
Abstract
Introduction
Achieving the optimal survival rate for sudden cardiac arrest in mountains is challenging. The odds of surviving are influenced mainly by distance, response time, and organization of the emergency medical system. The aim of this study was to analyze the epidemiology and outcomes of patients with out-of-hospital cardiac arrest in whom cardiopulmonary resuscitation was performed in the Polish Tatra Mountains.
Methods
This was a retrospective analysis of data on sudden cardiac arrest collected from the database of the Tatra Mountain Rescue Service and local emergency medical system from 2001 to 2021.
Results
A total of 74 cases of sudden cardiac arrest were recorded. The mortality rate was 88% (65/74). Return of spontaneous circulation was achieved in 22 (30%) patients. A group of survivors was characterized by more frequent use of an automated external defibrillator (AED) (56% vs 14%, P=0.011), a shorter interval between cardiac arrest and emergency team arrival (12 vs 20 min, P=0.005), and a shorter time to initiation of advanced life support (ALS) (12 vs 22 min, P=0.004). All survivors had a shockable initial rhythm. The majority of survivors (8/9, 89%) had a good or moderate neurological outcome.
Conclusions
This study confirms poor survival rate after sudden cardiac arrest in the mountain area. The use of AED, shockable initial rhythm, and shorter time interval to emergency team arrival and ALS initiation are associated with better outcomes.
Introduction
Mountains are typically inhospitable areas. Cold, hypoxic environments and rapidly changing weather conditions are associated with a high risk of emergencies. Cardiovascular events are important causes of morbidity during mountaineering activities; however, their frequency is lower than that for traumatic emergencies. 1 -5 The most serious cardiovascular emergency, that is, sudden cardiac arrest, is defined as an unexpected, nontraumatic death within 1 h of the onset of symptoms and is more common in patients with pre-existing cardiovascular diseases. 6
Achieving the optimal survival rate for out-of-hospital sudden cardiac arrest (OHCA) in the mountains is challenging.2,3,5,6 Survival is influenced mainly by response time and distance. Patients having events at greater distance from dispatch points have significantly lower discharge-from-hospital-alive rates.7,8 The odds of surviving OHCA in an urban setting may be >3 times higher than those of surviving in a rural setting. 7 Further, in a well-organized emergency medical system (EMS), patients with OHCA on ski slopes had a better chance of survival than the general population. 5 Each local community should develop its own strategy to make optimal use of forces and resources and to provide effective assistance to victims. Tourism and its seasonal fluctuations place a heavy burden on the local EMS. In some mountainous regions, rescue operations and medical emergency interventions can be performed rapidly and effectively provided weather conditions will permit.2,4,5 However, few data exist on the likelihood of surviving OHCA in the mountains.
The aim of this study was to assess the incidence and outcomes of OHCA in the Polish Tatra Mountains, focusing on identifying potential strategies for improving outcomes.
Methods
Study Design and Data Collection
We carried out a descriptive observational analysis of nontraumatic OHCA in the Polish Tatra Mountains between January 1, 2001 and December 31, 2021. The study was approved by the Jagiellonian University ethical board (number 1072.6120.266.2021) and complied with the Declaration of Helsinki and its amendments.
Data on sudden cardiac arrests attended by paramedics or physicians were collected from the registry of Tatra Mountain Rescue Service and a local community hospital providing definitive care and included location and timing, presence of a witness, course of life support procedures, use of medical equipment, achievement of return of spontaneous circulation (ROSC), postresuscitation care, survival status, and neurological outcome at discharge assessed using Cerebral Performance Categories (CPC). 9 Sudden cardiac arrest was defined as the absence of spontaneous respiration and a palpable pulse. ROSC was defined as electrical activity on the electrocardiogram with a palpable pulse for at least 5 min. Treatment in the field and in the hospital was performed according to the European Resuscitation Council guidelines for basic and advanced cardiac life support and postresuscitation care.
Study Participants
We included all patients of any age with nontraumatic OHCA on hiking trials and adjacent ski areas. Exclusion criteria were no cardiopulmonary resuscitation (CPR) performed, trauma, avalanche burial, lightning strike, suicide, or murder.
