998). There is a growing appreciation for the dual role of inflammation in stroke, with microglia implicated early and macrophages (both bone-marrow derived and brain parenchymal) implicated later in the establishment of a chronic, deleterious, proinflammatory state. Audebert
Work in other experimental stroke models showed that diffusion- and perfusion-weighted MRI using GBCAs is not able to differentiate inflamed from noninflamed infarct subareas (Schroeter et al, 2001). However, using USPIOs and T2*-weighted imaging, hypointense areas indicative of USPIO-laden inflammatory cells can be visualized. These areas of hypointensity were then confirmed by histologic and electron microscopic analyses to correspond with brain sections infiltrated with USPIO-laden macrophages (Rausch et al, 2001; Saleh et al, 2004b).
Several experimental and clinical investigations have been performed to identify the optimal time-window for detecting inflammation after ischemic injury. Experimental data reveal reproducible USPIO-induced enhancement as early as 24h after ischemia. In animal studies, ED1+ cells, a cell marker for macrophages, were found around the core of the infarct within the first 24 h after occlusion of the middle cerebral artery. On days 2 to 4, USPIOs were found mainly between the core and the periphery of the lesions and, by day 7, they were seen only at low concentration both within and around the lesion (Rausch et al, 2001). These findings may be important in the design and monitoring of future neuroprotective trials, especially those involving antiinflammatory agents.
In a single-center, open-labeled, clinical phase II study, the potential for USPIO-enhanced MRI versus conventional GBCA-enhanced MRI to image macrophages in human ischemic stroke lesions was tested. Ten consecutive patients received IV ferumoxtran-10 at the end of the first week after symptom onset. Two follow-up MRI scans were performed 24 to 36h and 48 to 72h after infusion. The USPIO-induced signal alterations in the ischemic area were evident on both T1-weighted and T2/T2*-weighted imaging. Contrast enhancement was observed primarily at the periphery of the infarcted parenchyma. Digital subtraction of GBCA-enhanced regions revealed distinct areas of USPIO enhancement, indicating that these areas of enhancement were not because of BBB disruption, but rather a consequence of iron-labeled macrophage infiltration (Figure 5A) (Saleh et al, 2004a; Saleh et al, 2007). There are very limited data on the utility of USPIOs in stroke. However, Henning
(
Imaging Carotid Atherosclerosis with Ultrasmall Superparamagnetic Iron Oxide Particles
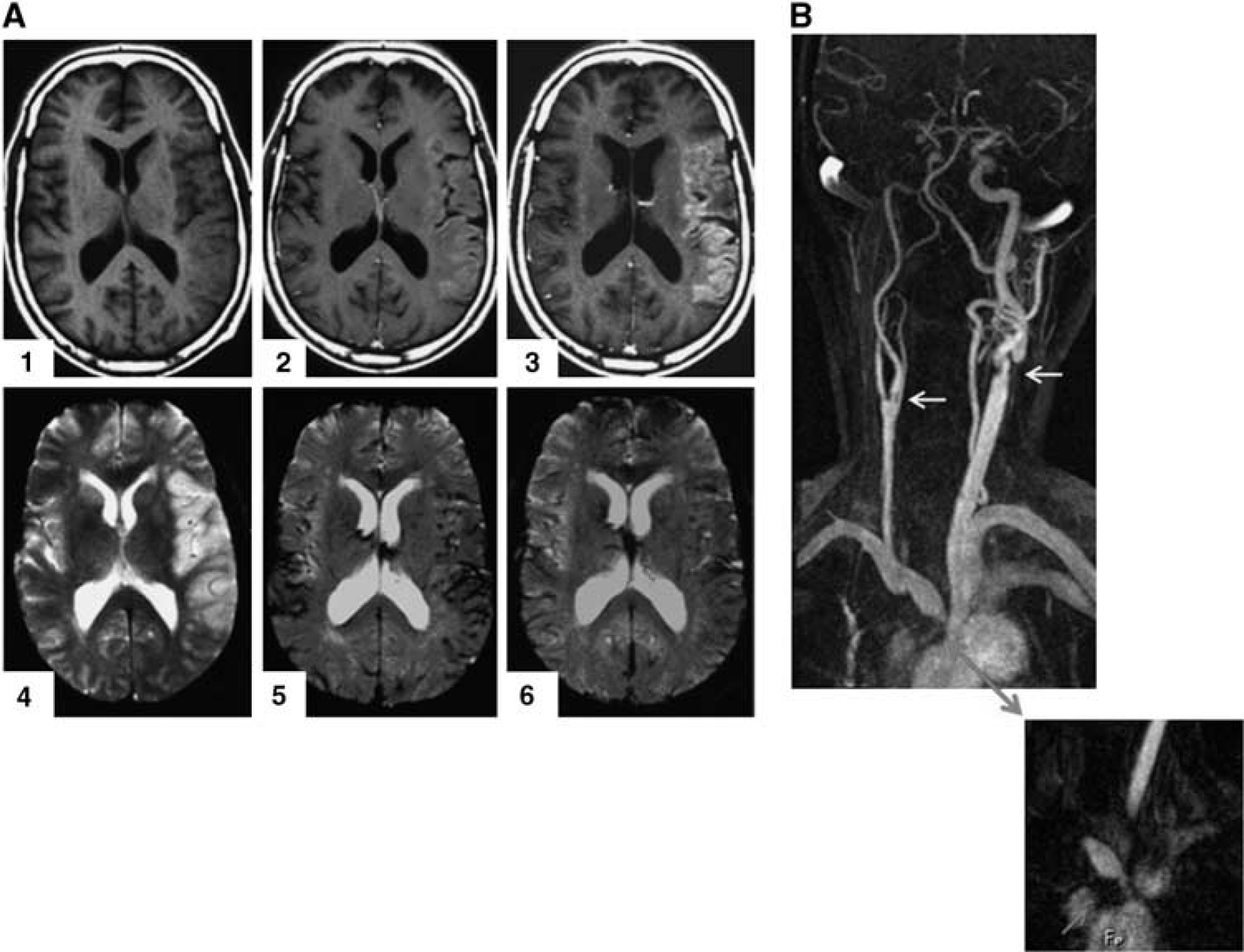
