
Abstract
Numerous epidemiologic observations reporting high prevalence of migraine among young individuals with stroke as well as dysfunction of cerebral arteries during migraine attacks prompt speculation on the existence of a comorbidity between the two disorders. The recent finding of silent infarct-like brain lesions in migraineurs reinforced this hypothesis and raised questions on whether migraine may be a progressive disorder rather than simply an episodic disorder. Stroke can occur during the course of migraine attacks with aura, supporting the assumption of a causal relation between the two diseases. Migraine may accentuate other existing risk factors for stroke, and both jointly increase the risk of cerebral ischemia outside of migraine attacks. In this regard, the role of migraine might be that of predisposing condition for cerebral ischemia. Migraine and ischemic stroke may be the end phenotype of common pathogenic mechanisms. Evidence of a migraine-stroke relation in cases of specific disorders, such as CADASIL (cerebral autosomal—dominant arteriopathy with subcortical infarcts and leukoencephalopathy) and MELAS (mitochondrial myopathy, encephalopathy, lactic acidosis, and stroke-like episodes), strongly supports this concept. Finally, acute focal cerebral ischemia can trigger migraine attacks, and, thus, migraine may be the consequence of stroke. In this paper, we will review contemporary epidemiologic studies, discuss potential mechanisms of migraine-induced stroke and comorbid ischemic stroke, and pose new research questions.
Introduction
Migraine is a common, chronic, multifactorial neurovascular disease characterized by severe attacks of headache and autonomic nervous system dysfunction (migraine without aura; MO). Neurologic aura symptoms (migraine with aura; MA) are present in a percentage of patients, which varies, according to the ascertainment criteria and the study design, from up to one-third in population-based studies to lower frequency in clinic-based studies (Lipton et al, 2001; Launer et al, 1999; Headache Classification Commitee of International Headache Society, 2004).
Although migraine attacks may be acutely disabling, the traditional view is that they do not result in long-term consequences to the brain. Against this assumption, new data have emerged that emphasize the high prevalence of migraine among young individuals with stroke as well as a dysfunction of cerebral arteries during migraine attacks and the finding of silent infarct-like brain lesions in migraineurs, thus leading to the hypothesis that a comorbidity between migraine and cerebral ischemia exists (Lipton and Silberstein, 1994). A careful evaluation of the existing data on the relation between migraine and stroke raises more questions than providing a clear picture.
In this paper, we will review contemporary epidemiologic studies, discuss potential mechanisms of migraine-induced stroke and comorbid ischemic stroke, and pose new research questions.
Migraine as a Risk Factor for Ischemic Stroke
The first epidemiologic suggestion that migraine may be an independent risk factor for stroke came from the Collaborative Group for the Study of Stroke in Young Women (1975), which showed a doubling of the relative risk (RR) of stroke with migraine compared with neighbor controls. Since then, the association of migraine with the risk of stroke has been investigated in several observational studies (Table 1), most of which have been summarized in a recent meta-analysis (Etminan et al, 2005). According to this meta-analysis, the pooled RR of ischemic stroke among patients with any type of migraine is 2.16 (95% confidence interval (CI), 1.89 to 2.48). The RRs for people with MA and MO are 2.27 (95% CI, 1.61 to 3.19) and 1.83 (95% CI, 1.06 to 3.15), respectively. However, as opposed to the MA—ischemic stroke association that was consistently confirmed by subsequent observational studies, two prospective studies and one case—control study recently published and not included in the meta-analysis did not show any increased risk of cerebral ischemia in patients with MO (Kurth et al, 2005; Stang et al, 2005; MacClellan et al, 2007). A stronger predisposing effect of MA was also observed in a recent analysis of the UK-based General Practice Research Database (Becker et al, 2007). Therefore, it seems, at least, unlikely that MA and MO are equally associated with ischemic stroke. At present, as the association is not as robust, whether MO should be considered a stroke risk factor remains unclear.
Risk of ischemic stroke according to type of migraine in epidemiological studies
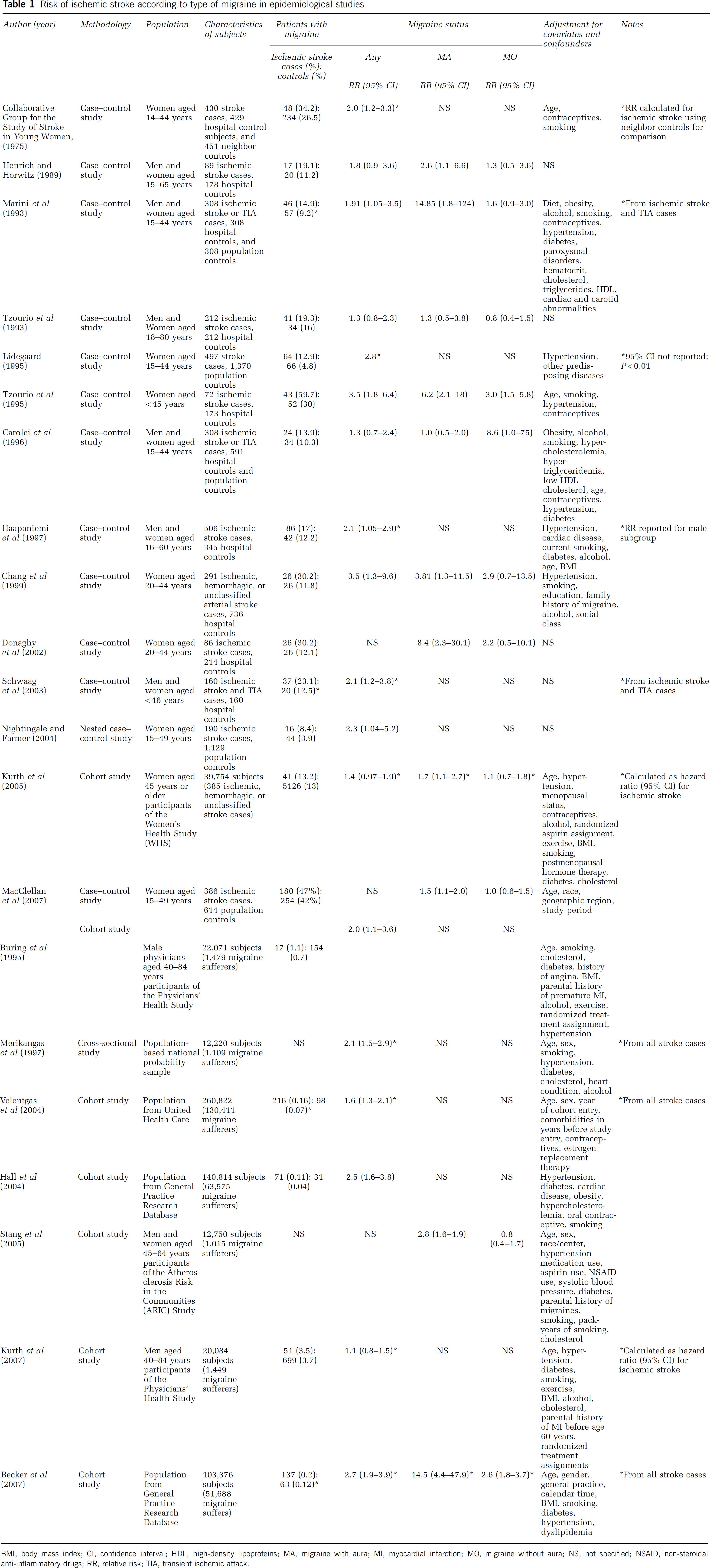
BMI, body mass index; CI, confidence interval; HDL, high-density lipoproteins; MA, migraine with aura; MI, myocardial infarction; MO, migraine without aura; NS, not specified; NSAID, non-steroidal anti-inflammatory drugs; RR, relative risk; TIA, transient ischemic attack.
