
Abstract
Introduction
Glenohumeral dislocations present a challenging management dilemma in austere settings where patient transport time may be prolonged. Expeditious reduction is preferable, but treatment is commonly expected to take place within a hospital or comparable facility. Through a novel shoulder injury program, professional ski patrollers trained as emergency medical technicians (EMTs) have diagnosed and reduced anterior shoulder dislocations using biomechanical techniques without sedation or analgesia for over 20 y. Summary records have been maintained to track the performance and safety of this program.
Methods
Five hundred forty-six records of winter sports-related shoulder injuries from 2009–10 to 2019–20 were retrospectively analyzed to determine the assessment performance and dislocation reduction efficacy of EMTs, with the intent of ascertaining whether EMT-trained practitioners can reliably and safely diagnose and reduce anterior shoulder dislocations without premedication in a remote and resource-limited setting.
Results
EMTs identified anterior shoulder dislocations with 98% sensitivity and 96% diagnostic accuracy. The overall success rate of reduction attempts was 86%, or 88% when limited to confirmed anterior dislocations. Two fracture-dislocations and 4 misdiagnoses were manipulated. No instances of iatrogenic harm were identified, and no patients who underwent successful reductions required ambulance transportation.
Conclusions
With appropriate education and within a structured program, EMT-trained practitioners can reliably and safely diagnose and reduce anterior shoulder dislocations using biomechanical techniques without premedication in remote and resource-limited environments. Implementation of similar programs in austere settings has the potential to improve patient care. Further, using biomechanical reduction techniques may reduce reliance on procedural sedation irrespective of care setting.
Introduction
Glenohumeral dislocations present a challenging management dilemma in situations where prehospital transport time may be prolonged. Expeditious relocation can relieve pain, ease reduction difficulty, and reduce the persistence of related neurovascular complications, 1 -4 but it is widely held that such reduction efforts should take place in a hospital setting, utilizing prereduction radiographs and procedural sedation or significant analgesia.1,2,5-7
This dilemma is especially relevant to winter sports enthusiasts. Shoulder dislocations rank among the top 5 specific injuries for which skiers and snowboarders seek care, with an estimated incidence that is notably higher than that of the general population. 8 -11 Further, many ski areas are located a substantial distance from the nearest hospital or comparable facility, creating the potential for significant delays to definitive treatment. During the 2021–22 winter season, there were a record 60.7 million recreational visits at the 473 ski areas across the United States.12,13 With reports estimating a rate of 2.6 injuries per 1000 visits, 14 and 3 to 6.5% of ski and snowboard injuries being glenohumeral dislocations,9,15 the importance of slope-side shoulder dislocation management cannot be overlooked.
Through a novel shoulder injury program, professional ski patrollers trained as emergency medical technicians (EMTs) have diagnosed and reduced anterior shoulder dislocations (ASDs) without the benefit of imaging or premedication for over 20 y. There is limited available literature on standardized protocols for the assessment and treatment of traumatic shoulder dislocations in austere settings.16,17 As such, we will provide details of this program. Moreover, there are few studies concerning prehospital shoulder reduction set within the unique healthcare systems of the United States, few studies that explore the diagnostic performance of nonadvanced practice clinicians, and, to our knowledge, no quantitative investigations of established reduction programs utilizing practitioners trained as EMTs. Therefore, this study is distinct in its care setting and its analysis. The intent is to demonstrate that the diagnosis and reduction without premedication of ASD can be performed safely and reliably by EMTs in a remote and resource-limited setting.
Methods
This retrospective analysis of 541 shoulder injury-related summary records (Figure 1) was approved by the Rocky Vista University Institutional Review Board and deemed exempt from full review or consent requirements. Permission for internal data use was granted by both Wolf Creek Ski Patrol (WCSP) and Wolf Creek Ski Area (WCSA).
