
Abstract
With the recent development of neonatal medicine, the number of children with medical complexities (CMCs) is increasing. Outdoor activities are important for their psychosocial development, and the principles of accessibility should be addressed. We report the experience of 2 CMCs’ high-altitude mountaineering with the necessary support. The participants were a 3-y-old girl with cerebral palsy, symptomatic epilepsy, and a ventriculoperitoneal shunt (Child A) and a 6-y-old girl who underwent bilateral Glenn operations at 11 mo for hypoplastic left heart syndrome (Child B). The support staff consisted of 4 doctors, 1 nurse, 5 nonmedical staff , 3 members from a mountaineering association, and 2 people from an oxygen company. The climbing schedule was 2 days. On the first day, we took a bus to a hut at an altitude of 2450 m and stayed overnight to acclimatize to the altitude. On the second day, we took the beginner’s route, which took 3 h to climb 500 m, and our team made an attempt on the summit. During the attempt, Child B panicked. Although her lung sounds did not raise suspicions of pulmonary edema, we decided to leave the mountain with her because her transcutaneous oxygen saturation decreased. Child A had no apparent health problems and made it to the summit. Although CMCs’ alpine climbing requires careful planning and staffing considering the risk of high-altitude sickness, our case suggests the feasibility of such activities with CMCs as part of accessibility.
Introduction
With the advancement of medical treatment, the mortality rate of children at birth has decreased, increasing the number of children with medical complexities (CMCs). 1 CMCs can now live at home using medical devices such as ventilators. However, support for these children’s growth and development through experience outside home is easily limited physically and psychologically due to concerns for deterioration of their physical condition. Therefore, CMCs’ families tend to have a different relationship with society, and social support for both CMCs and their families is still insufficient. 2
Because of their unique characteristics, CMCs are restricted from the normal experiences that many healthy children enjoy, such as play and travel. Previously, only a limited number of activities were identified as being potentially effective. Meanwhile, a previous study at our facility has suggested that a visit to an amusement park, such as Disneyland, may make the family and surrounding medical personnel more optimistic about such outings and was found safe to travel the park with sufficient preparation, potentially leading to improvement in the development of CMCs. 3
Outdoor activities are expected to have a positive effect on children. 4 This is because they have been shown to improve children’s cardiopulmonary function, build strong bones and muscles, help them control their weight, and reduce symptoms of anxiety and depression.5,6 Therefore, exploring the possibility of performing outdoor activities is meaningful for CMCs.
Orange Home-Care Clinic and Orange Kids’ Care Lab in Fukui City, Fukui Prefecture, Japan, provide daytime care and schooling support for children, including CMCs. We focus on the growth and development of CMCs by delivering challenging experiences that are often restricted for them. We have been going out not only to nearby places, such as beaches, but also places outside the prefecture. As part of outdoor activities, we attempted high-altitude mountaineering to climb the Tateyama Mountain Range (Oyama, 3003 m above sea level) near the prefecture with 2 CMCs. Tateyama has been the object of mountain worship since ancient times and is considered one of the 3 sacred mountains of Japan. Mount Oyama is regarded as paradise in Buddhism.
Case Report
A 3-y-old girl (Child A) and a 6-y-old girl (Child B) and their parents participated in this climbing trip to summit the Tateyama Mountain Range’s Mount Oyama. The support staff consisted of 15 adults: 4 doctors from the clinic of the same corporation, 1 nurse, 5 nonmedical staff members belonging to the Care Lab, 3 from the Toyama Alpine Club, and 2 from an oxygen company. In case of an emergency, the climbing team decided to use a service to call an emergency helicopter.
Child A had cerebral palsy, symptomatic epilepsy due to severe neonatal palsy, and a ventriculoperitoneal shunt due to hydrocephalus after intraventricular hemorrhage. The only medical device used was a nasogastric tube, and she also visited the pediatric outpatient department at a general hospital, where her epilepsy was carefully monitored. She has difficulty with verbal communication but can communicate her discomfort by crying. Before the climb, the clinic asked the neurosurgery department at the general referral hospital about the risks to the patients. These were deemed to be acceptable.
Child B underwent bilateral Glenn surgery at 11 mo for hypoplastic left heart syndrome. She was discharged from the hospital at the age of 1 y and 5 mo and started home-visiting medical care and nursing. At 2 y and 5 mo, she underwent Fontan surgery and started using Care Lab after her discharge. When she was 4 y and 11 mo old, she took a trip to Kume Island, Okinawa Prefecture, by airplane with the clinic and Care Lab staff. She was on a ventilator when she was first discharged from the hospital, but her condition had stabilized. In the fourth month after the discharge, she was switched to a speech cannula, and 2 months before the climb, the tracheal cannula was removed, leaving only a tracheal hole. She was able to walk a short distance with a guide. Because of her unique gestures, she was suspected of having some developmental traits, but no diagnosis was made. Her behavior gradually eased through interaction with others.
