
Abstract
Introduction
The quality of cardiopulmonary resuscitation (CPR) is critical in increasing the probability of survival with a good neurologic outcome after out-of-hospital cardiac arrest. In an austere environment with a potentially salvageable patient, bystanders or first responders may need to provide chest compressions for a prolonged duration or during physically challenging transportation scenarios. Consequently, they may be at risk of fatigue or injury, and chest compression quality may deteriorate. The study sought to assess whether or not access to and utilization of a mechanical compression device (Lund University Cardiopulmonary Assist System) was feasible and not inferior to manual compressions while extricating and transporting a patient from a ski slope.
Methods
Variable 3-person ski patrol teams responded to a simulated patient with out-of-hospital cardiac arrest in a nonshockable rhythm. Using a mannequin and CPR quality monitor, performance during manual CPR was compared with that of a mechanical compression device. This is a prospective, crossover analysis of CPR quality during extrication from a ski slope. Across 8 total runs, chest compression fraction, which is the proportion of time without spontaneous circulation during which compressions occurred, and high-quality CPR, as measured by appropriate rate and depth, were compared between the 2 groups. Extrication times between the 2 groups were also measured.
Results
There was no difference in compression fraction between the manual (91.4%; 95% CI [86.8–96.1]) and mechanical arms (92.8%; 95% CI [88.8–96.8]) (
Conclusions
Mechanical CPR devices are noninferior for use in ski areas during initial resuscitation and transportation. Compared with manual CPR, mechanical CPR would likely improve the fraction of time performing high-quality CPR.
Keywords
Introduction
Sudden cardiac death (SCD) is the leading nontraumatic cause of death during downhill skiing. 1 While traumatic arrest rates have remained stable over the years, the incidence of SCD has increased since the 1980s. 2 With upward of 100 million recreational visits to mountainous areas on a yearly basis, 3 of which approximately 60 million are visits to inbound ski areas, the aging patient demographic of the United States comes with a corresponding increase in SCDs during these activities.
Ski patrols are composed of rescuers with a variety of medical and rescue backgrounds who serve as emergency responders at most inbound ski areas. Ski patrols, much like conventional emergency medical services (EMSs), typically provide initial resuscitative efforts at the point of collapse for SCD patients. Some patients require extrication from their point of collapse even if unable to achieve return of spontaneous circulation (ROSC) at the mountainside. Ski patrols have different approaches to the delivery of cardiopulmonary resuscitation (CPR) during extrication and toboggan transport. Some use a 3- or 4-person rescue team that requires 1 person to continue providing chest compressions during transport off the mountain. This is performed while atop the patient in a toboggan while being pulled by another ski patrol member, which is logistically challenging and physically demanding and comes with added safety concerns during transport. Previous studies have demonstrated that CPR quality declines when it is performed while actively moving, 4 more commonly failing to reach the appropriate depth and speed recommendations compared with stationary CPR.
Given the challenges of the environment, it may seem that cardiac arrest on a ski slope carries an abysmal survival rate because of prolonged extrication times and resource-limited on-scene capabilities. However, a prospective analysis found just the opposite. The 30-d survival rate after cardiac arrest on a ski slope was 3 times higher than that in the general population (21% vs 6%, respectively). 5 The authors attributed this difference to the fact that the patients were statistically younger, more likely to have a shockable rhythm, and more likely to receive bystander CPR or early defibrillation.
Mechanical CPR device utilization has increased in recent years, although the literature supporting its efficacy compared with that of manual (hands-on) CPR is scant. In a 2020 meta-analysis, including multiple randomized control trials from 2006 to 2015, the clinical outcomes of the Lund University Cardiopulmonary Assist System (LUCAS) device vs those of manual CPR were similar in terms of ROSC, survival to hospital admission, survival to hospital discharge, and 30-d survival. 6 A similar article looking at a cluster trial found that there was no difference in survival and the cost-adjusted return on purchasing a mechanical CPR device was not apparent. 7 A retrospective analysis of 2 y of data from out-of-hospital cardiac arrest found improved odds of survival to the emergency department. 8 Although it was well known that traumatic cardiac arrest carries a grave mortality approaching 99%, 9 there have not been any large studies assessing mechanical CPR devices in traumatic cardiac arrest. The paucity of data supporting the benefits of mechanical device-assisted CPR has limited widespread adaptation, especially in small systems that cannot justify the cost in the absence of a clear benefit. However, many systems have adopted these devices because of ease of use, perceived benefit, and simplified maneuverability for providing CPR during transport. Prior manikin studies have evaluated the quality of mechanical CPR devices in wilderness transport settings using a Stokes basket, 10 in a sledge pulled by a snowmobile, 11 or in a helicopter, 12 and others have looked at manual CPR in a ski patrol toboggan 4 ; however, there are limited data on the quality of mechanical CPR in this setting. In a recent update to the Cochrane review, researchers did not find that using a mechanical CPR device was superior to manual CPR or consistently demonstrated either survival with good neurologic outcome or survival to hospital discharge. 13 They did suggest that mechanical CPR was a reasonable alternative when high-quality CPR was not possible or dangerous.