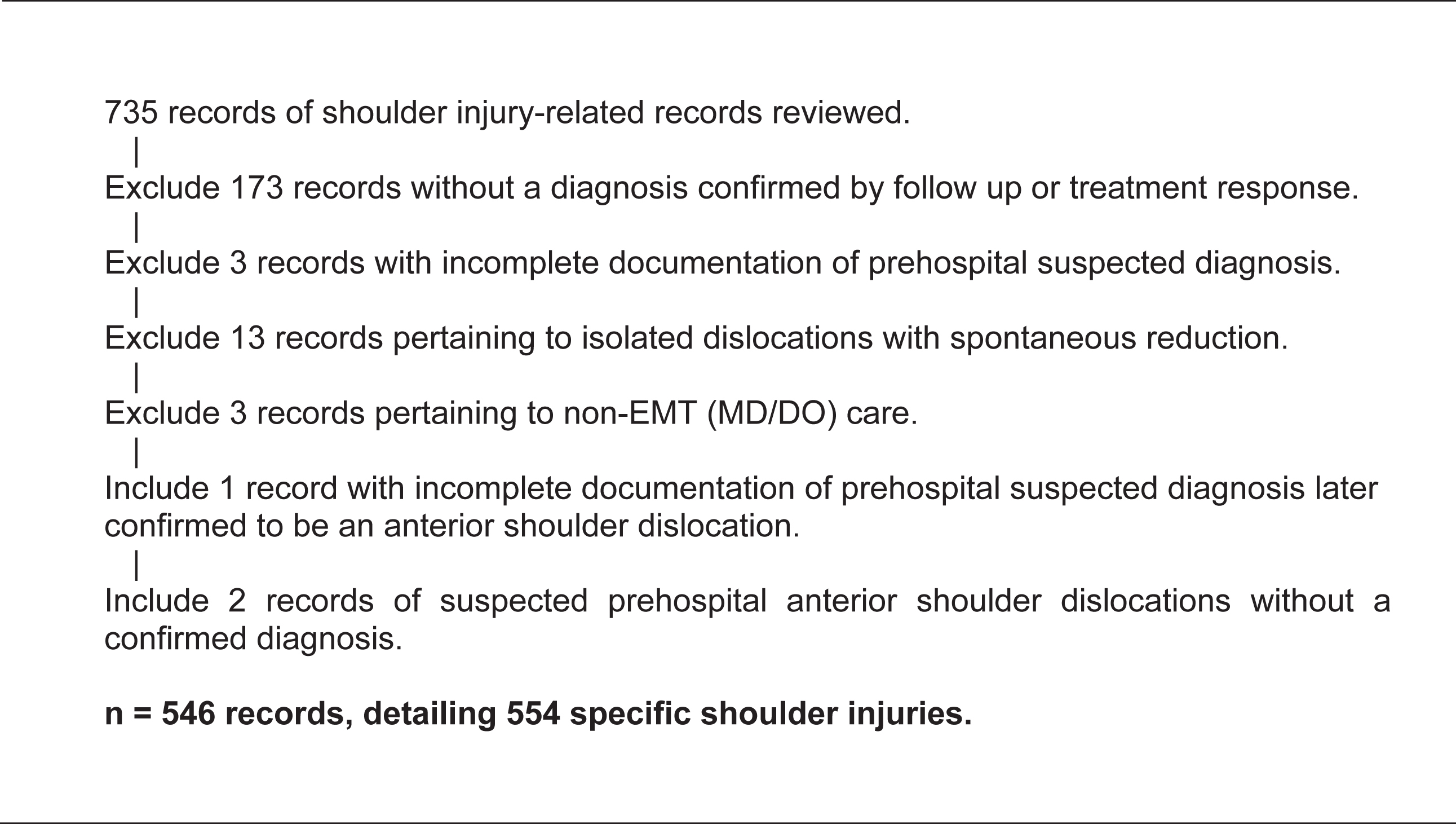
Data exclusion and inclusion criteria. Summary records from all shoulder-related injuries that presented to Wolf Creek Ski Patrol from 2009–10 to 2019–20 were compiled and reviewed. Number of total injuries exceeds number of total summary records due to records detailing multiple injury etiologies or bilateral injuries. EMT, emergency medical technician.