Study Setting
The Tatra Mountains are situated along Poland’s southern border. The Polish part of the Tatra Mountains is integrated as Tatra National Park (TNP), with an area of 21,164 km2 and 270 km of hiking trails. There are 8 mountain huts located in TNP, and each of them is equipped with an automated external defibrillator (AED). The region studied is located at an altitude between 1000 and 2500 m. TNP is a popular destination for tourists from Poland and surrounding countries, creating good conditions for hiking, climbing, alpine skiing, ski mountaineering, and snowboarding. The number of visitors to TNP is rising every year, with 2.9 million visitors in 2012 and 4.6 million in 2021. It is estimated that in the summer, particularly popular places are visited by >10,000 people per day. Additional tourist information is available at
The local EMS consists of 2 paramedic-staffed ambulances and 1 physician-staffed ambulance. An additional paramedic-staffed ambulance is available seasonally from January until the end of March and from July until the end of September. One centralized dispatch center is accessed via a uniform 3-digit number. One paramedic-staffed mountain rescue helicopter can reach all parts of the region within a 10-min flight. The helicopter operates only during the daytime, and the area is, however, at least partially within the range of helicopter emergency medical service stationing within 100 km and possessing a night flight capacity. For remote areas, mountain rescuers providing basic life support (BLS) measures equipped with AEDs are dispatched to provide first aid until the first regular team arrives. Most of the valleys are at least partially accessible by dirt roads. Definitive care is provided in 1 centralized community hospital with an interventional cardiology unit, capable of offering standardized postresuscitation care.
Statistical Analysis
Categorical variables are presented as numbers (percentages). Continuous variables are presented as medians (interquartile range) unless otherwise specified. Comparisons of categorical variables were performed using the χ2 test with Fischer correction whenever necessary. Comparisons of continuous variables were performed using the Mann-Whitney U test. A 2-sided P value <0.05 was considered statistically significant. Statistical analysis was conducted using R, CRAN version 4.1.0.
Results