This study sought to determine if mechanical CPR is as effective as manual CPR at an inbounds ski area when administered by ski patrollers during ski toboggan transport. The primary outcomes were assessment of chest compression fraction (CF) and percentage of time spent performing high-quality CPR. These were the specific targets of this study, in line with American Heart Association guidelines and studies demonstrating improved coronary artery perfusion, ROSC, and survival to hospital discharge. 9 The secondary outcome was time spent extracting the patient from point of collapse to collection point for hand off to EMSs.
Methods
The institutional review board at Albert Einstein Medical Center, Philadelphia, reviewed the study protocol and approved the study as nonhuman subjects research. The study was conducted at Big Boulder Ski Area in the Pocono Mountain region of Pennsylvania. The study utilized a prospective, crossover design to assess 2 interventions in series under similar conditions. Data were collected prospectively for analysis.
The study utilized a full-torso commercial CPR mannequin with makeshift appendages dressed in ski outerwear and placed at the top of a ski run. On-duty ski patrollers, 8 staff in total, and the study authors participated in simulated resuscitation. The person performing compressions was switched for every manual trial to prevent fatigue and learning as a confounder. The ski patrollers had varying degrees of familiarity with mechanical CPR and, specifically, the LUCAS 3 device (Stryker Corp, Kalamazoo, MI, United States) prior to the study. Prior to the trials, the ski patrollers were briefed by the authors on the use of the mechanical CPR device and the study protocol. Because of the nature of the research, the ski patrollers and authors were not blinded to the interventions during each iteration. Feedback on CPR quality was not provided during the trials. The accompanying CPR quality monitor (Zoll R Series ALS, Zoll Medical, Chelmsford, MA) was packed in a water-resistant duffel bag, with only the leads exposed, to ensure device safety and reduce the risk of dislodgement.
After the staff felt comfortable with the organization of the trials, a 3-person rescue team would begin with a “witnessed collapse” and initiate on-scene CPR while preparing for transport. Study timing for data collection started after the rescue team witnessed the patient collapse and arrived on scene to begin to administer CPR. The mannequin was loaded with an automated external defibrillator in a toboggan to transport down the hill to the ski patrol base either with 1 rescuer in the toboggan performing CPR or with a mechanical CPR device attached (Figures 1 and 2; see online supplemental video). Beat-to-beat data regarding depth and timing of each compression were then collected and analyzed. High-quality CPR was defined as the percentage of time spent performing compressions at a rate of 100 to 120 beats/min at a depth of 2.5 to 5 cm (2–3 inches). Timing for CPR quality and CF calculation started at the first minute of CPR through the final destination and last complete minute of CPR. The terrain consisted of an average slope of 10° (18% grade) and a maximum slope of 21° (38% grade) over an estimated distance of 570 m (1870 ft).

A 3-person rescue team performing manual cardiopulmonary resuscitation during transport.

A 3-person rescue team utilizing the Lund University Cardiopulmonary Assist System device for cardiopulmonary resuscitation during transport.
Data were exported from the CPR quality monitor and analyzed using the Zoll RescueNet Code Review software. Data points of interest, including the proprietary CPR quality score (an algorithmically generated integer on a scale of 0–100 accounting for rate, depth, and release), were exported as an XML file, and analysis of the data was performed using Microsoft Excel (Figure 3). Data were stored on a secure server and shared over the authors’ institutional network. Averages were compared using the t-test with confidence intervals (CIs).