No difference in the pooled risk was found stratifying analysis by age. Otherwise, all the analyzed studies found an increased risk in young women (RR 2.76; 95% CI, 2.17 to 3.52 for women younger than 45 years). Moreover, users of oral contraceptives had an approximately eightfold increase in the risk of stroke compared with those not using these agents (RR 8.72; 95% CI, 5.05 to 15.05). In line with this observation, recent data from the Stroke Prevention in Young Women Study (SPYW) showed a higher risk of stroke in women with probable migraine with visual aura who were cigarette smokers and oral contraceptive users and further reinforced the hypothesis that specific subgroups of patients in which the migraine—stroke pathogenic link is more expressed might be identified (MacClellan et al, 2007).
Is this enough to conclude that migraine is a risk factor for stroke? As pointed out by many authors, most of these studies are subject to several limitations. First, in most of the considered studies, a consistent definition for migraine is lacking. Accurate diagnosis of migraine is important to avoid nondifferential misclassification of exposure, which will bias the risk estimate toward showing no association. If this is the case, however, we cannot but assume that the increased risk of stroke emerging from the pooled analysis of data from observational studies is rather an underestimation of the effect. As such, it should be retained as an argument in favor of the reported association between migraine and stroke. Furthermore, in case—control studies, an interviewer bias and a recall bias can arise as possible consequences of the retrospective design. Second, potential bias in the selection of patients should be taken into account. At least theoretically, a referral bias may exist if stroke patients with migraine would be referred to the recruiting centers more frequently than stroke cases without migraine, or if the investigators were more prone to include stroke cases with migraine than without migraine. A further selection bias could be the consequence of a stroke—migraine misdiagnosis. Because transient ischemic attacks are sometimes difficult to distinguish from an attack of MA, especially when the aura occurs without headache, and migraine with prolonged neurologic aura (lasting longer than 24 h) may mimic stroke, the end results of such misclassifications would be an overestimation of the prevalence of migraine in cases and, therefore, an overestimation of the risk. Third, in some of the studies the influence of several confounders on the final results was not considered, whereas others were not controlled for. These include, for example, the use of medications with a potential effect on stroke risk (i.e., antihypertensive agents), or risk factors for both migraine and stroke, such as antiphospholipids antibodies. Finally, most studies are limited to younger individuals (aged 45 years or younger) leaving the association between migraine and stroke among the elderly unclear and ignoring the fact that migraine may start later in life.
With regard to this last observation, two prospective studies recently examined this relation. Data from 39,876 US female health professionals aged 45 years or older included in the Women's Health Study after a mean of 9 years of follow-up showed that MA increased 1.5-fold the risk of total stroke after adjusting for potential confounders of age, hypertension, menopausal status, contraceptive use, and alcohol consumption (hazard ration (HR) 1.53; 95% CI, 1.02 to 2.31) and 1.7-fold the risk of ischemic stroke (HR 1.71; 95% CI, 1.11 to 2.66) when compared with participants without migraine (Kurth et al, 2005). In contrast, there was no association between MO and total stroke or ischemic stroke. This association between MA and cerebrovascular disease as well as with ischemic stroke was confirmed in a large cohort of individuals ≥55 years of age at the time of migraine assessment, who participated in the Atherosclerosis Risk in Communities (ARIC) Study (Stang et al, 2005).
Taken together, these findings provide arguments to the assumption that migraine may have some influence on stroke risk even in older subgroups. However, effect modification by age is evident from prospective data, the risk of stroke being higher in younger age groups and decreasing over time, with no increased risk among the elderly (age 60 years or older) according to case—control analyses (Mosek et al, 2001). Whether this is the consequence of the greater effect of other major risk factors for ischemic stroke with increasing age or of their interaction with the mechanism by which migraine may lead to stroke remains to be determined.
The association between migraine and increased prevalence of cardiovascular risk factors and the observation that the vascular dysfunction of migraine may also extend to coronary arteries (Uyarel et al, 2005) has recently led to speculation that migraine, especially MA, may not only be associated with increased risk of stroke but also with other vascular events. To address this specific issue, data from two large-scale prospective cohorts of apparently healthy subjects, one including women aged 45 years or older participating in the Women's Health Study (WHS) and the other including men aged 40 to 84 years participating in the Physicians' Health Study (PHS), were recently analyzed (Kurth, 2007). Data from the 27,840 women included in the WHS indicated an association between overall migraine and major ischemic cardiovascular disease after a mean of 10 years of follow-up. Such an increased risk for any ischemic vascular events was only apparent for women with MA, and turned out to be approximately twofold higher compared with that observed in women who did not report any history of migraine after adjustment for traditional cardiovascular risk factors. In contrast, no increased risk for any ischemic vascular events was observed in women who reported MO (Kurth et al, 2006).
