
Abstract
Objective
To compare the outcomes of patients with non-traumatic cardiac arrest (CA) who received early versus late mechanical cardiopulmonary resuscitation (CPR) with the Lund University Cardiac Assist System (LUCAS) device in the emergency department (ED).
Methods
This was a retrospective observational study in the ED of a single medical center performed from May 2018 to December 2019; 68 patients with CA were eligible. We grouped the patients according to the time to initiating LUCAS use after CA into an early group (≤4 minutes) and late group (>4 minutes).
Results
The rate of return of spontaneous circulation (ROSC) was higher in the early group vs the late group (69.2% vs 52.4%, respectively). The 4-hour survival rate was significantly higher in the early group vs the late group (83.3% vs 45.5%, respectively), and CPR duration was significantly shorter in the early group (23.3 ± 12.5 vs 31.1 ± 14.8 minutes, respectively).
Conclusion
Early mechanical CPR can improve the success of achieving ROSC and the 4-hour survival rate in patients with non-traumatic CA in the ED, considering that more benefits were observed in patients who received early vs late LUCAS device therapy.
Keywords
Introduction
Cardiac arrest (CA) is a major public health problem. Each year, approximately 424,000 patients develop out-of-hospital cardiac arrest (OHCA) in the USA; 130,000 in Europe, 210,000 in Japan, and approximately 3.7 million worldwide. The 1-year survival rate for these patients is as low as <5%.1–5
Administering high-quality chest compressions has been considered a key determinant for successful resuscitations. 5 The latest guidelines emphasize that chest compressions should be performed with adequate rate and depth, complete recoils, and minimized pauses.6–8 However, the quality of traditional manual chest compressions could gradually decline with prolonged resuscitation times. Studies have revealed that rescuers were unable to perform adequate compressions for more than approximately 1 minute before losing effectiveness. After 4 minutes, the rescuers achieved only approximately 30% efficacy in chest compressions. 9 Furthermore, effective manual chest compressions are generally difficult to perform during patient transportation. 10
Mechanical cardiopulmonary resuscitation (CPR) provides effective, consistent, and uninterrupted chest compressions that overcome the inevitable fatigue and interruptions of rescuers. However, previous studies have reported different outcomes of mechanical CPR between pre-hospital and in-hospital settings. In the pre-hospital setting, studies failed to demonstrate improved clinical outcomes with mechanical devices compared with manual CPR,11–14 whereas in the hospital setting, mechanical CPR was more effective than manual CPR. 15 The differences between studies of CPR in in-hospital and out-of-hospital settings might be related to differences in evidence quality or clinical factors. 16 , 17 Nevertheless, mechanical CPR is being used increasingly in emergency departments (ED) worldwide. In 2016, the proportion of patients with OHCA receiving mechanical CPR increased by more than four times in the USA, compared with 2010. 18 Thus, more studies are required to prove the efficacy of mechanical CPR in the ED.
In the present study, we analyzed patients who received mechanical CPR with the Lund University Cardiac Assist System (LUCAS 2 Chest Compression System; Jolife AB Inc., Lund, Sweden), which was initiated at different time points for non-traumatic CA patients resuscitated in the ED. The objective of this study was to evaluate the outcomes of LUCAS use in adult patients with CA in the ED.
Methods
Study design and participants
This was a single-center, retrospective observational study conducted in the ED. This study was reviewed and approved by the Medical Ethics Committee of Chengdu Third People’s Hospital (approval number: 2018-S-6). The committee waived the requirement for informed consent because of the retrospective design of the study. Medical records were reviewed to select eligible study participants who visited our ED between 1 May 2018 and 31 December 2019. The reporting of this study conforms to the STROBE statement along with references to STROBE and the broader EQUATOR guidelines. 19
Inclusion criteria
Inclusion criteria 20 , 21 were: 1) age ≥18 years; 2) patients with witnessed CA in the ED or OHCA before arrival to the ED with ongoing CPR; and 3) patients who received mechanical compression with the LUCAS device in the ED.
Exclusion criteria
Exclusion criteria 20 , 21 were: 1) a duration of >2 minutes from CA to manual chest compressions; 2) traumatic CA, including hanging; 3) pregnancy; 4) patients who received mechanical compressions before arriving at the ED; and 5) patients with incomplete data.