Carotid artery atherosclerosis can be determined by MR angiography using GBCA or USPIO (especially in patients with renal failure), which also helps to verify the severity of stenosis (Figure 5B). However, recently it has been recognized that the composition and stage of atherosclerotic carotid plaques, rather than the severity of stenosis they induce, are important properties for assessing stroke risk. In experimentally induced hyperlipidemic rabbits, USPIOs of a diameter similar to that of low-density lipoprotein, 15 to 25 nm, enter and accumulate in atherosclerotic plaques with high macrophage content (Ruehm et al, 2002; Tang et al, 2006). Cappendijk
Imaging Autoimmune Disorders with Ultrasmall Superparamagnetic Iron Oxide Particles
Multiple Sclerosis and acute disseminated encephalomyelitis (ADEM) are immune-mediated disorders of the CNS. Several observations suggest a major role of macrophages in axonal injury, but the triggers for this autoimmune response have yet to be discovered (Bitsch et al, 2000; Brochet et al, 2006). Experimental autoimmune encephalomyelitis (EAE) is an animal model of human MS. It can be induced in several species by administration of myelin antigens or myelin-reactive CD4+ cells (Rausch et al, 2003). In EAE, USPIO-enhanced MRI reveals areas of hypointensity on T2*-weighted images, which correspond to USPIO-laden mononuclear cells within inflammatory lesions. Immunohistochemical analysis also shows that the iron particles are specifically localized within newly infiltrated ED1+ cells, but not in ED2+ perivascular macrophages (Floris et al, 2004).
In both animal and human studies of MS and ADEM, USPIO-enhancement patterns differ from GBCA enhancement in time (Figure 6) (Bendszus et al, 2005; Dousset et al, 2006; Floris et al, 2004; Rausch et al, 2003; Rausch et al, 2004; Vellinga et al, 2008). Rausch
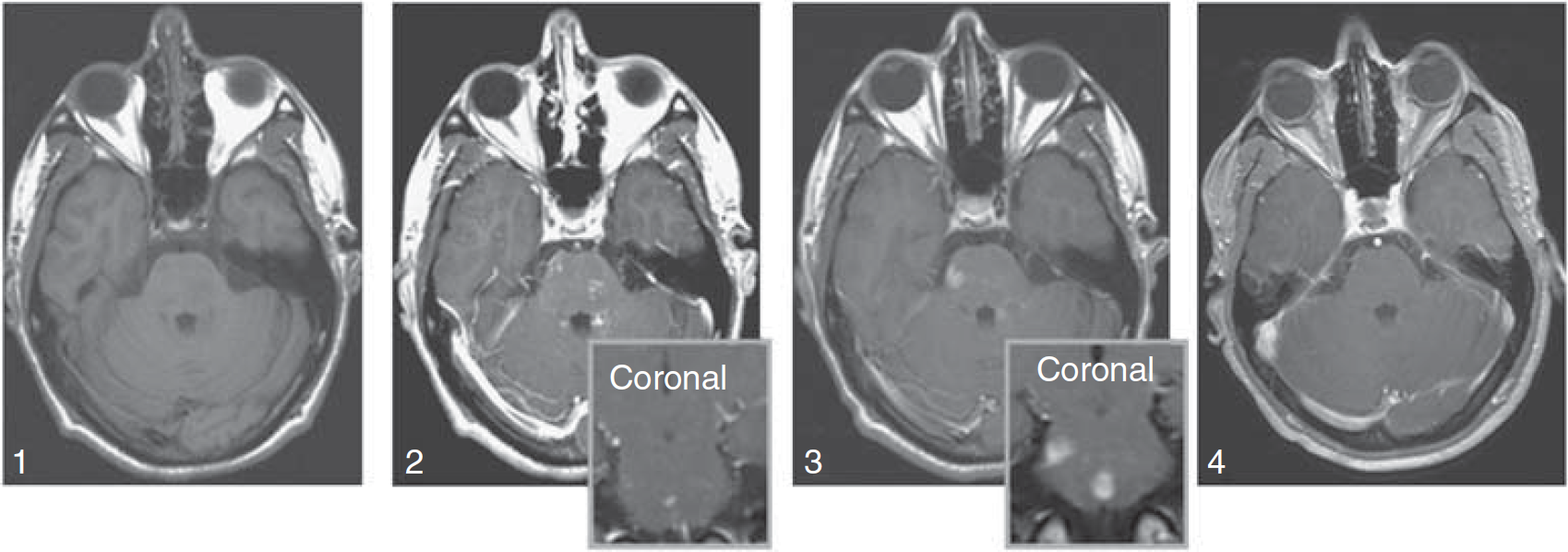
Patient with ADEM. Axial, T1-weighted images without (1), and with (2) gadolinium (inset, coronal) show faint, subtle enhancement in multiple brain stem lesions. Six days later, significant and more prominent enhancement can be seen at the same sites (3) using ferumoxtran-10 (inset, coronal). Three months later, the lesions no longer enhance on T1-weighted images with gadolinium (4).
Baeten
Miki
Acute axonal injury and irreversible axonal loss are generally accepted to be major factors in the pathophysiology of MS. Brochet
Improvements in early disease detection are clearly needed in this field; an exciting alternative to USPIO-enhanced MRI is work being conducted by Sibson
Imaging Central Nervous System Trauma with Ultrasmall Superparamagnetic Iron Oxide Particles