The climbing schedule was 2 days in autumn 2021 (Figure 1), and as the temperature at the time of climbing was about 10°C, we wore warm clothes. On the first day, the team drove to a mountain lodge in Tateyama Murodo (about 2450 m above sea level). Prior to arrival, we stopped for an hour in Midagahara (about 1930 m above sea level) on the way to Murodo. The healthcare providers and the children’s parents carefully observed the children for any changes compared with their usual condition, but no particular changes were observed.
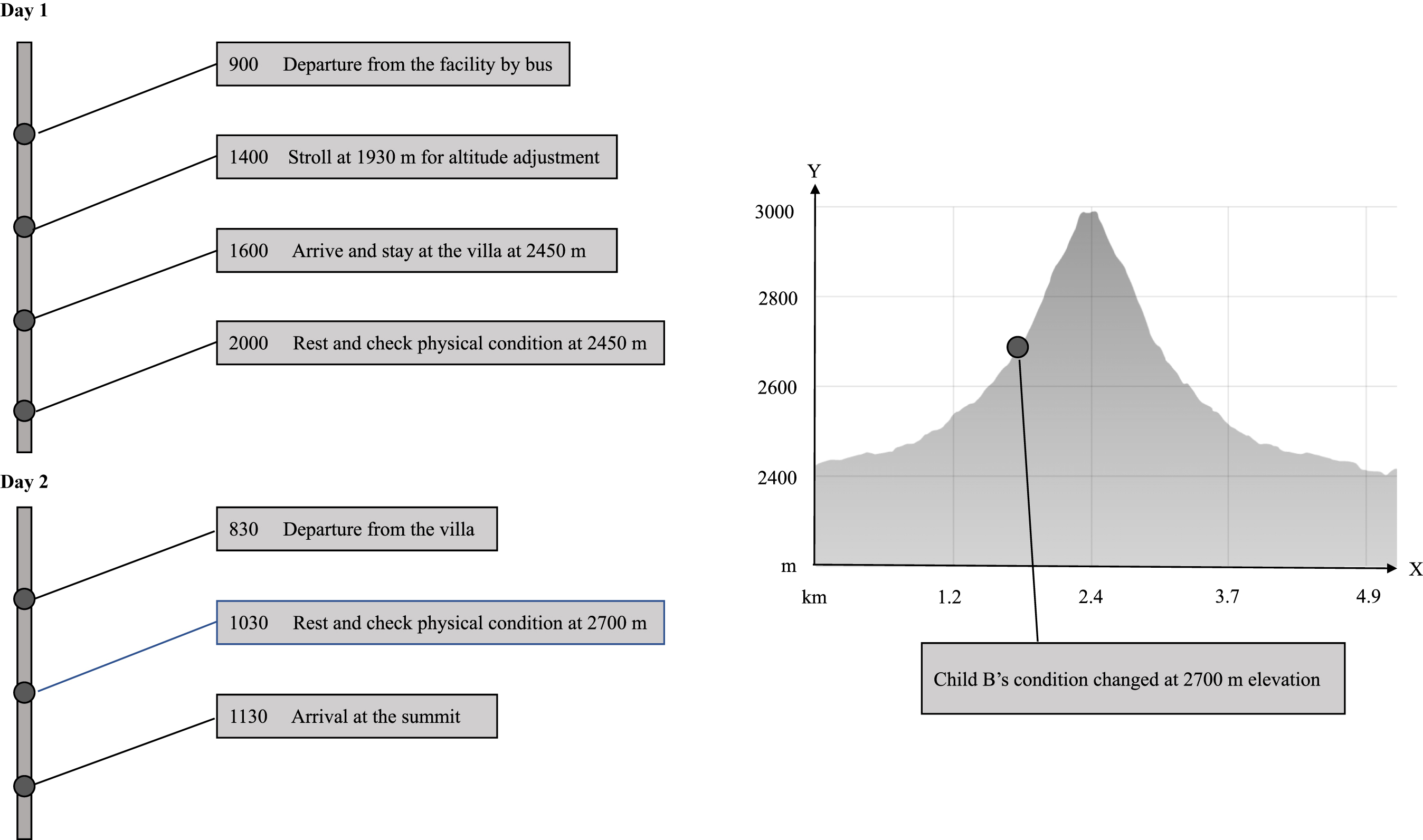
Itinerary to the summit of Mount Oyama. The team stopped for 1 h at 1930 m to observe the children’s condition and stayed overnight at 2450 m. Child B’s condition changed at 2700 m, and Child B descended the mountain.