Study protocol
All patients were immediately treated with manual chest compressions until the LUCAS device was deployed. The CPR algorithm is outlined in Figure 1. According to the 2015 American Heart Association (AHA) guidelines update for CPR and Emergency Cardiovascular Care and the 2011 guidelines of the National Resuscitation Council, Singapore, a member of the Resuscitation Council of Asia, which is part of the International Liaison Committee on Resuscitation (ILCOR),22,23 the compressors were replaced every 2 minutes in our hospital. All patients received endotracheal intubation, monitoring of partial pressure of end-tidal carbon dioxide (PetCO2), invasive ventilator-assisted ventilation, and conventional rescue medications. The LUCAS parameters were a pressing depth of 5 to 6 cm and frequency of 100 beats per minute with the suction cup height appropriately adjusted for each patient. There were two steps when implementing LUCAS therapy: 1) place the backplate under the patient and continue compressions, and 2) connect the top portion of the device to the backplate, adjust the vertical position of the suction cup and pressure pad, and begin mechanical CPR. We defined the CPR interruption interval as the time from the trailing edge of the last manual chest compression to the leading edge of the first mechanical compression.
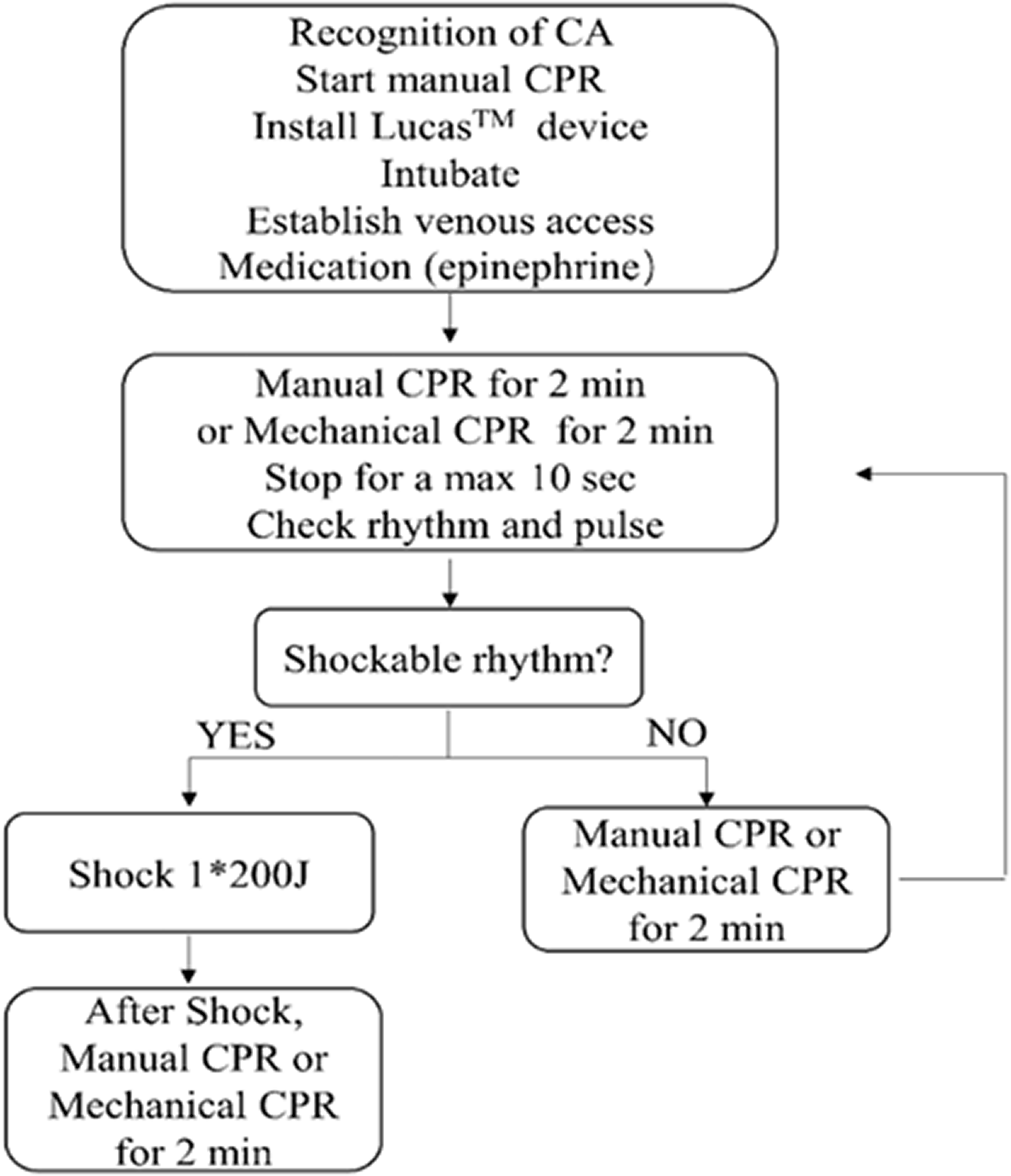
Mechanical CPR algorithm.