The development of neuroregenerative therapies for patients with traumatic brain or spinal cord injuries is no longer science fiction. Embryonic stem cells and other progenitor cell populations, combined with biocompatible structural matrices, are being investigated for their potential to restore function after trauma (Sykova and Jendelova, 2007). Critical factors for the successful application of these regenerative cell therapies include, ‘the ability of transplanted cells to migrate from the site of transplantation to the lesioned area; to survive, differentiate, and/or produce growth factors and cytokines for the prolonged periods of time necessary for the patient to benefit from their regenerative properties’ (Sykova and Jendelova, 2007). Implantation of stem cells may improve functional recovery after experimental models of brain and spinal cord injury (Bareyre, 2008; Kulbatski et al, 2005; McDonald et al, 1999; Sykova and Jendelova, 2007). The USPIOs may serve as useful adjuncts for noninvasive anatomic and temporal tracking of stem cells in CNS trauma and stroke (Hoehn et al, 2007; Weber et al, 2006).
Although there are limitations to USPIO-based molecular imaging, preclinical studies may benefit from the combination of magnetic cell labeling and tracking
In a controlled cortical injury model of TBI in rat, pooled leukocytes labeled with ferumoxides can be detected histologically around the periphery of the lesion. In the setting of experimental TBI, MRI tracking of USPIO-labeled inflammatory cells is difficult acutely using T2*-weighted imaging sequences because of the presence of free red blood cells. However, pre- and postferumoxytol-enhanced images may be useful for quantifying inflammation (Figure 7) (unpublished data). Dynamic imaging using ferumoxytol for the evaluation of cerebral perfusion and BBB permeability in the acute and chronic stages after TBI, may improve our understanding of the effects of TBI on cerebral hemodynamics. Information about edema formation, and monitoring therapeutic responses to treatments designed to reduce edema and inflammation, will be important in the translation of these novel strategies to humans.
(
Imaging Epilepsy with Ultrasmall Superparamagnetic Iron Oxide Particles
Akhtari
Emerging Therapeutic Applications Using Ultrasmall Superparamagnetic Iron Oxide Particles
The therapeutic applications of USPIOs are also rapidly expanding as the chemistry and throughput for production is streamlined. These agents can be conjugated to drugs, proteins, enzymes, antibodies, or nucleotides and can be directed to an organ, tissue, or tumor using an external magnetic field (Laurent et al, 2008). These same surface modifications, used for diagnostic specificity, will enhance targeting for drug-delivery, gene therapy, radiosensitization, radiation therapy planning with MRI, tissue repair, detoxification, and magnetic fluid hyperthermia (Chertok et al, 2008; Hartman et al, 2008; Khoo and Joon, 2006; Maier-Hauff et al, 2007; Thorek et al, 2006; van Landeghem et al, 2009).
