
Abstract
Introduction
Ski patrols are tasked with substantial challenges: distance from definitive care, complex extrications, and winter environments. Rules for US ski patrols stipulate that ≥1 persons be trained in basic first aid, but no further regulations regarding the specifics of provided medical care exist. This project investigated patroller training, patient care, and medical direction of US ski patrols through a survey of ski patrol directors and medical directors.
Methods
Participants were contacted via email, phone, and personal contacts. After consultation with known ski patrol directors and medical directors for question guidance, 2 separate institutional review board-approved surveys were designed: 1 for ski patrol directors and 1 for ski patrol medical directors, containing 28 and 15 qualitative questions, respectively. The surveys were distributed with a link to the encrypted Qualtrics survey platform. After 2 reminders and 4 mo, results were downloaded from Qualtrics into an Excel spreadsheet.
Results
Twenty-two responses from patrol directors and 15 from medical directors were received. The response rate is unknown. Outdoor emergency care certification was the minimum medical training required by 77% of the study participants. Twenty-seven percent of surveyed patrols belonged to an emergency medical service agency. Fifty percent of 11 surveyed ski patrols had a medical director, 6 of whom were board certified in emergency medicine. All surveyed medical directors stated that they assisted with patroller education, and 93% assisted with protocol development.
Conclusions
The surveys demonstrated variability in patroller training, protocols, and medical directorship. The authors questioned whether ski patrols would benefit from increased standardization of care and training, quality improvement programs, and medical directorship.
Keywords
Introduction
During the 2018 to 2019 winter season, ski areas in the United States experienced 59.3 million skier visits,1,2 creating a need for medical care because of both trauma and general medical illness. In order to address these needs, ski areas employ medical units, called ski patrols. In addition to technical rescue skills, ski patrollers are tasked with the responsibility of responding to medical incidents within, and often around, a ski area’s geographical location.
The majority of the total capacity for skiing in the United States is provided by public land that is leased from the US Forest Service, which requires that at minimum, ≥1 persons be trained to provide first aid/emergency care at the basic life support level. Basic life support is defined as medically accepted, noninvasive procedures that are used to sustain life, 2 such as cardiopulmonary resuscitation and automatic external defibrillation. Beyond basic life support, however, there is no national standard for medical training, care, or medical oversight requirement for ski patrols.
Ski patrols are not federally recognized as a part of the formal emergency medical services 3 structure, and no uniform regulations with regard to medical equipment, facilities, leadership structure, transportation, medical oversight, communications, quality improvement, or liability exist at this time.
The National Ski Patrol is a US-based, nonprofit organization that provides education and accreditation to emergency care providers in the mountain recreation industry. 4 The National Ski Patrol sponsors a medical training program called Outdoor Emergency Care, which is a 120-h medical certification course 5 focusing on both prehospital medicine and on-mountain (summer and winter) patient transport. While the National Ski Patrol requires the Outdoor Emergency Care training for membership, not every ski patrol is a National Ski Patrol member, which leaves the unaffiliated patrols without a medical requirement above that of the US Forest Service’s rule of staffing at least 1 basic life support-trained provider on the mountain.
It is generally agreed that safe and effective medical care requires a continuous evaluation of provider training, protocols, and patient care. As ski patrollers don uniforms and are compensated for their medical work, many argue that ski patrollers are acting within the official healthcare system as prehospital medical providers 6 and that their training, protocols, and oversight should be evaluated in line with other emergency medical service providers. Furthermore, because ski patrols provide prehospital medical care that exceeds the scope of Good Samaritan or Basic First Aid practice, 7 many experts argue that ski patrols, by definition, practice emergency medical services, and should, therefore, become formally affiliated with emergency medical services agencies.8,9
While there has been 1 study that investigated the basic medical care provided by ski patrols in 9 ski areas in Utah, 10 there have been no studies that investigated ski patrols, their medical direction, and their protocols throughout the entire US region. The purpose of this project was to characterize the medical training, patient care, scope of practice, medical direction, and oversight of US ski patrols through a survey of both ski patrol directors and, if applicable, their medical directors.
Methods
The project was approved by Oregon Health and Science University’s institutional review board (#21906).