This study is set at WCSA, a remote mountain in Southwest Colorado with a ski patrol comprised entirely of professional rescuers certified as EMTs, EMT-Intermediates, and EMT-Paramedics. WCSP provides emergency medical services to all reported injuries and medical complaints within the ski area. It maintains an Advanced Life Support presence and can administer opioids when indicated. WSCP also possesses a scope of practice waiver granted by the Colorado Department of Public Health and Environment permitting the closed reduction of ASD.
The shoulder injury program permitted by this waiver operates with defined assessment and treatment protocols, structured training, and regimented internal certification. All patrollers on staff receive annual training from Medical Directors on the diagnosis of shoulder injuries by history and physical examination. To be considered for shoulder technician certification, patrollers must demonstrate reliable clinical judgment and have previously assessed a minimum of 20 shoulder injury patients. Once selected as program candidates, patrollers receive additional training from established shoulder technicians, including education on glenohumeral anatomy and instruction on biomechanical reduction techniques. Following this training, candidates assist in 5 reduction procedures, then perform 5 reduction procedures under direct observation of certified shoulder technicians. Additionally, candidates must demonstrate proficiency in pertinent documentation and patient education to receive final approval from WCSP’s Medical Section Chief.
When responding to a shoulder injury, patrollers perform an initial and focused assessment on scene, including a neurovascular exam of the affected extremity. They then stabilize the shoulder in the patient’s position of comfort and provide transportation to the First Aid Room at the base of the mountain, where the shoulder is exposed after the patient has been removed from the elements. There, patrollers use a decision support checklist (Figure 2) to work through common differentials and determine a prehospital suspected diagnosis in accordance with 5 shoulder injury categories. These categories are not mutually exclusive, and a patient may have multiple suspected diagnoses. If a shoulder dislocation is suspected at any point, a shoulder technician is dispatched to rendezvous with the responding patroller(s). In cases where assessment suggests an isolated ASD, an attempt at reduction is offered to the patient. Prior to initiating manipulation, the procedure is explained, risks and benefits are discussed, and written consent is obtained.