The USPIOs can be used for hyperthermic ablation of CNS tumors after direct inoculation into tumors, or IV administration, depending on the agent's biodistribution. Once targeted, particles are exposed to an alternating magnetic field, which produces electrical current and subsequent energy dispersion in the form of heat. Superparamagnetic species with single magnetic domains, dissipate heat as a result of relaxation of the domain dipole, a process known as Neel relaxation (Hartman et al, 2008). It takes far lower-strength magnetic fields, using VSPIOs (3 to 7 nm), to achieve the same level of heating as larger ferromagnetic agents. One limitation of this treatment strategy has been target specificity. However, a feasibility trial was recently conducted using aminosilane-coated iron oxide nanoparticles in patients with recurrent glioblastoma (Maier-Hauff et al, 2007). In this study, Maier-Hauff
Risk and Utility of Ultrasmall Superparamagnetic Iron Oxide Particles in Comparison to Gadolinium-based Contrast Agents
Although there is solid evidence of the deleterious effects of nanoparticles and in some cases iron oxide nanoparticles, SPIOs appear quite safe and USPIOs, in particular ferumoxytol, appear to be remarkably safe, as evidenced by the recent FDA approval. The FDA-approved package insert for ferumoxytol (Feraheme) reviews three randomized clinical trials with a total of 1726 patients of whom 1562 had chronic kidney disease and were thereby chronically ill patients. Despite this, only two patients had significant reactions to ferumoxytol and these reactions were transient. It appears that in patients who do not suffer from iron overload, ferumoxytol even in seriously ill patients is quite safe.
With regard to its use in comparison to GBCAs, as we have tried to show in this review, except in patients with compromised kidney function, USPIOs are a supplement, rather than a replacement for GBCAs as contrast agents. In a head-to-head comparison, GBCAs are clearly a better screening agent, in part because of the rapid leak into CNS pathologic lesions. With ferumoxytol, it takes 24 h after contrast administration to get analogous images. In addition, in dynamic imaging it appears that Gd is superior to assess permeability (dynamic contrast enhancement), whereas when assessing blood volume and flow, USPIOs such as ferumoxytol act as a blood-pool agent at early time points, and thereby may give more accurate measurements of blood volume and blood flow. As USPIOs specifically target phagocytic cells, that is macrophages, they may also be better for assessing inflammation.
Conclusions
Superparamagnetic iron oxide nanoparticles are an important development for investigation and potential therapeutics across a wide variety of systemic and CNS pathologies. Although there is no perfect MRI contrast agent yet, USPIOs satisfy many of the requirements that limit paramagnetic gadolinium-chelate contrast agents. The USPIOs appear to be safe, are easy to administer, and provide significant contrast enhancement, even on low tesla magnets. They may serve as complimentary agents to improve localization, characterization, and follow-up in diverse neurologic lesions. In CNS tumors, USPIOs may improve detection and diagnosis and, using dynamic studies, will be invaluable in the future for monitoring therapeutic responses to antiangiogenic chemotherapies and for differentiating true tumor progression from pseudoprogression. The USPIOs may also serve as safe alternative contrast agents in patients with renal dysfunction who are at risk for nephrogenic systemic fibrosis with GBCA-based contrast agents. Although USPIOs such as ferumoxytol are not the answer to all diagnostic and therapeutic applications currently envisioned, many of these ideas are years, if not decades, from clinical practice. Ferumoxytol, in particular, is an exciting and powerful tool that is FDA approved and can be used to study a variety of CNS pathologies.
Footnotes
Acknowledgements
We thank Ms. Audrey Selzer for her assistance with 12T MRI acquisitions, Mr. William Woodward for collecting data for ![]() , and Ms. Emily Hochhalter for her administrative assistance. This research was funded in part by the National Institutes of Health grants NS33618, NS34608, NS053468, and NS44687 from the National Institute of Neurological Disorders and Stroke, a Department of Defense Center of Excellence Award, AMAG Pharmaceuticals Inc, and by the Department of Veterans Affairs, all to EAN. This research was also funded in part by a Neurosurgery Research and Education Foundation grant sponsored by Codman, a Johnson & Johnson Company to JSW, NIH RO1-EB007258 to WDR, The Oregon Opportunity and a grant from the WM Keck Foundation.
, and Ms. Emily Hochhalter for her administrative assistance. This research was funded in part by the National Institutes of Health grants NS33618, NS34608, NS053468, and NS44687 from the National Institute of Neurological Disorders and Stroke, a Department of Defense Center of Excellence Award, AMAG Pharmaceuticals Inc, and by the Department of Veterans Affairs, all to EAN. This research was also funded in part by a Neurosurgery Research and Education Foundation grant sponsored by Codman, a Johnson & Johnson Company to JSW, NIH RO1-EB007258 to WDR, The Oregon Opportunity and a grant from the WM Keck Foundation.
The authors declare no conflict of interest.