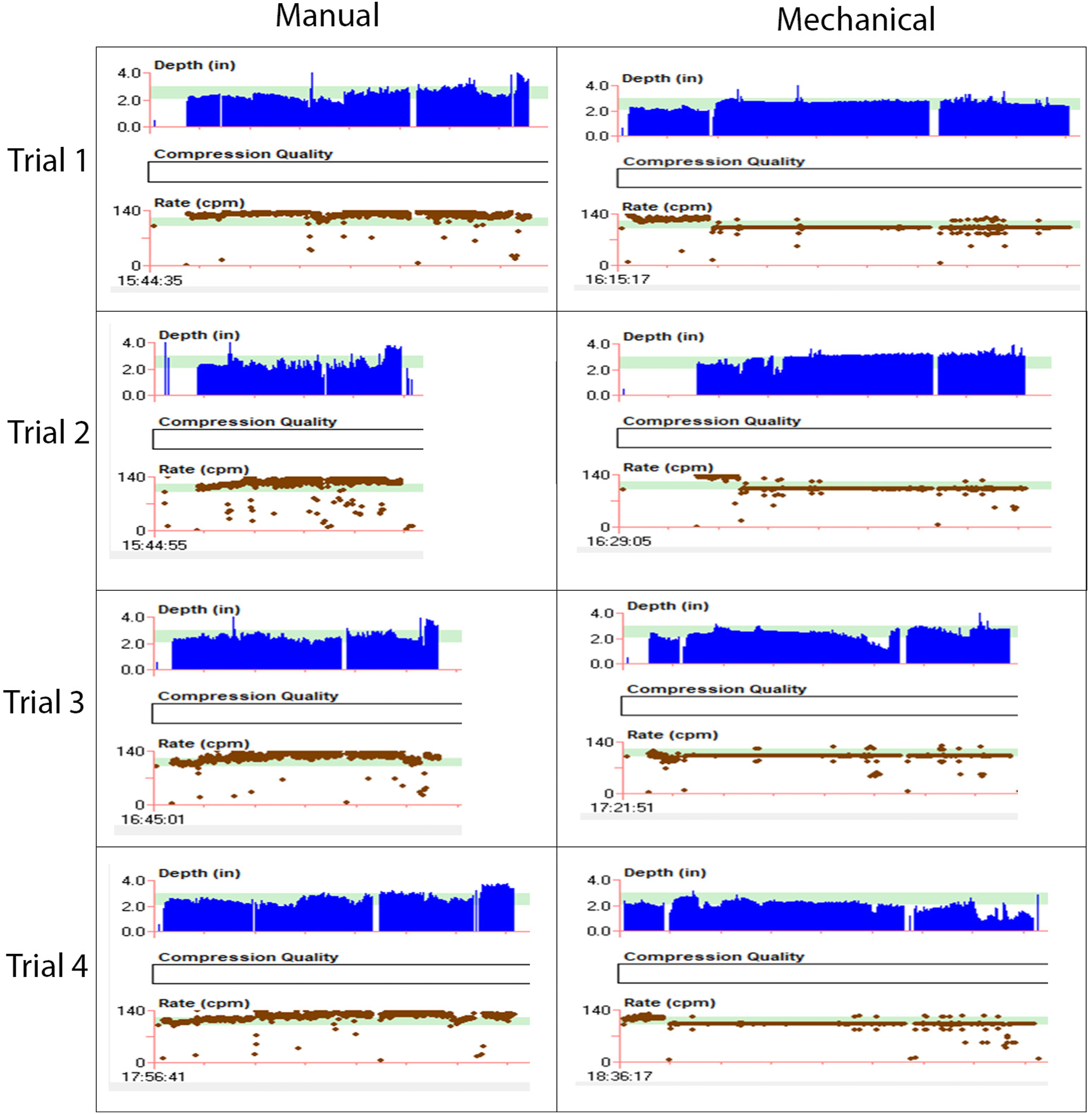
Manual vs mechanical trial beat-to-beat variation and composite graphs.
Results
There was no difference in CF between the manual (91.4%; 95% CI [86.8–96.1]) and mechanical arms (92.8%; 95% CI [88.8–96.8]) (
Summary of high-quality cardiopulmonary resuscitation a
CPR, cardiopulmonary resuscitation.
Discussion
The principles of EMS regarding CPR also generally apply to inbound ski areas: resuscitate where found, provide immediate CPR, defibrillate if there is a shockable rhythm, and do not transport until ROSC is achieved. However, in a subset of cases, a reversible cause is present or an intervention available that is not able to be corrected or provided in situ, respectively, mandating transportation to continue resuscitation. In this circumstance, the added complication of toboggan transportation and variable terrain adds significant complexity to the extrication compared with conventional EMS. Performing CPR becomes more difficult on a changing incline. The addition of accelerating and rotational motions while being transported downhill on a toboggan is difficult to account for when performing compressions. The center of gravity over the patient changes, not only from the grade of terrain, but also from any terrain obstructions, such as uneven snowpack or natural debris. Seemingly small irregularities lead to a sensation of instability and multiple human factors that alter the quality of CPR. The results of this study further corroborate the findings that manual CPR in a moving toboggan will likely result in an increased compression rate and inappropriate compression depth while having little impact on chest CF. 4 As a reflex favoring self-preservation, ski patrollers noted that they would bend their knees, bringing the center of gravity closer to the mountainside, but shift their arms overhead, impeding CPR quality.