Two separate surveys were written: 1 for ski patrol directors and 1 for ski patrol medical directors. Both ski patrol directors and medical directors were consulted on the survey’s design. Survey participants were recruited through emails to industry contacts, outreach to ski area staff via published web page contact information, advertisement in a snow science journal, and Twitter. Participants were guaranteed that survey results would be published in aggregate form and thus be anonymous. All US ski patrol directors and medical directors were eligible to complete their respective surveys. A gift card raffle was offered to all survey participants as an incentive. At least 2 attempts were made to contact individuals. Responses were collected from November 29, 2020 through March 20, 2021. As the study’s recruitment email was passed informally and via mass email between patrol and medical directors, response rates could not be calculated because of an unknown total distribution number, but the authors estimated that the surveys reached ∼200 qualified respondents.
The surveys were delivered and analyzed using the Qualtrics survey platform. All data were designed in a qualitative fashion: data were categorized by question type, and the relative results were calculated and analyzed using Excel.
Results
Thirty-seven survey responses were received. Twenty-two survey responses were collected from ski patrol directors (Figure 1). Most surveyed ski patrols were associated with ski areas located >16 km (10 mi) from the nearest hospital but <160 km (100 mi) from the nearest level II trauma center. Most surveyed ski areas had ≤500,000 skier visits per year and responded to 100 to 500 medical incidents per year (Table 1). The ski patrols in this survey varied greatly in size, make-up, minimum requirements, and agency affiliations (Table 2).
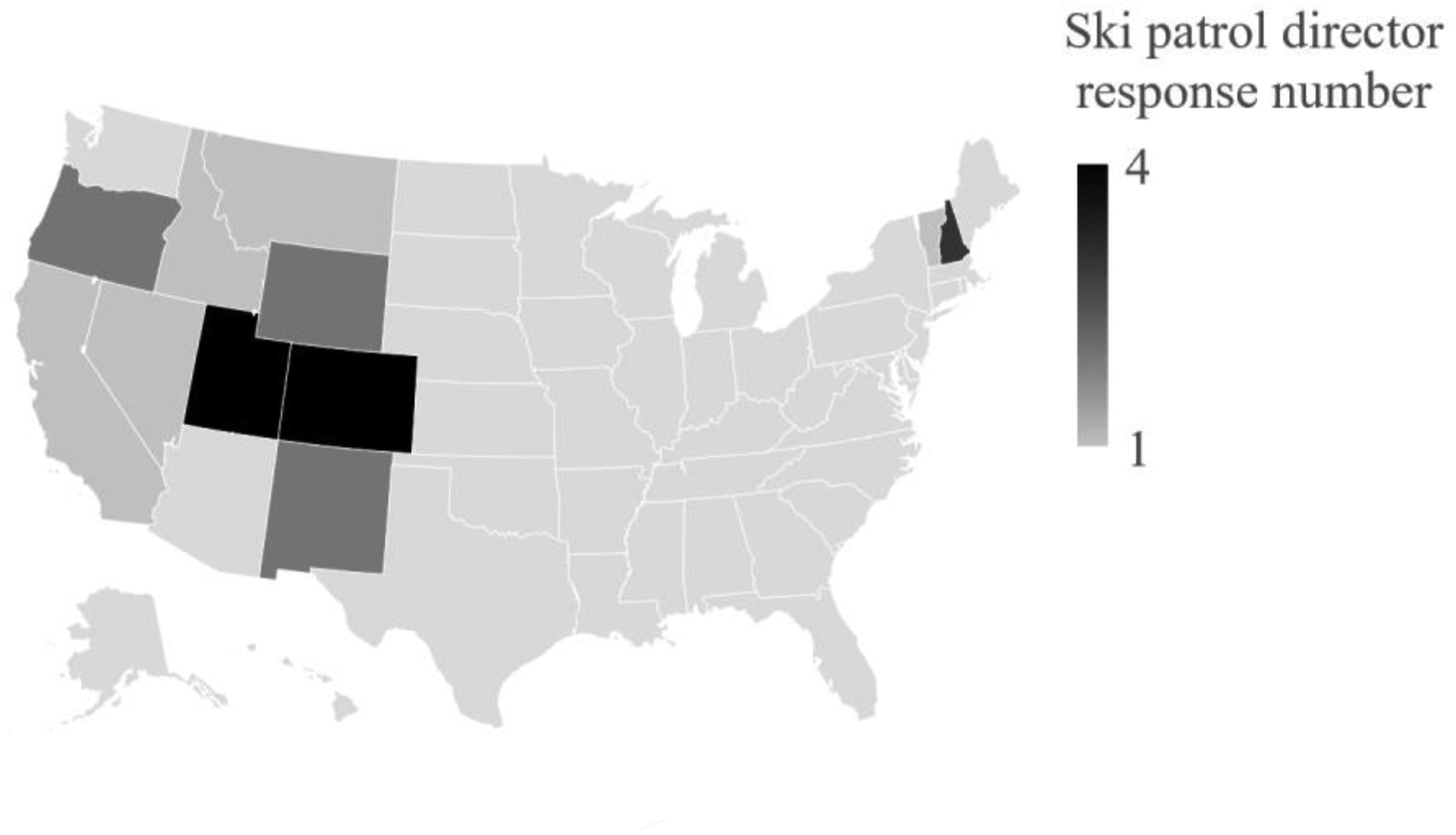
Location of ski patrol director survey respondents by US state. The highest concentration of respondents is located in the intermountain US region.