We enrolled 74 consecutive patients with OHCA who received CPR. The study sample comprised predominantly men (95%), and the median age was 58 y (IQR: 52, 63). The majority of OHCAs occurred on the hiking trails (57/74, 77%) at a median altitude of 1219 m (IQR: 1100, 1568) above sea level. The distribution of OHCAs across study years, months, hours, and altitude is presented in Figure 1. BLS was performed in 70 (95%) cases. A witness was present at 66 (89%) events, and a bystander BLS was initiated immediately in 37 (53%) cases. AED was used during BLS procedures in 14 (19%) cases.
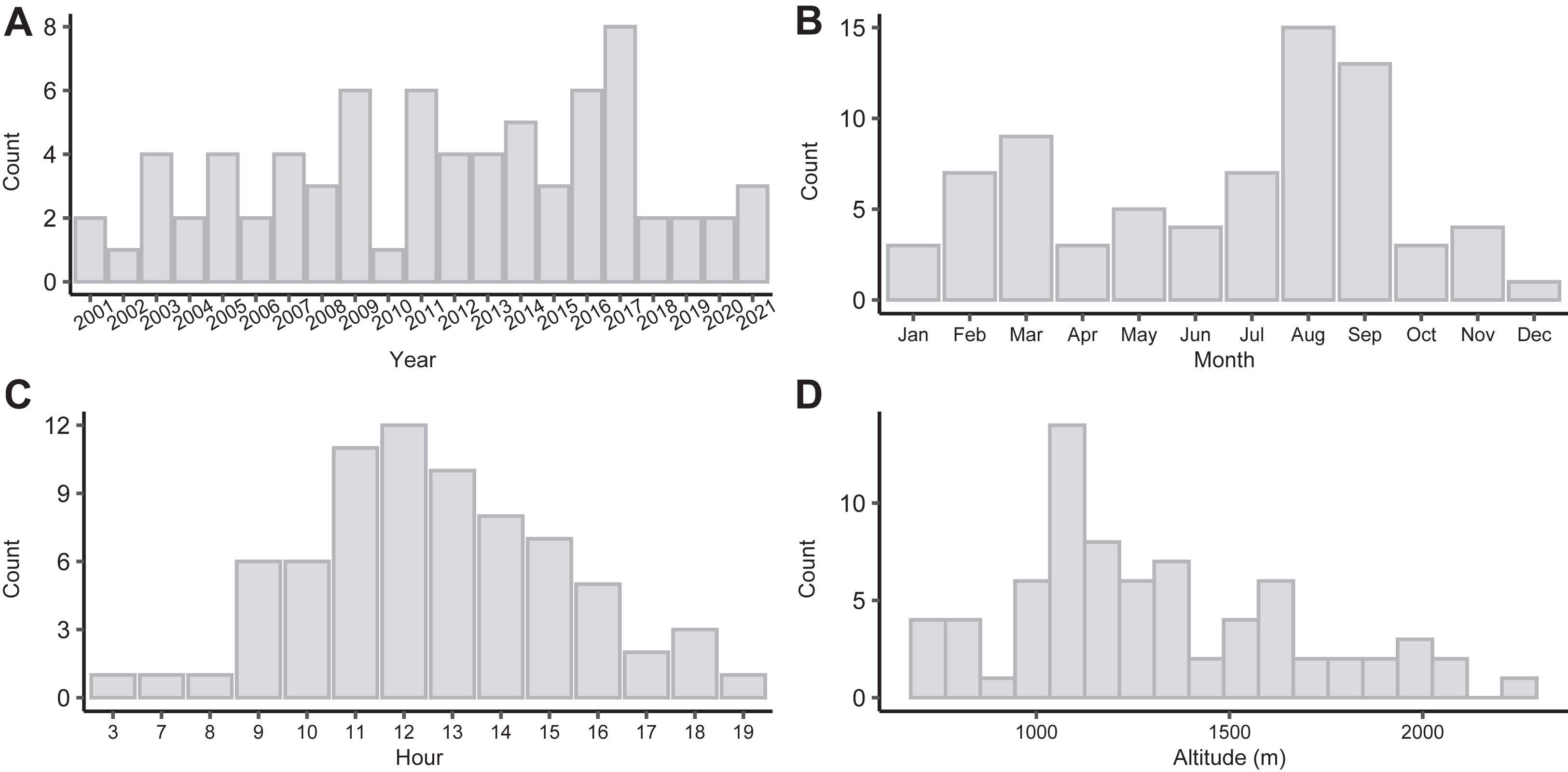
Distribution of out-of-hospital sudden cardiac arrest across years, months, hours, and altitudes.
The most frequently used means of emergency team arrival were helicopter (55/74; 74%) and ambulance (4/74; 5%). The medical team included a medical doctor in 36 (49%) cases. Advanced life support measures were performed in 71 (99%) patients. The initial rhythm was shockable in 45 (61%) cases. Defibrillation and tracheal intubation were performed in 49 of 74 (66%) and 57 of 74 (77%) patients, respectively. Intravenous access was secured in 67 (91%) cases, whereas an automatic chest compression device was used in 30 (41%) patients.
The study group characteristics are summarized in Table 1. Distribution of cardiac arrests by year, month, hour, and altitude is presented in Figure 1.
Study group characteristics
MASL, meters above sea level; BLS, basic life support; AED, automated external defibrillator; ALS, advanced life support.
Categorical variables are presented as number (%). Continuous variables are presented as median (interquartile range).
The mortality in the study group was 88% (65/74). The majority of nonsurvivors died within 24 h of cardiac arrest (60/65; 92%). Assessment of neurological outcomes at discharge revealed a good cerebral performance category (CPC) in 1 in 6 (67%) survivors, moderate cerebral disability (CPC 2) in 2 (22%) survivors, and severe cerebral disability (CPC 3) in 1 (11%) survivor. Detailed characteristics of all survivors are presented in Table 2.
Characteristics of out-of-hospital cardiac arrest survivors
MASL, meters above sea level; CA, cardiac arrest; BLS, basic life support; RT, rescue team; ROSC, restoration of spontaneous circulation; AED, automated external defibrillator; ACD, automatic compression device; PCI, percutaneous coronary intervention; TH, therapeutic hypothermia; CPC, Cerebral Performance Category; VF, ventricular fibrillation.