With regard to men, data from the 20,084 male physicians included in the PHS indicated an association between overall migraine and major cardiovascular disease. Compared with nonmigraineurs, men who reported migraine had an increased risk for major cardiovascular disease, ischemic stroke, myocardial infarction, coronary revascularization, angina, and ischemic cardiovascular death. In case of stroke, men who were younger than 55 years of age had increased risk of stroke, which was not apparent in the older age group (Kurth et al, 2007), thus suggesting an age-dependent effect of migraine on disease risk.
At least theoretically, it cannot be excluded that the relation between migraine and stroke might be just one aspect of a more generalized effect of chronic nonspecific headache. Actually, the evaluation of cross-sectional data from the first US National Health and Nutrition Examination Survey (NHANES I) showed a 1.5-fold increased risk of stroke in both patients with migraine and patients with severe nonspecific headache compared with the subjects without these conditions (Merikangas et al, 1997). More recently, in a prospective cohort study derived from the FINRISK study, Jousilahti et al (2003) found a significant association between chronic nonspecific headache and stroke among men. However, because of the diagnostic criteria adopted in the NHANES I study, it is likely that most cases of severe nonspecific headache were actually migraine sufferers. Similarly, the lack of a precise definition of migraine represents a major limitation for a correct interpretation of the data proposed by Jousilahti and co-workers. These drawbacks, in association with recent data from large prospective cohorts, showing no association between nonmigraine headache and stroke, make the hypothesis of a major effect of any nonspecific headache on the risk of cerebral ischemia very unlikely.
Classification of Migraine-Related Stroke
One of the most relevant drawbacks in unrevealing the complex relation between migraine and cerebral ischemia is the lack of consistency in the definition of migraine-related stroke. In the attempt to categorize this entity, four major issues might be considered (Welch, 2003). First, cerebral ischemia can occur in the course of an attack of MA, causing true migraine-induced infarction. Second, migraine and stroke share a common underlying disorder that increases the risk of both diseases. Third, migraine might cause stroke only because other risk factors for stroke are present to interact with the migraine-induced pathogenesis. Fourth, stroke may mimic migraine.
Migraine-Induced Stroke: the Migrainous Infarction
It has long been recognized that, although a rare event, stroke may occur during the course of a migraine attack with aura. This phenomenon suggests a causal relationship between migraine and stroke.
According to the International Headache Society (IHS) migraine classification, ‘migrainous infarction’ is defined as a stroke occurring during a typical attack of MA (Headache Classification Commitee of International Headache Society, 2004). Patients have a history of MA and the neurologic deficits occur in the same vascular distribution as the aura and are associated with an ischemic brain lesion in a suitable territory shown by neuroimaging. A major criterion of this cause of infarction is that other possible causes are excluded by appropriate investigations. However, which investigations should be carried out and when is not clear. The absence of causes other than migraine does not necessarily imply that migraine is the cause, given that about half of the ischemic strokes in young adults have no detectable cause.
Furthermore, stroke has been reported in persons experiencing MO, and in two large series this was more common than infarcts during attacks of MA (General discussion, 1998; Linetsky et al, 2001). Criteria for true migraine-induced stroke should include potentially modifying risk factors that might be present and that are critical to understanding the mechanisms. Finally, the definition of migrainous stroke, with the stipulation that the present MA attack is typical of previous attacks, is also biased toward posterior cerebral artery territory infarcts, because most aura are visual in nature.
According to large series, the incidence of migrainous infarction (Merikangas et al, 1997; Linetsky et al, 2001; Arboix et al, 2003; Kittner et al, 1998; Sochurkova et al, 1999) varies between 0.5% and 1.5% of all ischemic strokes and 10% to 14% of ischemic strokes in young patients. The incidence of migraine-related infarction (per 100,000 persons per year) was estimated at 1.44 (95% CI, 0 to 3.07) from the Oxfordshire Community Stroke Project prospective registry, and at 1.7 from a retrospective review of Mayo Clinic records from nearly 5,000 migraineurs aged < 50 years (Henrich et al, 1986; Broderick and Swanson, 1987). In series published since the introduction of the IHS criteria, the percentage of stroke in persons aged < 45 years attributed to migrainous infarction ranges from 1.2% to 14% (Arboix et al, 2003; Kittner et al, 1998; Sacquegna et al, 1989; Kristensen et al, 1997). The clinical features typifying migrainous stroke included female sex, mean age in the low-to-mid 30s, a history of cigarette smoking, and ischemic involvement of the posterior cerebral artery territory (Arboix et al, 2003).
In summary, IHS criteria might be too strict for a correct diagnosis of migrainous infarction. In spite of the limitations inherent in the diagnostic criteria and the consequent weakness of the epidemiologic studies, it seems reasonable to assume that migrainous infarction does not account for all strokes occurring during migraine attacks, and, overall, it is responsible for only a minority of migraine-related infarcts.
Symptomatic Migraine
Cerebral autosomal-dominant arteriopathy with subcortical infarcts and leukoencephalopathy is an autosomal-dominant disease of vascular and smooth muscle cells due to
Cerebroretinal vasculopathy and HERNS are two rare inherited conditions characterized by a primary microangiopathy of the brain in combination with vascular retinopathy. A distinctive feature of CRV and HERNS is the presence of progressive subcortical contrast-enhancing lesions with surrounding edema (pseudotumors) typically located within the frontoparietal white matter. Migraine is a clinical finding in some cases, also including progressive visual loss, seizures, focal neurologic deficits of sudden onset (stroke-like), cognitive worsening, renal insufficiency, and proteinuria.
Mitochondrial myopathy, encephalopathy, lactic acidosis, and stroke-like episodes is associated with several mutations in mitochondrial DNA. The phenotypic expression is highly variable ranging from asymptomatic state to severe childhood multisystem disease with lactic acidosis. Recurrent episodes of headache (mostly migraine) are part of the clinical spectrum.
Migraine is also a clinical finding of other mitochondrial disorders such as Leber's hereditary optic neuropathy, myoclonic epilepsy with ragged-red fibers, and a syndrome characterized by neuropathy, ataxia, and retinitis pigmentosa (Ferrari and Haan, 2001; Haan et al, 1997).