Ski area demographics
Ski patrol demographics
One half of the surveyed ski patrols hosted an on-site medical clinic. In addition to what is considered traditional ski patrol medical equipment, such as toboggans, oxygen, basic airway devices, backboards, and extremity splints, surveyed ski patrols cited the use of additional equipment; fewer than half utilized advanced airway devices, and only 1 stated the use of a mechanical chest compression device (Table 3).
Medical training/care
OEC, Outdoor Emergency Care; EMT, emergency medical technician; WFR, wilderness first responder; RN, registered nurse; NP, nurse practitioner; PA, physician assistant; MD, medical doctor; DO, doctor of osteopathy; ALS, advanced life support; EMS, emergency medical service.
The incident command system was utilized by the majority of surveyed ski patrols in at least some capacity, with most using the incident command system for both avalanche and major medical responses. The incident command system was also used in lift evacuation, mass casualty incidents, and out-of-area rescues. As a supplement to both private transport and ground ambulances, the majority of surveyed ski patrols cited helicopter use for medical transport at a rate of 1 to 5 times per season. Indications for patient transport via helicopter ranged from minimum requirements of open fracture to 1 patrol that stated that they only transported if neurosurgical intervention was anticipated.
The majority of ski patrols participated in out-of-area responses. Insurance coverage for out-of-area response varied among the surveyed ski patrols: many were covered by their ski area’s insurance, while a minority sought coverage from their local search-and-rescue/sheriff, their respective fish and game agencies, or state-licensed emergency medical service agencies (Table 4). The majority of the surveyed ski patrols employed additional protocols beyond their baseline standard of care. Protocols pertaining to cervical collar and backboard use were among the most common additional protocols utilized (Table 5).
Medical equipment/resources
LUCAS, Lund University Cardiopulmonary Assist System; RN, registered nurse; PA, physician assistant; NP, nurse practitioner; MD, medical doctor; DO, doctor of osteopathy.
Ski patrol systems and operations
SAR, search and rescue; EMS, emergency medical services; TBI, traumatic brain injury.
Fifteen survey responses were received from ski patrol medical directors (Figure 2). Among the surveyed ski patrol medical directors, emergency medicine was the most common specialty. Most surveyed medical directors had not completed any specific training for their role as a ski patrol medical director, but some had completed training as an emergency medical technician in outdoor emergency care or had pursued fellowships in medical directorship. Wilderness first responder or wilderness emergency medical technician training was completed by a minority.
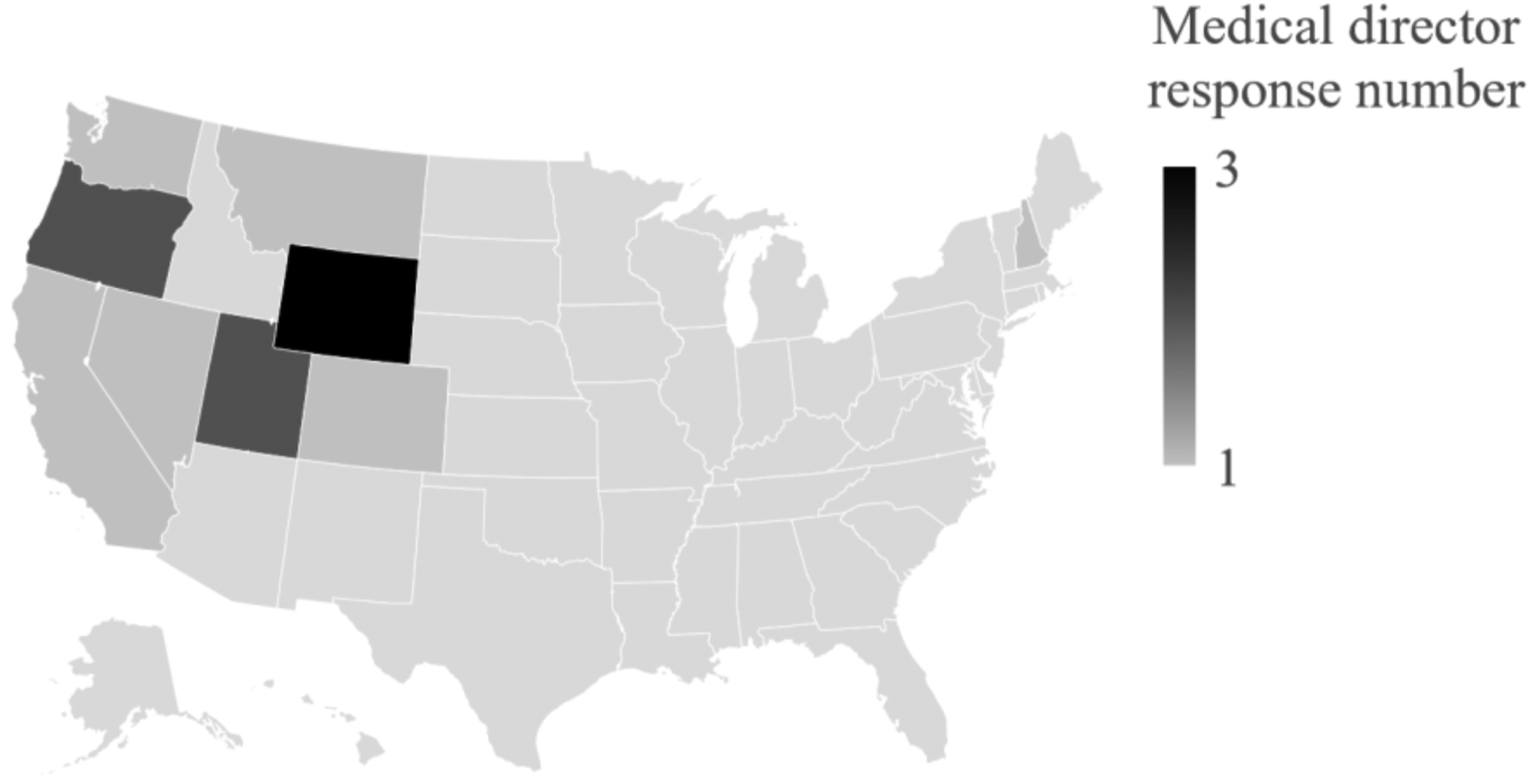
Location of ski patrol medical director respondents. The highest concentration of ski patrol medical director responses is located in the western US region.