Our emergency medical and nursing staff underwent 4 hours of intensive training on the use of the LUCAS 2 device. Prior to this training, staff also received instructions on performing standard manual 30:2 CPR in accordance with the 2015 AHA guidelines update for CPR and emergency cardiovascular care and the 2011 guidelines of the National Resuscitation Council, Singapore.22,23 The staff were required to demonstrate proficiency in the skills of manual and LUCAS CPR in a training room environment, as well as continued proficiency at monthly intervals through supervised performance in training room environments and the production of rhythm strips.
Data collection and outcome measurements
We collected the patients’ demographic and clinical data. The definition of initial PetCO2 in CA is similar to the definition used in a previous study. 24 Arterial and venous blood gas samples were taken immediately on patient arrival at the ED and 15 minutes after initiating LUCAS use.
The patients were divided into two groups according to the time from initiating manual chest compressions to initiating LUCAS use as an early group (≤4 minutes) and late group (>4 minutes). The causes of CA were divided into cardiogenic and non-cardiogenic causes. Cardiogenic CA constituted acute myocardial infarction-related and/or primary ventricular tachycardia/ventricular fibrillation (VT/VF) and pulmonary embolism. Non-cardiogenic CA constituted metabolic, electrolyte imbalance, respiratory, or other causes.
The primary outcome was the sustained restoration of spontaneous circulation (ROSC, defined as the recovery of sinus or supraventricular heart rate with a palpable arterial pulse for at least 20 minutes), 13 , 18 , 20 , 21 ,25–27 admission, and 4-hour survival. Information after admission to the hospital was provided by the Hospital Information System’s (HIS) admissions data. We defined failure of resuscitation as follows: 30 minutes after resuscitation, the patient still suffered loss of consciousness, no response to external stimuli, dilated pupils, no light reflex, non-palpable aortic pulse, no measurable blood pressure, and no spontaneous breathing or effective heart rhythm.
Statistical analysis
Continuous data are presented as mean ± standard deviation and were compared by the t test. Categorical data are presented as percentage or rate and were compared by the χ2 test. SPSS software (version 15.0; SPSS Inc., Chicago, IL, USA) was used for analysis. P < 0.05 indicated statistical significance.
Results
Characteristics of the study participants and baseline clinical laboratory test results on ED arrival
We reviewed data for 149 consecutive patients with CA. After excluding 81 patients according to the predetermined criteria, 68 patients with CA were included for analysis; 42 patients with OHCA in the late group, 9 patients with OHCA in the early group, 4 non-ED in-hospital patients (CA in other departments), and 13 ED-witnessed CA patients in the early group. The factors related to CA and pre-hospital resuscitation in patients with OHCA are shown in Table 1. The duration of pre-hospital CPR and total CPR were significantly shorter for OHCA in the early group vs the late group (P < 0.05 for both). Regarding OHCA, only 9 patients were transferred quickly to the ED for early LUCAS use. There were no statistically significant differences in demographics, comorbidities, shockable rhythm, and interval from collapse to manual compression between the two groups. In our preliminary study (in press), univariate analysis showed significant differences between the ROSC group and non-ROSC group for the early use of LUCAS (≤4 minutes).
Factors related to CA and pre-hospital resuscitation in patients with OHCA between the early and late groups.

Results are means ± standard deviations or number(percentage).
Early group, Lund University Cardiac Assist System (LUCAS) CPR initiated ≤4 minutes after manual compressions; Late group, LUCAS CPR initiated >4 minutes after manual compressions.
CA, cardiac arrest; OHCA, out-of-hospital cardiac arrest; CPR, cardiopulmonary resuscitation.