Migraine is also part of the clinical spectrum of hereditary hemorrhagic teleangiectasia (Osler—Weber—Rendu disease), an autosomal-dominant vascular dysplasia characterized by a high prevalence of vascular malformations in various organs, including the lung, liver, kidney, and brain, as well as by mucocutaneous teleangiectasias (Guttmacher et al, 1995).
Migraine with aura is classically related to cerebral arteriovenous malformations (AVMs). In most of these cases, MA ceasing after the removal of AVM has been documented, consistent with the definition of symptomatic migraine, but there are also sparse reports of cases unchanged after surgery (Has, 1991). The possibility of a causal relation is indirectly supported by the side of aura, being contralateral to the AVMs and the side of headache, being ipsilateral to the AVMs, as well as by the coexistence of MA and arteriovenous shunts in leptomeningeal angiomatosis (Sturge—Weber syndrome) (Chabriat et al, 1996).
Diffuse White Matter Lesions in Migraineurs
Abnormalities of uncertain clinical significance are frequent findings on brain MRI scans of patients with migraine. The most common abnormality is white matter lesions (WMLs), typically multiple, small, punctate hyperintensities occurring in the deep or periventricular white matter and often seen on T2-weighted or Fluid-Attenuated Inversion Recovery (FLAIR) images. Not infrequently, these WMLs may cause uncertainty for physicians and anxiety for patients and can lead to a variety of diagnostic tests and treatments (McDonald et al, 1996). In a small minority of cases, the number, distribution, and location of WMLs may lead to the diagnosis of an underlying disease of which migraine may be but one symptomatic manifestation (Table 2).
Differential diagnosis of multifocal white matter lesions
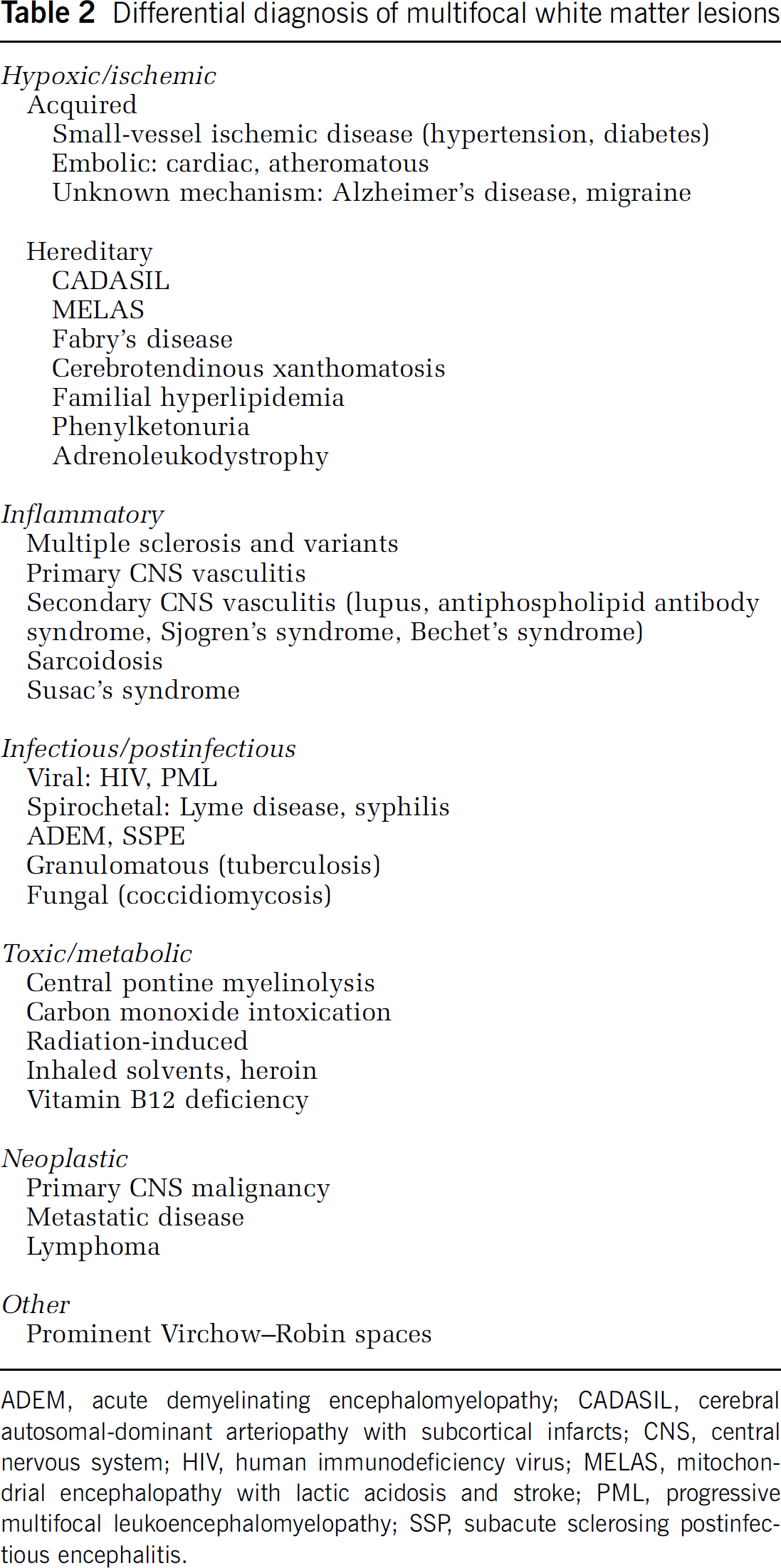
ADEM, acute demyelinating encephalomyelopathy; CADASIL, cerebral autosomal-dominant arteriopathy with subcortical infarcts; CNS, central nervous system; HIV, human immunodeficiency virus; MELAS, mitochondrial encephalopathy with lactic acidosis and stroke; PML, progressive multifocal leukoencephalomyelopathy; SSP, subacute sclerosing postinfectious encephalitis.
The clinical history, the presence or absence of cardiovascular risk factors, family history, physical examination, and specific neuroimaging features assist clinicians in narrowing the differential diagnosis in these cases, whereas, in selected circumstances, specific biochemical and genetic testing, and further neuroimaging are necessary.