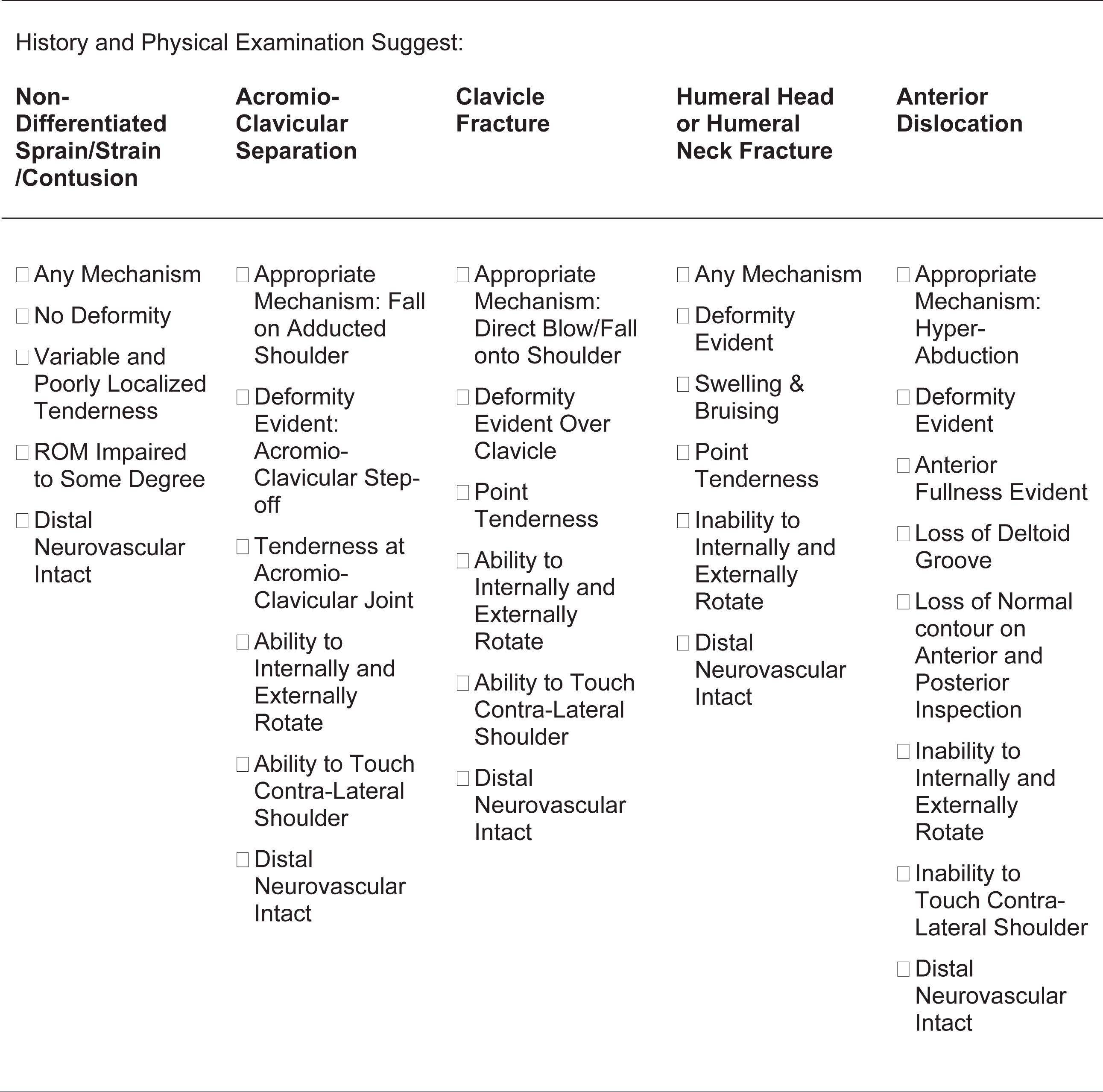
Prehospital assessment support checklist. Clinical support tool used by Wolf Creek Ski Patrol to guide and document history and physical exam-based prehospital assessment. ROM, range of motion.
The reduction techniques utilized by the program are scapular manipulation, external rotation, and the Cunningham Technique (Figure 3). These modalities are extensively described elsewhere and were selected for their simplicity, efficacy, and atraumatic nature.1,3,7,9,18-24 The use of 3 distinct but complementary techniques allows attempts at ASD reduction regardless of extremity position on presentation or patient body habitus. WCSP shoulder reduction protocols intentionally avoid the use of sedation and analgesia before or during any reduction procedure to allow full patient feedback regarding their discomfort, as an increase in symptoms may suggest a clinically significant occult injury or possible misdiagnosis. Protocols do not provide specific guidance on modality selection or limitations as to the use of multiple techniques or procedural duration; these decisions are left to the clinical judgment of the shoulder technician.

Biomechanical reduction techniques. Cunningham Technique (left), external rotation (center), and scapular manipulation (right). These modalities are utilized by emergency medical technician-trained practitioners on Wolf Creek Ski Patrol to reduce isolated anterior shoulder dislocations. All photographs are of simulated patient encounters. Photos by B. Pringle.
After the completion of reduction attempts, regardless of outcome, a focused neurovascular exam is performed, and patients are offered analgesia and disposition appropriate to their condition and level of pain. This can vary substantially, from patients declining oral nonsteroidal anti-inflammatories and being discharged after successful reductions, to patients requiring intravenous opioids and arrangements for ambulance transportation in cases of failed reduction attempts. Additionally, the injured extremity is immobilized, and the patient is advised to seek immediate hospital evaluation.