Multivariate logistic regression analysis showed that early use of LUCAS (≤4 minutes) was an independent factor influencing ROSC (odds ratio (OR): 1.986; 95% confidence interval (CI): 0.298–13.223; P < 0.05). Therefore, according to the duration from initiating manual chest compressions to initiating LUCAS use, we assigned the patients to an early group (≤4 minutes; n = 26, 38%) and a late group (>4 minutes; n = 42, 62%) (Figure 2). The characteristics of the patients in the two groups are shown in Table 2. There were no statistically significant differences in demographics, comorbidities, duration of total CPR, and baseline laboratory data on ED arrival, between the two groups. Compared with the early group, patients in the late group had fewer un-shockable rhythms and received more epinephrine. Shockable rhythm was observed as an initial ECG rhythm in less than 3% of patients. The mean time from CPR to LUCAS use, as well as the number of patients across different time periods according to the minutes elapsed from CPR to LUCAS application, are shown in Figure 3.

Patient selection. Early group, Lund University Cardiac Assist System (LUCAS) CPR initiated ≤4 minutes after manual compressions; Late group, LUCAS CPR initiated >4 minutes after manual compressions.
Comparisons of the participants’ characteristics and baseline clinical laboratory data on ED arrival between the early and late groups.

ED, emergency department; Early group, Lund University Cardiac Assist System (LUCAS) CPR initiated ≤4 minutes after manual compressions; Late group, LUCAS CPR initiated >4 minutes after manual compressions; pH, blood pH.
PO2, partial pressure of oxygen; PCO2, partial pressure of carbon dioxide; CK-MB, isoenzyme of creatine kinase; PetCO2, partial pressure of end-tidal carbon dioxide; hs-cTnI: high-sensitivity cardiac troponin I; BUN: blood urea nitrogen.

Number of patients and the minutes interval from CPR to LUCAS device application
ROSC, admission, and 4-hour survival
As shown in Table 3, the percentages of patients with CA who achieved ROSC in the two groups were approximately 52.4% to 69.2%. Compared with the patients in the late group, more patients in the early group achieved ROSC and survived to admission, although with no significant differences. Additionally, longer pre-hospital resuscitation durations were associated with later LUCAS use and longer total CPR duration. The 4-hour survival rate was significantly higher in the early group vs the late group (P < 0.05). There were no surviving and discharged patients in our study.
Comparisons of the outcomes between the early and late groups.
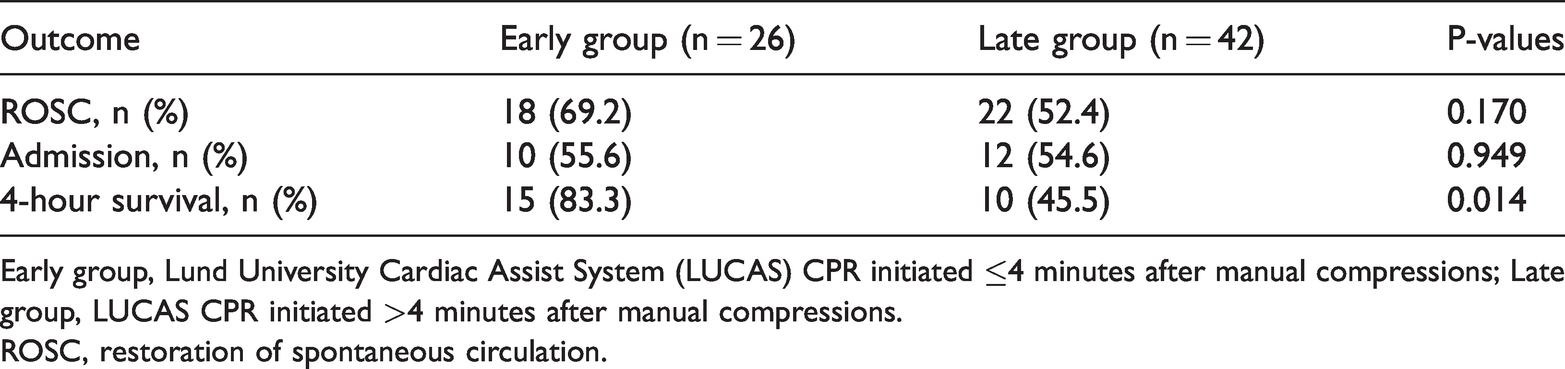
Early group, Lund University Cardiac Assist System (LUCAS) CPR initiated ≤4 minutes after manual compressions; Late group, LUCAS CPR initiated >4 minutes after manual compressions.
ROSC, restoration of spontaneous circulation.