White matter lesions are common in the general population, occurring in approximately 10% of individuals in the fourth decade of life and up to 80% of individuals in the eight decade (Fazekas et al, 1989). Several reports suggest that the prevalence and the number of WMLs on brain MRI scan increase with advancing age, vascular risk factors (diabetes, smoking, hypercholesterolemia, hypertension), cardiovascular disease, stroke, and dementia (de Groot et al, 2000; Vermeer et al, 2003). The prevalence of WMLs in migraine ranges from 6% to 40% (Fazekas et al, 1992; Gozke et al, 2004). Suggested variables that might influence this association are the quality of MR imaging equipment and sequences used, patient's age, migraine type and frequency, and the presence or absence of vascular risk factors.
Results of a recent meta-analysis showed a fourfold increased prevalence of WMLs on MRI scan in patients with migraine compared with nonmigraineurs age- and sex-matched controls (odds ratio (OR), 3.9; 95% CI, 2.26 to 6.72). The risk of WMLs in migraineurs appears to be independent on both age and vascular risk factors (Swartz and Kern, 2004). The recently published Cerebral Abnormalities in Migraine, an Epidemiological Risk Analysis (CAMERA) study supports the observation that some migraineurs are at increased risk for subclinical infarct-like brain lesions (Kruit et al, 2004). This cross-sectional prevalence study evaluated a population-based sample of Dutch adults aged 30 to 60 years. Randomly selected patients with MA (
Overall, the study showed that patients with MA have a 12-fold increased risk of cerebellar infarct-like lesions and that female migraineurs had more supratentorial deep WMLs than nonmigraineurs. The risk of lesions increased with attack frequency, independent on cardiovascular risk factors.
Further analyses of the infarct-like lesions observed in the CAMERA study were subsequently performed, in which topographic details of these parenchymal defects were systematically characterized to better define their pathophysiology (Kruit et al, 2005; Kruit et al, 2006). The combination of vascular distribution, deep border zone location, shape, size, and imaging characteristics on MRI makes it likely that these lesions have an infarct origin. If these lesions are true vascular infarcts, it might be that a combination of (possibly migraine-related) hypoperfusion and embolism is the likeliest mechanism, and not atherosclerosis or small-vessel disease. However, because there are no postmortem studies identifying the pathology of these MRI findings, their etiology is unknown. Interestingly, a case patient with migraine who developed what appeared to be cerebellar infarcts on MRI, but whose lesions vanished on repeat imaging, which questions an ischemic pathology, has been reported (Rozen, 2007).
Is Migraine a Progressive Disorder?
The evidence of WMLs in migraineurs opens the issue of whether migraine may be a progressive disorder in some way rather than simply an episodic disorder. The natural history of migraine is to decrease in severity and to abate and disappear in later life, suggesting a nonprogressive course. However, in a population sample, Scher et al (2003) showed that over the course of 1 year, 3% of individuals with episodic headache (headache frequency 2 to 104 days per year) progressed to chronic daily headache (attacks frequency > 180 days per year). This population-based result is compatible with findings from a case—control study and numerous clinic-based observation studies (Scher et al, 2002).
Imaging results suggesting progressive brain changes in migraine are particularly interesting in light of these epidemiologic results. However, these data should be interpreted cautiously because numerous factors, other than the presumed progressive course of the disease, may contribute to ‘chronification’ of episodic migraine. Among them, one of the most common modifiable factors for transformation, occurring in approximately one-third of patients developing chronic daily headache, is analgesic overuse. The evidence that chronic daily headache may spontaneously revert to episodic in some cases is a further argument against the hypothesis of migraine as a progressive disorder (Scher et al, 2002). Finally, because the migraine-stroke relation seems to be subtype specific, the influence being prominent for MA and negligible for MO, one might speculate that migraine is a progressive disorder only in a specific subgroup of subjects. Therefore, whether migraine causes permanent, progressive brain lesions is not definitively established and there is no data whether lesions in the brain produce chronic migraine. Only a longitudinal study would give information on the accumulation of lesion load that would provide evidence for a progressive course.
How can Migraine Lead to Ischemic Stroke?
So far, no fully convincing evidence has been produced to explain the exact mechanism of the increased risk of ischemic stroke in migraine. Numerous hypotheses have been raised including vasospasm, endothelial dysfunction, congenital thrombophilia, platelet hyperaggregability, and association with cardiac abnormalities, among others.
A first hypothesis is that stroke can occur during the course of migraine attacks with aura (migrainous stroke). Migraine is considered to be a neurovascular disorder in which arterial constriction and decreased blood flow to the posterior circulation are consequences of a spreading wave of neuronal depression in the cerebral cortex. In this regard, CSD may induce short-lived increases in cerebral blood flow and tissue hyperoxia (Cao et al, 1999), followed by a more profound oligemia and consequent increased intraparenchymal vascular resistance (Cutrer et al, 1998). Thus, low flow in major intracerebral vessels may be due to increased downstream resistance and not due to major intracranial arterial vasospasm. Essentially, a low cerebral blood flow and neuronally mediated vasodilatation could cause sluggish flow in large intracerebral vessels during the aura of migraine. When combined with factors predisposing to coagulopathy, such as dehydration hyperviscosity, or intravascular thrombosis, migraine-induced cerebral infarction could occur, although rarely. Neurogenically mediated inflammatory responses accompanying vasodilation of extraparenchymal vessels caused by release of vasoactive peptides and nitric oxide, the activation of cytokines, and the upregulation of adhesion molecules also predispose to intravascular thrombosis (Bolay et al, 2002). This could explain why migraine-induced stroke usually respects intracranial arterial territories whereas aura involves more widespread brain regions. In addition, frequent aura, if due to CSD, could induce cytotoxic cell damage and gliosis based on glutamate release or excess intracellular calcium accumulation (Welch and Ramadan, 1995). Thus, a persistent neurologic deficit could be due to selective neuronal necrosis. Finally, vasospasm, the result of the release of vasoconstrictive molecules, including endothelin and serotonin, once thought to be the mechanism of migraine aura, has been implicated in migrainous infarction, although documented cases are rare.