All patients presenting to WCSP with shoulder injuries have their care documented on a dedicated shoulder injury form that supplements their standard chart. Additionally, shoulder injury patients permit release of medical information related to their acute injury as part of their written consent for care. After discharge or transfer, patrol staff makes a minimum of 3 attempts to obtain a definitive diagnosis and disposition from the destination hospital, or from the patient directly. Follow-up findings are recorded on the shoulder injury form and are reviewed by WCSP Medical Directors. Quality assurance and improvement oversight is carried out monthly by the patrol’s Medical Section Chief and seasonally by Medical Directors. For this, deidentified summary records are maintained on all shoulder injuries. Since the 2009–10 season, this data has been maintained digitally in Microsoft Excel (Microsoft, Redmond, WA) spreadsheets.
WCSP uses clinical signs of a successful reduction as a surrogate for confirmation of a prehospital diagnosis of ASD when hospital follow-up and radiographic confirmation are not available. For confirmation of reduction, all the following must be present: normalization of preprocedural visual deformity; marked reduction or elimination of pain; and ability to internally rotate, externally rotate, flex, and extend the shoulder. The perceived clunk of a reduction is not a requirement but instead considered an encouraging sign if present.
Since certain glenohumeral injuries are common findings after a successful reduction and do not alter acute management,7,25 follow-up findings suggestive of a Hill-Sach’s deformity, Bankart lesion, or nondisplaced greater tuberosity fracture are not included in the humerus fracture category when classifying injuries for summary recordkeeping. For confirmation of a prehospital diagnosis classified as a nondifferentiated sprain/strain/contusion, WCSP uses successful follow-up from either the receiving facility or the patient suggesting absence of any other injury etiology as verification.
Summary records of shoulder injury-related patrol responses were compiled from the 2009–10 to 2019–20 winter seasons. This time frame was selected to capture all digitally maintained data from prior to the COVID-19 pandemic, during which WCSA/WCSP operations were dramatically affected. The summary records from one season, 2015–16, were lost in digital form, but a printed version was located and transcribed. Records were systematically reviewed by a fourth-year medical student with training and prior experience in data abstraction. This review was then audited and corroborated by an emergency medicine physician. Decisions regarding unclear record entries were made jointly.
Data was collected using Microsoft Excel. Suspected diagnosis category classification(s), time of report, procedural times, utilization of ambulance transport, incidence of iatrogenic harm, and confirmed diagnosis(es) were extracted from the summary records. Demographic information was also collected including patient age, documented sex, and equipment type used.
Records detailing incidents in which isolated dislocations spontaneously reduced prior to manipulation, records detailing care with in-person involvement of physicians, and records with incomplete diagnosis data that were insufficient for analysis were excluded. However, 3 records pertaining to ASD that would have been excluded due to incomplete diagnosis data were included in the analysis to prevent an overestimation of the diagnostic accuracy of EMTs. Two of these records listed a prehospital suspected diagnosis of ASD and were then lost to follow-up. The third record deviated from the program’s categorical diagnostic approach, with a prehospital suspected diagnosis listed as “fracture,” and was confirmed to be an ASD on follow-up. All 3 were treated as misdiagnoses.
Assessment sensitivity and demographics for each shoulder injury category were analyzed, as was the accuracy of prehospital suspected diagnoses of ASD. For reduction procedures, success rate, time from report to procedure initiation, procedural duration, instances of manipulation on misdiagnoses and fracture-dislocations, instances of iatrogenic complications, patient disposition, nature of follow-up, and demographics were analyzed. Summary records did not include data regarding the modalities utilized in cases of ASD reduction, preventing analysis. Continuous data are presented as mean±SD (range). Relevant proportions are reported as percentage (95% CI). Associations are reported as (P, odds ratio [95% CI]). Statistical analysis was completed using MedCalc v.20.215 (MedCalc Software, Ostend, Belgium). Statistical significance was defined as P<0.05.