When only AED was used, initial rhythm was described as “shockable” or “nonshockable.”
Defibrillation by bystanders and ROSC on rescue team arrival.
Factors Associated with Mortality: Univariable Analysis
A univariable analysis revealed that the survivors’ group was characterized by more common immediate initiation of BLS (89% vs 48%, P=0.028), more frequent use of AED during BLS (56% vs 14%, P=0.011), lower rate of physician participation in the emergency team (11% vs 54%, P=0.029), and shorter time to emergency team arrival (12 vs 20 min, P=0.005) and to ALS initiation (12 vs 22.0 min, P=0.004). All survivors had shockable initial rhythm, compared with 55% (36/65) of the nonsurvivors. Intervals from cardiac arrest to the first defibrillation (14 vs 30, P=0.018) and intubation (14 vs 30, P=0.018) were shorter among survivors than among nonsurvivors. Characteristics of patients stratified by survival status and ROSC status are presented in Table 3.
Characteristics stratified by survival status and return of spontaneous circulation status
MASL, meters above sea level; BLS, basic life support; AED, automated external defibrillator; ALS, advanced life support.
Categorical variables are presented as number (%). Continuous variables are presented as median (interquartile range).
A ROSC was achieved in 22 (30%) patients, 13 (59%) of whom eventually died. Nonsurvivors in whom ROSC was achieved were characterized by a longer time from cardiac arrest to ROSC (35 vs 14, P=0.001) and to the first defibrillation (21 vs 8, P=0.010) than survivors. Moreover, AED was used during BLS in 56% of survivors and in none of the nonsurvivors with preceding ROSC. All ROSCs were achieved in the field—there were no reported ROSCs during transport or in the hospital.
Discussion
Our study shows a high mortality rate in patients with nontraumatic OHCA who received CPR in the Polish Tatra Mountains. Factors potentially related to survival included use of AED during BLS, shorter time to emergency team arrival, and earlier initiation of ALS.
It is estimated that 16 people die each year in the analyzed area, the majority of whom are victims of fatal falls. Nevertheless, approximately 20% of deaths are a consequence of primary cardiac arrest. The incidence of OHCA in the Tatra Mountains and adjacent ski areas was 4 per year, and in the Austrian Alps, 78 per year. This is not surprising given the fact that the Tatra mountains have a 70-fold smaller area than the Austrian Alps, and the number of people visiting Tirol every year is >10-fold that in the Polish Tatras. 3 Our study shows that victims of OHCA are mainly middle-aged men. The findings are consistent with those of a prior study in which the risk for sudden cardiac death in hikers was significantly higher for men aged >34 y. Risk during mountain hiking was increased by a factor of 4, and the risk during downhill skiing was increased by a factor of 2. 6
Our study showed that the survival rate from OHCA to hospital discharge accounted for 12%, mostly with a favorable neurologic status. Importantly, the survival rate was also low among patients in whom ROSC was achieved and only slightly exceeded 40%. Internationally, OHCA survival rates vary widely from 0.6% to 25%.10,11 In Europe, approximately 8% of all patients in whom CPR was initiated survived to hospital discharge. 11 Moreover, disparities exist in the effects of CPR between rural and urban areas due to their different characteristics, distances, population densities, and resources. 7 In the Austrian Alps, CPR was attempted in 17% of OHCAs, and only 3% of patients survived to hospital discharge. 3 In another study conducted in the French Alps, bystander CPR was started on-slope in 43%, and 30-d survival was 21%. 5 Despite difficult access and management conditions, patients undergoing OHCA on ski slopes recorded a surprisingly high survival rate. A possible explanation was a healthier and younger population and the efficiency of AED-BLS by ski patrols. Considering the survival rate in OHCA cases in Poland at the level of 8%, the results obtained in difficult mountain terrain are not as poor as might be expected. 11