Experimental data also point toward the activation of the thrombotic cascade during the course of a migraine attack. In fact, platelets and mast cells have been shown to release platelet-activating factor, a potent inducer of platelet activation and aggregation, also involved in the release of von Willebrand factor, and indirectly in the activation of the platelet IIb/IIIa receptor, crucial for binding fibrinogen, thus leading to primary hemostasis (McCrary et al, 1995). Increased plasma levels of these molecules have been observed during the course of migraine attacks compared with those in the interictal phases.
However, these mechanisms hold only for the so-called migrainous strokes, which, as defined by the IHS criteria, is a rare event. Therefore, its low incidence cannot explain the increased risk of stroke in migraine. Further, ischemic strokes mostly occur between migraine attacks (Tzourio et al, 1993, 1995).
A second hypothesis is that the migraine—ischemic stroke pathway is modulated by the intervention of common risk factors. In this regard, different case—control studies have observed that patent foramen ovale (PFO) is significantly more common in patients who suffered MA than in patients without migraine (Anzola et al, 1999; Del Sette et al, 1998). Similarly, in patients with ischemic stroke, MA is twice as prevalent in patients with PFO than in those without (Lamy et al, 2002; Sztajzel et al, 2002). Several observational studies, from both single and multicenter experiences, suggest PFO closure to reduce the frequency of migraine attacks. In particular, among migraineurs this might be proposed for those patients in the MA subgroup and might indirectly reduce the risk of stroke, in spite of the small stroke predisposing effect of PFO and some recent findings indicating no stronger association between MA and ischemic stroke among women with PFO compared with women without (MacClellan et al, 2007). However, these reports present some limitations, including retrospective design that implicates recall bias, the absence of control group, placebo effect that can result in a up to 70% reduction of attack frequencies (Migraine-Nimodipine European Study Group, 1989a,
b
), administration of aspirin after PFO closure and its potential prophylactic effect (Diener et al, 2001). Paradoxical embolism is suggested to be the causal link between migraine and PFO, but insufficient data are available to substantiate the hypothesis that migraine frequency (and, indirectly, ischemic stroke risk) is reduced by PFO closure. The only way to address this issue is by randomization. At present, only one prospective, randomized, double-blind trial on the therapeutic effect of PFO device closure on MA patients compared with sham has been conducted (Migraine Intervention with STARFlex® Technology, MIST). In the MIST trial, 73 patients underwent a sham operation and 74 patients had their PFO closed. The primary end point of the study, complete elimination of headache, was not achieved, as three patients in the treatment group versus three patients in the sham group had complete resolution of migraine. In contrast, one of the preplanned secondary end points of the MIST trial showed that patients who underwent PFO closure had a 37% reduction in median total migraine headache days compared with 26% in the sham group (
Although unproven, these observations prompt to speculation that migraine might be a predisposing condition for specific pathogenic subtypes of ischemic stroke, particularly in young patients. In the last years, some observations have suggested migraine as a predisposing condition for sCAD, one of the most common causes of stroke in young patients. In two French case—control studies, migraine resulted twice as common in patients with sCAD compared with patients whose ischemic stroke was not related to a CAD (D'Anglejan-Chatillon et al, 1989; Tzourio et al, 2002), and this association was stronger and more significant in patients with dissections involving multiple vessels. A large Italian case—control study confirmed these findings (Pezzini et al, 2005). The mechanism by which migraine may affect the risk of sCAD is unknown. A common generalized vascular disorder is hypothesized to be a predisposing condition for both diseases. Recent observations of increased activity of serum elastase, a metallopeptidase that degrades specific elastin-type amino acid sequences, in migraineurs suggest a possible extracellular matrix degradation (Tzourio et al, 2000) that might facilitate sCAD occurrence. Furthermore, in line with previous observations of altered common carotid artery distensibility in patients with sCAD (Guillon et al, 2000), Lucas et al (2004) recently reported that the endothelium-dependent vasodilatation assessed in the brachial artery is significantly impaired in these subjects. Similar vascular changes have been observed in migraine patients during interictal periods (de Hoon et al, 2003) and replicated in a recent cross-sectional study in migraineurs of recent onset, thus excluding possibility of bias due to longstanding history of migraine and repeated exposure to vasoconstrictor drugs (Vanmolkot et al, 2007). Finally, the analysis of small families has shown that the structural abnormalities related to sCAD might be familial and follow an autosomal-dominant pattern of inheritance (Grond-Ginsbach et al, 2002; Hausser et al, 2004). This implicates that genetically determined alterations of the extracellular matrix may play a crucial pathogenic role and that candidate genes involved in the regulation of endothelial and vessel wall functions might increase susceptibility to both conditions (Kloss et al, 2006; Pezzini et al, 2002; Scher et al, 2006).
A third hypothesis is that a number of predisposing conditions may be operant in increasing the risk of ischemic stroke in migraine, particularly in young women. Hormonal status seems to play a pathogenic role in the development of MO, but not of MA, which, as a matter of fact, represents the situation where the incidence of ischemic stroke is higher (Bousser, 2004). Inconsistent results have also been found for the various biologic or clinical markers of thrombotic risk studied so far (Crassard et al, 2001; Kern, 2004), such as platelet activation, factor V Leiden mutation (Soriani et al, 1998), von Willebrand factor (Tietjen et al, 2001), prothrombin factor 1.2 (Hering-Hanit et al, 2001), platelet leukocyte aggregation (Zeller et al, 2004), antiphospholipid antibodies (Cervera et al, 2002; Tietjen et al, 1998), and livedo reticularis (Tietjen et al, 2002).
In contrast, there is mounting evidence that migraine may be a risk factor for endothelial dysfunction, which may represent a link to ischemic stroke and heart disease. Endothelial dysfunction is characterized by the reduction in bioavailability of vasodilator (such as nitric oxide), an increase in endothelial-derived contracting factors, and consequent impairment of the microvasculature reactivity. It also comprises endothelial activation, characterized by a procoagulant, proinflammatory, and proliferative state, which in turn predisposes to ischemia. Endothelial dysfunction is mediated by increased oxidative stress, an important promotor of the inflammatory process (Bonetti et al, 2003), which has been proposed in the pathogenesis of migraine. In fact, compared with migraine-free controls, oxidative stress markers have been found to be higher in migraineurs, even during the interictal period, thus yielding support to the association.