Clinical laboratory test results 15 minutes after initiating LUCAS use
Compared with the baseline clinical laboratory results on ED arrival, blood pH improved significantly 15 minutes after initiating LUCAS use in the early group (P < 0.05), but not in the late group. The partial pressure of oxygen (PO2), partial pressure of carbon dioxide (PCO2), and PetCO2 also improved significantly 15 minutes after initiating LUCAS use in both groups (P < 0.05). However, the lactate concentration did not change significantly between the two groups 15 minutes after initiating LUCAS use (Table 4).
Improvements in clinical laboratory data from baseline to 15 minutes after initiating LUCAS use.

Early group, Lund University Cardiac Assist System (LUCAS) CPR initiated ≤4 minutes after manual compressions; Late group, LUCAS CPR initiated >4 minutes after manual compressions; pH, blood pH.
PO2, partial pressure of oxygen; PCO2, partial pressure of carbon dioxide; PetCO2, pressure of end-tidal carbon dioxide.
Discussion
In our study, the percentages of patients with CA who achieved ROSC in the late and early groups were 52.4% and 69.2%, respectively; which is higher than that reported in a previous study of mechanical compression (36.9%) and hands-only compression (30.5%) among 517 patients admitted to 14 teaching hospital EDs in seven Chinese provinces from July 2015 to July 2017. 21 Our results showed that mechanical compressions could improve ROSC in the ED. We also analyzed the efficacy of LUCAS use initiated at different time points. There were no significant differences in ROSC between the two groups. However, we observed a trend in improved success of ROSC and admission rates in the early group. Furthermore, longer pre-hospital resuscitation duration was associated with later LUCAS use and longer total CPR duration. There were no surviving and discharged patients in our study; therefore, we chose the 4-hour survival rate as the main outcome index in accordance with the LUCAS in Cardiac Arrest (LINC) study, which was a large randomized controlled study of 2589 patients with OHCA designed to evaluate the efficacy and safety of LUCAS combined with mechanical CPR and defibrillation. 14 The 4-hour survival rate was significantly higher in the early group (P < 0.05). This finding highlights the possibility that early implementation of LUCAS could result in better short-term survival rates. The time spent installing the LUCAS device was almost 20 s in both groups, which was similar to the 21-s interval described in a previous study. 27 Shorter compression interruption times improve the effectiveness of CPR. 5
In our study, shockable rhythm was observed as an initial ECG rhythm in less than 3% of patients, which is much lower than in conventional CA cohorts. Compared with developed countries in Europe, and in the USA, and Japan, treatment resources for critical patients in China are limited, medical resources are relatively insufficient, the community emergency system is underdeveloped, and a large number of emergency resources are used to treat non-critical patients. Additionally, CPR directed by dispatchers has not been popularized.28–31 The rate of defibrillation is much lower than that in developed countries, such as the USA and UK, especially when CA occurs outside the hospital. A 2016 multicenter cohort study of 310 patients with OHCA showed that 92.9% of patients with CA were witnessed, but only a small fraction (2.3%) received bystander CPR, and only 1% received defibrillation at the first evaluation. 32
A meta-analysis in 2019 demonstrated no meaningful difference between the mechanical CPR group and the manual CPR group for ROSC, survival to admission, survival to discharge, and survival to 30 days. 11 Previous randomized controlled trials (RCT) also failed to demonstrate improved clinical outcomes compared with manual CPR when mechanical CPR devices were used in a pre-hospital setting, including the Prehospital Randomized Assessment of a Mechanical Compression Device in Cardiac Arrest (PARAMEDIC) trial, 13 Circulation Improving Resuscitation Care (CIRC) trial 12 , and the LINC study. 14 The ROSC and admission rates were similar between the two groups in our study; however, the 4-hour survival rate was better in the early group. These differences between pre-hospital and ED settings might be related to the following factors: 1) More medical personnel in the ED allowed the LUCAS device to be placed quickly, and the compression interruption time while installing the LUCAS device was shorter. Delayed use of LUCAS was because most of the patients were transported to the ED after pre-hospital manual compressions or from other hospital departments. Transfer to the ED was time-consuming and resulted in delays in LUCAS device initiation in the late group. 2) It is difficult for emergency healthcare providers to maintain high-quality compressions in the ED with longer manual chest compression times. After 4 minutes, chest compressions achieved only 30% of the standard press requirements. 33 3) Early placement of the LUCAS device allows ED healthcare providers to devote more energy to advanced life support, such as endotracheal intubation and hypothermia therapy, especially when there is a staffing shortage.