The hours worked by ski patrol medical directors varied from just a few hours per month to 40 h per week. In addition to phone contact, most of the ski patrol medical directors surveyed stated that they were available on scene, by radio, and in person at the clinic. The vast majority of surveyed ski patrol medical directors wrote or expanded upon their ski patrol’s medical protocols. Most respondents were involved in quality improvement activities for their ski patrol, and all surveyed ski patrol medical directors stated that they assisted with continued medical education for their ski patrol (Table 6).
Medical director training and work
EMS, emergency medical service; DiMM, Diploma in Mountain Medicine; FAWM, Fellowship in Academy of Wilderness Medicine; MFAWM, Master Fellowship in Academy of Wilderness Medicine; WEMT, wilderness emergency technician; WFR, wilderness first responder.
Discussion
This project investigated aspects of ski patroller training, medical care, and medical direction of ski patrols across the United States. The surveys demonstrated an appreciable variation in ski patrol demographics, patroller training, and medical direction.
Ski area and patrol demographics, such as annual skier visits, distance to definitive care, and patrol roster size, did not appear to affect whether the surveyed ski patrols staffed volunteers in addition to paid patrollers or whether the surveyed ski patrols employed advanced medical practitioners able to practice up to their scope of practice. No surveyed ski patrol used only volunteer staff. While usually not able to perform all of the duties of a paid patroller (ie, avalanche mitigation) and with varying capabilities among ski patrols, a volunteer pool can allow ski areas to accommodate the ebb and flow of busier times. If used, paramedics can provide advanced life support services, such as endotracheal intubation as well as vasopressor and other medication administration, both on the slopes and in clinics. 11
The majority of the surveyed ski patrols are members of the National Ski Patrol, which requires outdoor emergency care certification as every ski patroller’s minimum medical training. Regardless of National Ski Patrol membership, most of the surveyed ski patrols also require outdoor emergency care certification as their minimum medical certification. Ski patrols in this survey that did not require outdoor emergency care certification as their minimum training were most commonly found to require an emergency medical technician certification. Compared with emergency medical technician training, outdoor emergency care is considered to include less training in geriatrics, pediatrics, medical illness, and medication administration 5 but provides additional training in skills that are considered more specific to ski patrolling, such as orthopedics, environmental emergencies, and winter transport. 4
Ski patrols are not considered part of the United States’ emergency medical service structure nationwide, and less than one third of the ski patrols in this survey are affiliated with an emergency medical services agency. Some states require ski patrols to have emergency medical service affiliation (Maryland), while others (Idaho) allow ski patrollers to engage in medical care without a license, 3 further demonstrating the varied medical structure regarding ski patrols in the United States.