A fourth hypothesis is that the migraine—stroke link is caused by the effects of specific medications. Actually, drugs used in migraine, such as triptans and ergot alkaloids, have been investigated as a possible risk factor for ischemic events. Cardiovascular safety of migraine treatments has been brought forward by their vasoconstrictive action and by reported cases of stroke, myocardical infarction, and ischemic heart disease after triptan and ergotamine use (Tfelt-Hansen et al, 2000; Mueller et al, 1996). Moreover, an increased number of white matter abnormalities (Kruit et al, 2004) and mortality (Velentgas et al, 2004) has been found in patients taking ergotamine. In the last years, large-scaled studies have investigated the risk of ischemic events and death in patients with triptan and ergotamine-treated migraine. Data from General Practice Research Database in the United Kingdom showed that in general practice, triptan treatment did not increase the risk of ischemic events (Hall et al, 2004). Similarly, this finding was confirmed by a wide retrospective cohort study from a health-care provider in the United States (Velentgas et al, 2004). This study also investigated the rates of vascular events in relation to ergotamine use finding no association. Recently, a retrospective nested case—control study using data from the PHARMO Record Linkage System conducted in The Netherlands investigated whether the overuse of triptans and ergotamina is associated with an increased risk of ischemic events (Wammes-van der Heijden et al, 2006). Results showed that overuse of triptan, neither in the general population nor in those using cardiovascular drugs, increases the risk of cerebral, cardiovascular, or peripheral ischemic events. In contrast, ergotamine overuse increases significantly the risk of ischemic complications (OR 2.55; 95% CI, 1.22 to 5.36), especially in patients concomitantly using cardiovascular drugs (OR 8.52; 95% CI, 2.57 to 28.2). However, therapeutic doses of either triptans or ergotamines were not associated with an increased risk of ischemic vascular events. Overall, these findings suggest that triptan use and even triptan overuse are safe in general, although heighten the risk of ischemic complications due to ergotamine overuse, likely in relation to its greater vasoconstrictive properties.
Finally, migraine and cerebral ischemia might be linked via genetic pathways.
Genetic Influence on Migraine—Stroke Relation
Over the past years, evidence from twin and family history studies, although not entirely consistent, has supported the notion that genetic predisposition plays a major role in the occurrence of both migraine and ischemic stroke (Ferrari, 2003).
Monogenic Forms of Migraine
Although many chromosomal regions have been reported to be possibly involved in migraine occurrence, the mutations in three genes for familial hemiplegic migraine (FHM) represent the only established monogenic cause of migraine so far. Familial hemiplegic migraine is a subtype of MA characterized by an autosomal-dominant pattern of inheritance and at least some degree of weakness (hemiparesis) during the aura. In spite of these clinical markers, a broad variability is the rule: age at onset, frequency, duration, and features of attacks may be different from one patient to another, even among affected members from a given family who carry the same mutation in the same gene (Ducros et al, 2001; Terwindt et al, 1998), and less frequent features such as cerebellar ataxia, which occurs in some families, minor head trauma acting as triggering factor, and severe attacks with impairment of consciousness have also been reported. Furthermore, the majority of FHM patients also experience attacks of typical MA and MO. Thus, it seems reasonable to assume that FHM represents one side of the spectrum that at the other end is formed by the common forms of migraine and, as a consequence, a valid model to study genetic factors of migraine in general as well as the relation between migraine and ischemic stroke.
To date, three different genes responsible for different subtypes of FHM have been identified. FHM1 is caused by mutations in the
Overall, the common consequence of FHM1, FHM2, and FHM3 mutations seems to lead to increased levels of glutamate and potassium in the synaptic cleft causing an increased propensity to CSD. Whether this might also increase the propensity to cerebral ischemia is unknown.
Similarly, the contribution of FHM genes in common forms of migraine (MO and MA) remains unclear (Colson et al, 2007). A recent study showed no linkage to the
Polygenic Forms of Migraine
The recent diffusion of powerful new technologies of gene analysis along with the possibility to use informatics resources that provide genome-wide sequence and variant data has fostered an effective and challenging approach to complex diseases. Among these, genetic association studies are retained as a powerful instrument to identify small RRs. On the basis of the results of such analyses, several specific genetic variants have been implicated in migraine susceptibility, which can be gathered from three main streams (Colson et al, 2007). The first group includes genes involved in neurotransmitter-related pathway, such as genes encoding for dopamine D2 receptor (
Several candidate genes for migraine are also good candidate for cerebral ischemia (Table 3). Among them, in spite of the inconsistent results of some studies exploring the hypothesis of a link between this marker and migraine (Rubino et al, 2007), the C677T polymorphism of the