Previous articles reported that higher blood pH, lower lactate concentration, and higher PetCO2 were associated with favorable clinical outcomes in CA. 24 ,34–38 PetCO2 concentrations >1.9 kPa after 20 minutes of compressions might be used to accurately predict ROSC. 36 Some studies reported that high lactate or low pH were associated with a poor prognosis in patients resuscitated from OHCA; blood pH >7.05 was an independent predictor of favorable outcomes after OHCA. 35 Future research must determine whether early application of mechanical CPR can also improve these measurements and result in favorable outcomes.
Our study showed that the blood gas analysis (pH, PO2, and PCO2) results improved after 15 minutes of mechanical CPR in the early group. However, with delayed LUCAS CPR, blood pH did not increase, which is a consistent with ROSC and 4-hour survival rates.
CA causes tissue oxygen deficiency, lactate accumulation, and metabolic acidosis, which can lead to low blood pH. Elevated lactate reflects ischemia-reperfusion injury combined with tissue hypoperfusion. Lactate has also been proposed as a target for resuscitation. 36 Serum lactate concentrations were elevated even when CPR was performed with sufficient blood flow recovery to ameliorate systemic hypoxia and hypoperfusion, with more than 6.0 mmol/L being reported in some studies.37–39 In our study, we also demonstrated that serum lactate concentrations were >10 mmol/L both before and after mechanical CPR, and serum lactate concentrations did not improve after 15 minutes of mechanical CPR. A multicenter study suggested that mechanical CPR enabled improved hemodynamics. 37 The persistently high lactate concentration in the patients in our study might be related to the lack of adequate time for lactate clearance.
Acidosis, peripheral vasodilation, decreased cardiac preload, and the inability to effectively perform CPR generally increase PCO2. In our study, after initiating LUCAS use, PCO2 decreased significantly compared with the baseline data, indicating that mechanical CPR could increase blood flow and accelerate carbon dioxide clearance. Our study showed that PO2 improved after initiating LUCAS use, indirectly indicating that mechanical CPR could effectively augment cardiac output.
PetCO2 monitoring is a useful tool for predicting ROSC in a patient with CA. 37 Some research has shown that PetCO2 values <1.5 kPa after 20 minutes of CPR or <1.8 kPa after 15 minutes of CPR are incompatible with ROSC. 36 In our study, we found the PetCO2 values improved after 15 minutes of CPR in each group. The values were higher in our study than in studies of manual CPR (2.36 kPa), 21 indicating that mechanical chest compressions achieved ROSC better than manual chest compressions.Thus, when the LUCAS mechanical CPR device was used in patients with CA, PetCO2 values improved after 15 minutes of mechanical CPR compared with values immediately after resuscitation (0 minutes); therefore, earlier use of mechanical CPR is ideal.
Limitations
This study was conducted at a single medical center, and the sample size was relatively small. The data were collected from within a relatively short timeframe (May 2018 to December 2019); therefore, the results require further validation through an extended study period. Further prospective studies and/or larger, multicenter studies are needed to corroborate our findings. Whether our results apply universally to other hospital areas, such as general wards, intensive care units, and operating rooms, has yet to be determined. In addition, this study was not a randomized controlled trial but a retrospective observational study with all of the limitations inherent in this study design. Selection biases pertaining to the decision to use mechanical CPR by the treating physician could not be accounted for in this study.
Conclusion
For patients who received mechanical CPR with the LUCAS device in the ED, there was a significant difference in the 4-hour survival rate, and an improved trend in the ROSC and admission rates between patients who received LUCAS CPR ≤4 minutes after manual compressions and patients who received LUCAS CPR >4 minutes after manual compressions. In addition, PO2, PCO2, and PetCO2 improved after 15 minutes of mechanical CPR. In conclusion, early mechanical CPR can improve outcomes in patients with non-traumatic CA in the ED.
Footnotes
Acknowledgment
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Sichuan Health and Family Planning Commission Funding (grant number: 18PJ323) and the Third People’s Hospital of Chengdu.
Author contributions
Tao Xiang, Li Luo, XiaoDong Zhang, and Hang Dai conceived this study. Li Luo and XiaoDong Zhang wrote the initial draft, and Tao Xiang contributed to substantive revision. JiMei Zhang, GuangYing Zhuo, YuFang Sun, XiaoJun Deng, Wei Zhang, and Ming Du contributed to data collection; and all authors participated in this study. Tao Xiang and XiaoDong Zhang take responsibility for this study as a whole.