This study provides evidence to support the practice of using mechanical CPR devices in the ski patrol setting using objective data on CPR quality during toboggan transport. Despite years of practice in ski areas worldwide, the evidence to support routine use of mechanical CPR devices is limited. Both mechanical CPR and manual CPR are effective for patients suffering medical cardiac arrest in inbound ski areas who require toboggan transport. Mechanical CPR can be superior to manual CPR and may improve logistical considerations that would likely be magnified over longer transport times. Although the difference in extrication time was statistically significant, there is likely minimal clinical significance in real-world scenarios. This study demonstrates that if a ski patrol team does include a mechanical CPR device in their rescue efforts, they can expect to add about 1 min to their total transport time. The added minute comes from applying the mechanical CPR device to the patient. The device used in this experiment came with a portable, plastic backpack with straps and was not difficult to transport. Implementing a mechanical CPR device was readily adapted to by the team and did not require extensive training as a potential barrier to entry. All training was “just-in-time” and performed within hours of application. The overall variation in CPR quality can be attributed largely to the change in compressor during each trial. The effect of cold temperatures on battery life is unknown. Under normal conditions, a fully charged, new battery is expected to last for 45 min continuously, per the device insert. In mechanical trial 3 (Figure 3), the piston moved from the target area due to shift of the device and required readjustment at the pulse check point.
There are multiple limitations to this study that require further investigation before suggesting practice-changing guidelines. The sample size included in the study was small and only involved 4 different CPR providers. The baseline characteristics of the CPR providers were not controlled for and may not accurately represent a cross-section of ski patrollers. The number of trials performed also limits the generalizability of the study. All trials were performed on the same day, same moderately pitched run, and under similar conditions, but different conditions and weather could have changed the outcomes. Frequent changes in weather, especially at altitude, can have dramatic effects on even menial tasks. Although considered, airway management variables, such as bag-valve-mask ventilation during transport, were intentionally excluded from the study to limit confounding variables. Ventilation is a real-world consideration that needs to be addressed on a case-by-case basis.
The study was performed using a plastic CPR mannequin and Zoll CPR quality monitor. The mannequin was a torso model, and even considering the added appendages, it does not have the dimensions, weight, or realism that complicate the coordination of transport. The standard CPR mannequin with attached extremities does not have arms capable of securing to the mechanical CPR device. This may have made it easier to perform CPR while in the toboggan or to maneuver the patient with the mechanical CPR device attached. Body habitus, additional layers of clothing, and many real-world variables exist in real patients that could confound the results. Chest wall compliance is different in a real person, as is adherence of the mechanical CPR device suction cup on the piston to the chest wall, particularly when using a CPR quality monitor.
The ski area we utilized was small compared with that of many resorts (approximately 600-ft vertical drop) and had a short extrication time of just under 10 min, although this can be expected to vary greatly with each mountain or ski run. Additionally, the ski area is not located at an altitude (approximately 610 m [2000 ft] at the summit); so, any complications due to hypoxia or high altitude could not be assessed. The study was performed on the same ski run, providing the team with some consistency and skill improvement over the course of the day, which would not be typical in a real-world setting. To mitigate this, we used a different compressor for each iteration. Auditory and visual CPR feedback from the CPR quality monitor, indicating the depth of compression and appropriate rate, was not made available during manual CPR trials, in keeping with the equipment typically available at this ski area.
Further, the study participants were not blinded to the objective of the trial and may have had preconceived notions about which option would inevitably be superior. No subjective data, such as a provider preference or prior familiarity with the mechanical CPR device, were collected. Statistical analysis was performed and analyzed by the same researchers conducting the experiment, which introduced the possibility of bias due to lack of blinding.
Conclusions
Utilizing a mechanical CPR device while extricating a patient in cardiac arrest from an inbound ski area may increase the time spent performing high-quality CPR with similar chest CF while having minimal impact on extrication time.
Footnotes
Acknowledgment
The authors thank Vail Resorts and Big Boulder Ski Patrol in Lake Harmony, Pennsylvania, for hosting them and accommodating their research team for the day. They thank Stryker Corporation for providing the Lund University Cardiopulmonary Assist System device in use for the day.
Author Contributions: research analyst (SLR); research concept, designer (RCO); approval of the final manuscript (SLR, RCO).
Financial/Material Support: Stryker Corporation provided the mechanical cardiopulmonary resuscitation device in use. They had no involvement in the conceptualization of the study, data collection, or analysis of the study results. Einstein Medical Center provided the cardiopulmonary resuscitation manikin and Zoll R Series ALS monitor. Big Boulder Ski Area provided ski patrol staff and equipment.
Disclosures: None.
Supplemental Material(s)
Supplementary material associated with this article can be found in the online version at