Association studies of candidate genes for migraine also analyzed as candidate genes for ischemic stroke
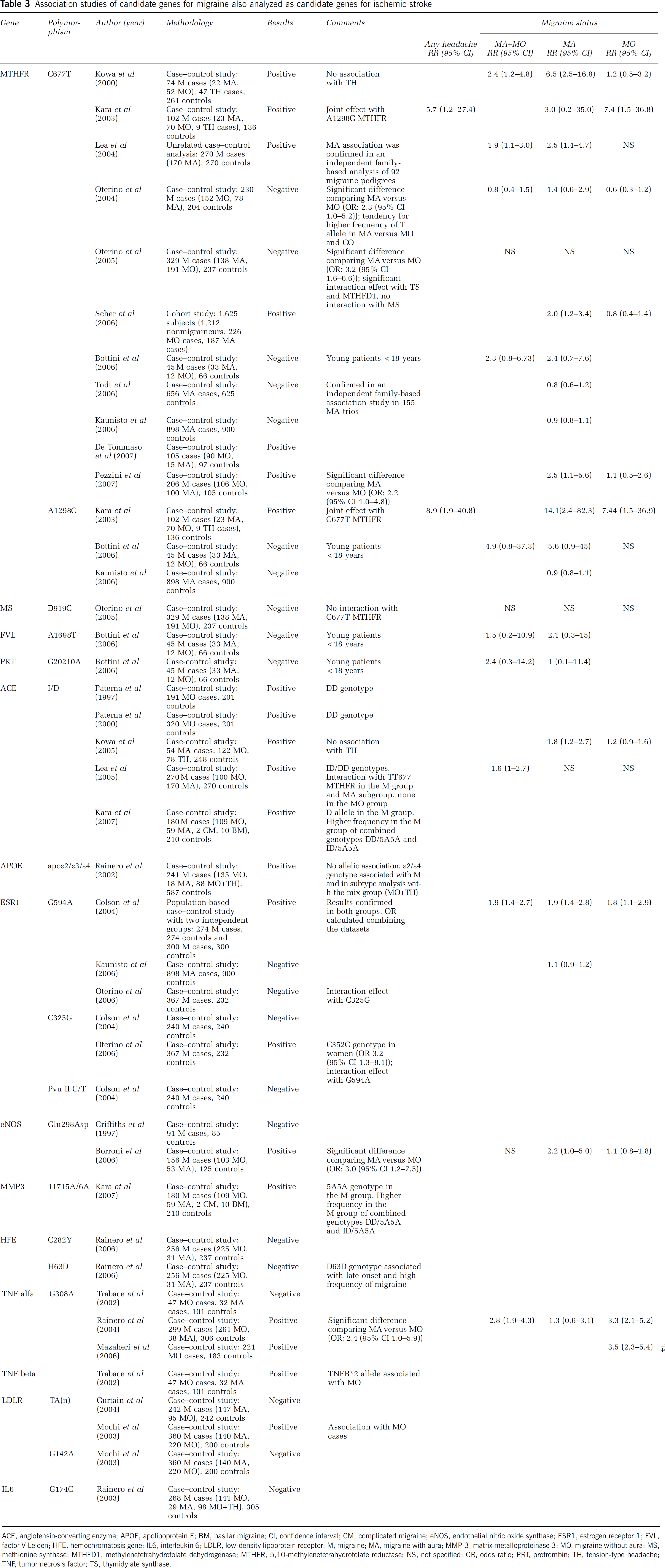
ACE, angiotensin-converting enzyme; APOE, apolipoprotein E; BM, basilar migraine; CI, confidence interval; CM, complicated migraine; eNOS, endothelial nitric oxide synthase; ESR1, estrogen receptor 1; FVL, factor V Leiden; HFE, hemochromatosis gene; IL6, interleukin 6; LDLR, low-density lipoprotein receptor; M, migraine; MA, migraine with aura; MMP-3, matrix metalloproteinase 3; MO, migraine without aura; MS, methionine synthase; MTHFD1, methylenetetrahydrofolate dehydrogenase; MTHFR, 5,10-methylenetetrahydrofolate reductase; NS, not specified; OR, odds ratio; PRT, protrombin; TH, tension-type headache; TNF, tumor necrosis factor; TS, thymidylate synthase.
In this regard, we recently reported the results of a genotype—migraine—stroke interaction study in which the TT-genotype of the C677T
Although genes involved in the migraine—stroke relation remain to be fully elucidated, we believe this methodological approach may shed light into the pathophysiological pathways linking the two disorders, and eventually result in new and individualized therapeutic strategies.
Practical Implications
The identification of susceptibility factors linking migraine to ischemic stroke is still in its early stages, and, thus, in the short term, it will be impossible to stratify migraine sufferers and identify those at highest risk of stroke occurrence. At present, available data support the following recommendations:
emphasis on identification and treatment of modifiable vascular risk factors, such as smoking, hypertension, diabetes, and hypercholesterolemia, is warranted in migraineurs, especially those with MA. Because of the potential synergistic effect of several migraine-specific drugs with vasoconstrictive action, including triptans, and traditional predisposing conditions in increasing the risk of ischemic stroke, subjects with major cardiovascular risk factors should be encouraged to adopt migraine prophylactic strategies. This approach should be also recommended to those subjects with a personal history of prior ischemic (cerebral and/or myocardial) disease. Drugs that can decrease the risk of stroke (i.e., antihypertensives) are valid pharmacological options in these cases, whereas non-steroidal anti-inflammatory drugs (NSAIDs) or combination analgesics should be considered as an alternative acute treatment approach. Triptans are also contraindicated in patients with hemiplegic and basilar migraine. Estrogen-containing oral contraceptives should not be prescribed to women with MA, particularly when they have major vascular risk factors or are aged > 35 years. There is no direct evidence that PFO closure is effective for MA prophylaxis and, indirectly, for primary prevention of stroke, and, as a consequence, this procedure cannot be recommended for MA prophylaxis. Positive results from small observational studies need to be confirmed in the setting of a randomized, unbiased, placebo-controlled study with adequate power. Whether antiplatelet agents might be an effective preventive measure in these subjects remains to be determined. Patients with migrainous stroke should undergo the same diagnostic workup and receive the same pharmacological treatment of any ischemic stroke in the young, both in the acute phase and at follow-up. The possibility that migraine may be conceptualized not just as an episodic disorder but as a chronic episodic disorder and sometimes chronic progressive disorder remains an attracting hypothesis, at present. When proven, this shift in conceptualization would implicate that the goals of treatment may also shift. Preventing disease progression in migraine has already been added to the traditional goals of relieving pain and restoring patients' ability to function (Loder and Biondi, 2003; Silberstein, 2000). If the brain lesions of migraineurs have a significant clinical correlate, preventing the accumulation of brain lesions may become an additional goal of treatment. The association of stroke with frequency of migraine attacks suggests that migraine, especially MA, prophylaxis may actually reduce migraine-related stroke risk, and opens the issue of whether prophylactic drugs that decrease such a risk (i.e., antihypertensives) might be the best option in these cases. At present, data are too limited to recommend the use of antiplatelet drugs to reduce the risk of stroke in migraineurs. Emerging treatment strategies to prevent disease progression, including risk factor modification, preventive therapies, and the early use of acute treatments, will be an important focus for future investigations (Loder and Biondi, 2003; Scher et al, 2002).
Conclusions
Strong arguments support the hypothesis that the relationship between stroke and migraine is more than coincidental. The link between MA and cerebral ischemia, indicated by epidemiologic observations, appears to be stronger among young but may persist in the elderly. In contrast, the evidence is very weak for MO. Although recent findings suggest the hypothesis of migraine as a progressive brain disorder, data are still too scarce to draw any conclusion. Identifying the population with migraine at highest risk of stroke should be the first step toward risk reduction and the goal of future research. At present, from the available data, the overall absolute risk of stroke among young migraine patients seems to be fairly low.
Footnotes
The authors state no duality of interest.