Results
Five hundred forty-six records, detailing 554 shoulder injuries, were available for analysis after exclusion and inclusion criteria were applied. Table 1 summarizes EMT assessment performance and demographics for shoulder injury categories. EMTs assessed ASD with 98% (95% CI, 95–100%) sensitivity. Age of ASD was 35±16 (11–80) y, with an 89% (95% CI, 83–94%) male predominance that differed significantly from all other shoulder-related incidents (P=0.02, odds ratio=2.3 [95% CI, 1.3-4.2]). No substantial difference in incidence was noted between skiers and snowboarders. Lower EMT assessment sensitivity was attained with other injury etiologies. Notably, humerus fractures were identified with 46% (95% CI, 31–62%) sensitivity. Age of humerus fractures was 45±21 (9–75) y, with a 59% (95% CI, 44–74%) female predominance that differed significantly from all other shoulder-related incidents (P<0.0001, odds ratio=6.58 [95% CI, 3.3–12.9]).
Confirmed shoulder injuries vs prehospital assessment
The Other Injury Etiology column allows the analysis to reflect the minority of confirmed injuries that exist outside of the Wolf Creek Ski Patrol shoulder injury classification system. It includes 2 posterior glenohumeral dislocations, 4 scapula fractures and 2 unknown diagnoses that were suspected to be anterior glenohumeral dislocations with the patients lost to follow-up.
One confirmed anterior dislocation was suspected to be a posterior dislocation, another had an incomplete prehospital suspected diagnosis; it was included to prevent an overestimation of emergency medical technician assessment sensitivity.
Table 2 summarizes EMT assessment and reduction procedures on confirmed and suspected ASD. For confirmed ASD, reduction success was 88% (95% CI, 83–94%). Two successful procedures were performed on fracture-dislocations; both fractures were missed on prehospital assessment, and both patients were >50 y. However, there were no instances of worsening neurovascular abnormalities related to manipulation identified on follow-up. Prehospital suspected diagnosis of ASD was 96% accurate (95% CI, 92–99%), with diagnostic confirmation by either hospital follow-up or clinical response to treatment. Three percent of suspected ASD were misdiagnoses, and 1% was lost to follow-up. Of the misdiagnoses, 2 were determined to be acromioclavicular separations, and 2 were isolated proximal humerus fractures (both fractures were suspected on prehospital assessment, as concomitant to ASD). For all injuries suspected to be ASD, reduction success rate was 86% (95% CI, 80–92%). There were 3 reduction attempts on misdiagnoses, and 1 on a shoulder injury without a confirmed diagnosis. Ninety-seven percent of reduction procedures (95% CI, 94–100%) were performed on confirmed ASD diagnoses.
Anterior shoulder dislocations: prehospital diagnostic accuracy and reduction procedures attempted
Procedures on misdiagnoses include 2 acromioclavicular separations and 1 isolated humerus fracture.
Table 3 summarizes reduction procedures on confirmed ASD. For successful reductions, average time from report of injury to reduction procedure was 22±14 (0–80) min, and average procedural duration was 4±5 (0–35) min. Age among successes was 34±15 (11–80) y. Ambulance transport was not utilized by any patient who underwent a successful reduction. For procedure failures on confirmed ASD, average time from report of injury to attempted reduction was 25±12 (0–56) min, and average procedural duration was 13±6 (4–25) min. No differences were observed in time from report of injury to attempted reduction between successes and failures (P=0.20), but the duration of failed procedures was significantly longer (P<0.0001). Of note, 4 records did not detail the time when the failed attempt was aborted, preventing determination of procedural duration. Age for reduction failures was 39±21 (14–75) y. Ambulance transport was utilized by 3 (20%) of the patients with unsuccessful reduction attempts. Although this percentage was higher than that of successful procedures, the occurrence was too low within the sample for an accurate estimate of statistical significance.