On the second day, we aimed to reach the summit of Mount Oyama. We climbed 500 m on the beginner’s route in 3 h. On the second day’s morning, the 2 children’s physical condition was the same as usual. Each child was assigned a staff member, and the 2 teams headed for Ichinokoshi (about 2700 m above sea level), the middle point of the climbing route. The trail to Ichinokoshi was relatively well maintained, and the children traveled in a rickshaw-like vehicle with a wheelchair attached to a pole (Figure 2). At around 2650 m, Child A’s wheelchair was damaged and became difficult to use; therefore, the staff made the decision to carry her. At Ichinokoshi, Child B’s respiratory status changed: her oxygen saturation (SpO2) dropped to 76%, pulse rate increased to 110 beats/min, and respiratory urgency was observed, but lung sounds were normal. Furthermore, 3 L/min of oxygen was used for 10 min. However, this was only discharged near the mouth as a mask and cannula were not worn because of the patient’s reluctance. No improvement was observed. As a result, the team could not rule out the possibility of high-altitude pulmonary edema or the possible effects of right-to-left shunting caused by pulmonary hypertension. Therefore, the team immediately descended the mountain. During the descent, Child B’s condition and her observations gradually recovered; her SpO2 was 90%, and her pulse rate fell to 100 beats/min as they reached the starting point. After that, they went for a walk and ate near Murodo; by then, her mood and condition had returned to normal. There were no apparent abnormalities in Child A, and the team decided to summit Mount Oyama (Figure 3). At the summit, Child A had no findings of decreased SpO2, respiratory urgency, or vomiting. There was no obvious change in her condition as she did not appear to be in any distress from the parents’ point of view. They descended after spending 20 min on the summit. Overall, the only trouble throughout the trip was the change in Child B’s condition, and there were no physical changes or injuries to the staff.

Climbing to Ichinokoshi. The children traveled in a rickshaw-like vehicle with wheelchairs attached to a pole. Participants provided consent for publication of the photograph.

Climbing from Ichinokoshi to the summit of Mount Oyama. One of the children is shown being carried by a staff member. Participants provided consent for publication of the photograph.
Discussion
We report here our attempt to climb a 3000-m peak with 2 CMCs and a support team. While only 1 of the children reached the summit, we found that climbing activities with CMCs could be carried out safely. Importantly, healthcare providers and the children’s parents carefully observed the children for any changes compared with their usual condition, but no particular changes were observed. Climbing the sacred mountain proved to be a safe and meaningful experience for the CMCs as well as their families and support staff.
Key to our success was a heightened awareness of altitude sickness. Rapid ascent puts one at risk of acute mountain sickness, high-altitude cerebral edema, and high-altitude pulmonary edema. In addition, the children’s cardiovascular and respiratory backgrounds were additional risk factors for altitude sickness. Since neither of the children could accurately communicate symptoms of headache, dizziness, and lightheadedness, we recognized that the diagnosis of altered mental status would be problematic. In order to reduce this risk, we chose a peak of modest altitude and ensured that we took regular breaks during our ascent. In addition, we were accompanied by family members and carers who knew the children very well. A clear descent plan was put in place in the event of difficulties. This was undertaken successfully for Child B.
The long-term impact of this experience is difficult to quantify. However, a previous study showed that through social participation, children and their families gained confidence and provided encouragement to set future goals. 7 Indeed, one of the participants commented, “I have never done anything with my family that gave me such a sense of accomplishment. I want to continue to share this experience with others through our activities.”
We present the experience of 2 CMCs who safely undertook climbing of a 3000-m peak. Children with medical complexities tend to have very limited social interaction compared with other children. These experiences allow them to safely connect with others through a shared experience of mountains.
Conclusion
We present 2 cases of CMCs who safely experienced climbing of 3000-m peak. CMCs tend to have limited social participation and experiences as a family and children. Depending on the child’s condition, it may be possible to take up a similar challenge by preparing, managing physical needs, and collaborating with specialists in fields other than medical professionals. In addition, building a strong relationship of trust with the medical team on a daily basis is an indispensable element for taking on challenges. It is necessary to gather knowledge to reduce the barriers for CMCs and their families to connect with society through such endeavors.
Footnotes
Acknowledgments
The authors express sincere gratitude to all the staff members involved in this case.
Author Contributions: initial draft of the manuscript (HM, TO, AO); proofreading of the manuscript in English (YK, TT); data analysis and preparation of the manuscript (HM, TO, YK, AO, HB); lead author and submission responsibility (HM). All authors critically reviewed and revised the manuscript. HM had full access to the data, controlled the decision to publish, and accept full responsibility for the work.
Financial/Material Support: None.
Disclosures: AO received personal fees from MNES Inc and MRT Inc, respectively, unrelated to the submitted work. TT received personal fees from MNES Inc and Bionics co ltd, unrelated to the submitted work. There are no further conflicts of interest to declare.