Studies on OHCA have shown that early initiation of CPR and increased use of AEDs are associated with an improved chance of survival. 11 In our study, the rate of immediate bystander CPR (52%) is close to that reported in European studies in urban areas (58%) and higher than that reported in the Austrian Alps. 3 This discrepancy may result from the rapid growth of tourism and the increasing levels of public awareness and training in BLS of laypersons. Nevertheless, our study adds to the evidence that the higher proportion of witnessed OHCA, the higher probability of bystander CPR and enhanced survival. In our study, AED was used during BLS in approximately 20% of patients, which is comparable to data from the Austrian Alps (17%) but significantly lower than that from the French Alps (44%).3,5 The specific organization of rescue service on French ski slopes with a ski patrol equipped with an AED and wide availability of medical emergency helicopter rescue made for a shorter time to first defibrillation and rapid BLS on the scene. 5 In our study, the AED-BLS was attempted in >55% of survivors, compared with 14% of nonsurvivors. We believe that these data strongly support recommendations made by the International Commission for Mountain Emergency Medicine and European Resuscitation Council on the placement of AEDs at specific sites such as mountain huts and ski resorts.12,13 Nearly all survivors in our study had a good neurological outcome (CPC 1-2) at discharge, which further emphasizes the importance of the universal availability of AEDs and immediate initiation of life support procedures by bystanders in terms of functional capacity and quality of life in OHCA survivors.
Organizations or communities involved in the management of OHCA should evaluate their system performance and target key areas with the goal to improve performance. Interventions that can be implemented by healthcare systems to improve outcomes of OHCA have been recently provided. 14 Although some studies suggested no additional benefit from ALS in an AED-optimized system, a recent study has shown that early ALS was associated with improved survival to hospital discharge, which is in line with our observations.15,16 It is suggested that in mountainous and other less available areas, onsite medical diagnostics and treatment should be provided by integrating mountain rescue services and ALS-staffed ambulances and helicopters. 17 A good quality of treatment during the postresuscitation phase with urgent coronary angiography, optimization of circulation and ventilation, targeted temperature management, advanced neuroprognostication, and rehabilitation may improve outcomes. 14 However, given the results of our study, more emphasis should be placed on reducing the time from cardiac arrest to AED-BLS provision and raising awareness about CPR and defibrillation among hikers and mountaineers.
This study has several strengths, such as the completeness of data including all OHCAs during the study period and the accuracy of data collected retrospectively according to the Utstein scheme. Moreover, OHCA victims were treated by a single, specialized mountain rescue group, which is an integral part of the local system.
Limitations
We are also aware of several limitations of our study. First, the small study sample did not allow us to perform reliable multivariable analysis, thus increasing the risk of omission of important confounding factors. Second, the retrospective character of the study significantly increased the risk of systematic bias and decreased the quality of evidence. Finally, more detailed data on patients’ medical history, for example, comorbidities and medications, would provide us with some interesting and significant observations.
Conclusions
The survival rate of 12% from OHCA in difficult mountain terrain is not as poor as might be expected. Importantly, the majority of the survivors were discharged from the hospital with a favorable neurological status. Factors potentially related to survival include shockable initial rhythm, more frequent use of AED during BLS, a shorter time to emergency team arrival, and a shorter time to ALS initiation. Efforts to further develop public access to a defibrillation program, to accelerate the delivery of the AED to the scene, and to improve the level of public CPR awareness and knowledge are crucial for the further improvement of OHCA outcomes.
Footnotes
Acknowledgments
The authors thank Mr Jan Krzysztof, head of Tatra Mountain Rescue Service, for his consent to use the organization’s database for this research work. They would also like to thank all doctors, paramedics, and other members of Tatra Mountain Rescue Service for their help in collecting the data.
Author Contributions: study conception and design (MM, KP, WSz, AG, SK); analysis and interpretation (MM, KP, WSz, SK); data collection (MM, AG, SK); writing the article (MM, KP, WSz, AG, SK); critical revision of the article (MM, KP, WSz, AG, SK); statistical analysis (MM, KP, WSz, SK); final approval of the article (MM, KP, WSz, AG, SK).
Financial/Material Support: None.
Disclosures: None.