Confirmed anterior shoulder dislocations: prehospital reduction without premedication efficacy
Discussion
Foremost in any discussion of expanding diagnostic and treatment practices to a prehospital setting are the parallel issues of necessity, accuracy, safety, and efficacy. During this study, WCSA averaged 193,152 recreational visits annually, with 2.6 injuries per 1000 visits, consistent with the injury rate reported at high-visitation resorts. 14 Of these incidents, 14% were shoulder-related injuries, marginally higher than the proportion reported elsewhere.26,27 For ASD, mean age and sex characteristics were similar to prior demographic findings.17,23,25,28-32 The 2 nearest hospitals are approximately 40 min away in ideal driving conditions. Transport time for ambulance response ranges from 80 to 90 min in ideal conditions. However, inclement weather often makes winter travel around WCSA slow and hazardous. Although we recognize that prereduction imaging and procedural sedation or analgesia should be considered by clinicians when available, this study’s remote location, limited resources, and relatively high incidence of shoulder-related injuries raise the question of whether adhering to these practices is optimal care. As such, exploring early management for shoulder dislocations is reasonable on both compassionate and clinical grounds.
For hospital-based closed reduction of ASD, radiographs are considered necessary for confirmation of the diagnosis, and to identify concomitant glenohumeral fractures.5,7,24 In this study, EMTs assessed ASD with 98% sensitivity and 96% accuracy without imaging. This accuracy is marginally lower than the reported 98% clinical assessment-based accuracy of physicians diagnosing traumatic ASD 33 and higher than the 83% accuracy of triage nurses. 34 Although the necessity of prereduction radiographic confirmation has been questioned, available literature and decision-making tools avoid the notion of bypassing imaging in the context of traumatic mechanisms, where the probability of concurrent glenohumeral injury is heightened.3,30,33,35 However, the foundation of this perceived need is not well supported, since these concomitant injuries rarely affect short-term management.25,36-38
A pressing question posed by this study is whether the attempted reduction of suspected ASD can be performed safely when significant fracture-dislocations or misdiagnoses cannot be ruled out by imaging. Although concern for displacing a fracture is reasonable, studies have shown that worsening radiographic abnormalities from reduction attempts are exceedingly rare31,33 and that biomechanical techniques, such as those used in this study, can be safe and effective even with clinically significant fracture-dislocations.21,28,32,38 Indeed, though there were 2 reductions of fracture-dislocations and 4 attempted reductions on confirmed or potential misdiagnoses in this study, there were no cases of suspected manipulation-related harm identified on follow-up. Although the traditional notion that routine radiographs are necessary is not supported by recent studies or our findings, we recognize the benefits that timely imaging may provide. Studies exploring the use of point-of-care ultrasound for ASD have shown promising results for confirming both diagnosis and reduction and defining the presence of concomitant fractures. 39 As point-of-care ultrasound becomes more widely available and economically feasible, utilizing it for imaging related to ASD may improve austere care in the future.
Regarding treatment efficacy, the reduction success rate for EMTs practicing without patient premedication was 86% overall and 88% considering only confirmed ASD. These rates are comparable to or higher than rates reported by some studies with physicians utilizing the same techniques in settings where premedication was available.18,21,40 This success rate may be attributable to early intervention because the time from report of injury to procedure initiation was 23 min, lower than the reported average time from injury to emergency department presentation. 41 Indeed, delay variables have been found to be the only independent predictors of reduction failure. 2 Although reports exist that higher degrees of success have been attained using the same modalities,22,32,41,42 such findings came from studies where radiographic injury confirmation was obtained prior to reduction attempts. It is reasonable to expect lesser efficacy when concern for manipulating an occult injury or misdiagnosis remains. In sum, the success rates observed in this study demonstrate that biomechanical techniques can be used effectively by appropriately trained EMTs.