The outdoor emergency care certification has traditionally provided many ski patrols with their protocols, which help to ensure a minimum medical service base. However, individual ski patrol protocol modifications for emerging data, such as backboard utilization, historically occurred before the outdoor emergency care curriculum was able to adapt. Protocol development from a qualified source, such as a medical director, can assist a ski patrol in providing the medical care that is most specific and beneficial for their individual situation. 7 Of the 15 medical directors surveyed, all but 1 have expanded their ski patrol’s protocols and 13 perform quality improvement tasks, demonstrating how medical directors can play an active role in furthering and monitoring the quality care provided by ski patrols. While only one half of the surveyed ski patrols had a medical director, 19 of the 22 surveyed ski patrols stated that they expanded their medical protocols. This data point calls into question the provided medical care: if a patrol is not strictly following an official medical training and certification program, such as outdoor emergency care, and if there is no medical director determining best practices, then how is safe and effective treatment ensured?
The majority of surveyed ski patrol medical directors were board certified in emergency medicine, whose training aligns with the acute and often traumatic nature of ski patrol medicine. The often austere and wilderness-like prehospital conditions that can be found in some ski areas and the adjacent backcountry terrain 12 make further training in wilderness and austere medicine for a ski patrol medical director a reasonable consideration, which multiple respondents stated that they have pursued. The medical direction of emergency medical services can be divided into direct (cell phone, radio, in person) and indirect (protocol development, provider education, quality improvement) work. 6 While great variability was found in the specialty and further training that a medical director has undergone, all 12 of the surveyed ski patrol medical directors contributed to patroller education, demonstrating that medical direction can play an effective role in furthering ski patrollers’ medical knowledge.
Limitations
This study has limitations: most prominent is the potential bias due to this its limited sample size and the spatial distribution of respondents. Difficulties in achieving a higher number of responses were likely due to the timing of survey release and the short time frame that the survey was open. The survey was released in December 2020, which occurred at an extraordinarily busy time for ski patrols and their directors:it was the first year of the COVID-19 pandemic, which required new logistics for medical care at a time with increased skier visits in conjunction with the holiday season. Ideally, the survey would have been released in August or September, which would have allowed for an entire US ski season window for survey response. As many ski areas close up in April and patrol directorship can often be a seasonal means of employment for smaller ski areas, the survey was closed after a mere 4 mo of distribution. Because most responses originated from the western region of the United States, it is possible that a selection bias toward western US ski patrols exists. Given the small and regionally biased survey responses, the results of this study must be approached with caution. A larger survey with a more balanced national distribution would likely better characterize the training, medical care, and direction of US ski patrollers.
This study did not evaluate the quality of ski patroller training, provided medical care, or medical direction of US ski patrols, and no conclusion regarding the effectiveness, costs, or benefits of these aspects can be made from this study.
Conclusions
Despite its limitations, the authors believe that this survey indicates variety in the training, medical care, and medical direction of US ski patrols. The survey signifies that medical directors, if present, do play an active role in a patroller’s medical education and protocol modification. Given the heterogeneity in ski patrollers’ medical training, resources, and oversight demonstrated, this survey does not indicate evidence of consistency in the training or medical care that ski patrol patients will receive. This issue raises the question of whether further standardization and quality assurance measures, through either official affiliation with emergency medical services or formal medical direction requirements, should be sought within the ski patrol industry.
Footnotes
Acknowledgements
Acknowledgments: The authors thank Dr Barron Reyes and Lee Watson for initial project input; ski patrol director, Joe Calder, for help with survey distribution; and Dr Emma DeLoughery for manuscript design.
Author Contributions: study concept and design (LLF, OSL, TGD); data acquisition (LLF, TGD); data analysis (LLF, OSL, TGD); drafting and critical revision of the manuscript (LLF, TGD, EEJ); approval of the final manuscript (LLF, OSL, TGD, EEJ).
Financial/Material Support: None.
Disclosures: None.
Presented virtually at the Wilderness Medical Society’s 2021 Summer Conference, June 27 to July 1, 2021.