It is noteworthy that the only prior study concerning ski patrol-based ASD reduction utilized analgesia not routinely available to prehospital providers in the United States. 17 Further, the WCSP program’s intentional avoidance of premedication may highlight a point where patient safety is better served by nonroutine care. Sedation readily achieves its intended purpose of relieving discomfort and promoting muscular relaxation, but it is not without its detractions. Many adverse medication events have occurred during sedation related to glenohumeral reduction procedures.3,28,43-46 Studies have noted concerning events, including apnea and bradycardia, in 8% of patients receiving ASD-related procedural sedation 45 and remarked on the “obvious danger” of sedating nonfasting patients. 19 In this respect, our findings may translate to a hospital setting because they support the conclusion that biomechanical reduction techniques and prompt relocation may eliminate the need for routine premedication, as has been proposed in other studies.3,19,21,22,28,29 By considering biomechanical reduction attempts prior to pursuing procedural sedation, especially in cases of early presentation, hospital-based providers may avoid the potential complications, increased staffing and resource requirements, and lengthened time of care that have been associated with sedation related to glenohumeral reduction procedures.3,28,43-46
As a pertinent aside, the 46% EMT assessment sensitivity of humerus fractures was lower than that of other shoulder injury etiologies. Additionally, humerus fractures were uniquely noted to have a higher mean age than other shoulder injury categories and a statistically significant female predominance. Pairing this age trend and sex predominance with the relative EMT assessment performance presents a point for possible improvement. If these demographic variables are integrated into program protocols and training, increased awareness and consideration could mitigate the possibility of manipulating a potential misdiagnosis.
Lastly, there are 2 points that may be of substantial importance to patients in a prehospital setting. First, the 113 patients who underwent successful early reduction procedures were spared an idealized minimum of 40 min of further discomfort from continued dislocation during transport. Second, patients with successful reductions were, as an entire cohort, free of the financial and logistical burdens of ambulance transportation, as none required outside emergency medical services.
Limitations
This study has several limitations. It is a retrospective review of a program that has been in place for over 20 y. As such, there is no control group to compare the diagnostic and treatment performance of EMTs to commonly accepted providers in an equivalent environment. Importantly, we also recognize that discontinuous care and variances in follow-up make it impossible to rule out the possibility of unidentified procedure-related iatrogenic harm. Additionally, this study’s reliance on a data set abstracted by several individuals over many years introduces further limitations, as inconsistencies in documentation and missing data create ambiguities and exclusions that could affect study findings. Moreover, inter-rater reliability was not assessed. We also recognize the potential for observation bias from a perceived need to document all shoulder injuries, including those that would be considered insignificant outside of a formal shoulder injury program, resulting in an overestimation of incidence. Additionally, time of report is not a perfect surrogate for time of injury, leading to an underestimation of time to treatment. Also, the specific reduction techniques utilized by practitioners were not noted in summary records and thus not addressed in this study. Lastly, it is noteworthy that the WCSP shoulder program has low practitioner turnover. Consequently, external validity may be limited to similar agencies. Prospective studies of EMT-trained practitioners utilizing these protocols, studies of these protocols being utilized within other care environments, such as hospital triage or rural ambulance services, and screening and deidentification of individual WCSP patient charts to obtain data on the utilization and efficacy of specific reduction modalities could add insight beyond our findings and should be pursued in the future.
Conclusions
The results of this study suggest that, with appropriate education and within a structured program, EMT-trained practitioners can reliably and safely diagnose and reduce ASD without premedication in resource-limited environments. Implementation of similar programs in austere settings has the potential to improve patient care. Further, these results support the conclusion that the use of biomechanical reduction techniques decreases reliance on premedication to facilitate reduction procedures. Consequently, these techniques may be beneficial in a variety of medical settings.
Footnotes
Acknowledgments
We thank WCSA, WCSP, Pagosa Springs Medical Center, Rio Grande Hospital, Molly McDonald, and Dr Mark Payton.
Author Contributions: study concept and design (BP, GH); program design (GH, TM, JR); acquisition of data (BP, GH, TM, JR); analysis of data (BP, GH, TM, IZ); drafting of manuscript (BP); all authors participated in critical revision of drafts and approved the final manuscript.
Financial/Material Support: None.
Disclosures: None.