
Abstract
There are numerous emergency department visits in the United States for all types of marine animal injuries each year. These injuries may result in significant morbidity or mortality if not managed appropriately. Accurate identification of the offending species, thorough wound hygiene, and judicious use of antibiotics are important for preventing infections. This review aims to describe management strategies and antimicrobial considerations for nonmammalian marine vertebrate penetrating trauma in North America, the Caribbean, and Hawaii. A literature search was performed to identify studies on this subject. This literature consisted of clinical case reports and case series. Reports extracted included those on sharks, barracuda, eels, catfish, stingrays, lionfish, stonefish, and scorpionfish. The majority of reported trauma occurred to beachgoers, fishermen, or commercial aquarium employees who routinely handle these animals. Injury patterns depended on the species but most commonly affected the lower extremities. Infections were seen from saltwater bacteria, human skin flora, or marine animal oral flora. After thorough wound irrigation and exploration, most authors recommended prophylactic antimicrobials to cover Vibrio species, in addition to other gram-negative and gram-positive species. The literature is notable for the lack of controlled studies. Some authors recommended radiographic and/or ultrasonographic imaging to identify retained foreign bodies, such as spines, sand, or teeth.
Introduction
In the United States, there are an estimated 4200 emergency department visits for all kinds of marine animal injuries each year. 1 Injuries described in the literature include bites, abrasions, contusions, puncture wounds, and envenomations. These may be complicated by life-threatening infections from saltwater bacteria or the marine animal’s oral or skin flora. Although most wounds heal without complication, local infection, necrotizing fasciitis, septicemia, permanent neurological deficits, and vascular injuries have been described. 2 -7 This review describes the management of marine nonmammalian vertebrate penetrating traumatic injuries in North America, the Caribbean, and Hawaii.
Literature Search Methodology
The PubMed search engine was utilized to identify the species of interest: sharks, stingrays, eels, stonefish, scorpionfish, lionfish, catfish, and barracuda. We systematically identified relevant publications using the Boolean search strategy: (shark attack OR shark bite OR shark wound OR shark trauma OR shark injury) AND (antibiotics OR microbiology OR treatment OR management). This search strategy was repeated by replacing “shark” with each different species. The study period included the time from PubMed database inception until April 2021. The literature search yielded few controlled studies. We included case reports, retrospective and prospective case series, and review articles pertaining to marine vertebrate penetrating trauma in North America, the Caribbean, or Hawaii (Figure 1). The University of California, Irvine, determined this study to be nonhuman subject research and, therefore, exempt from review.
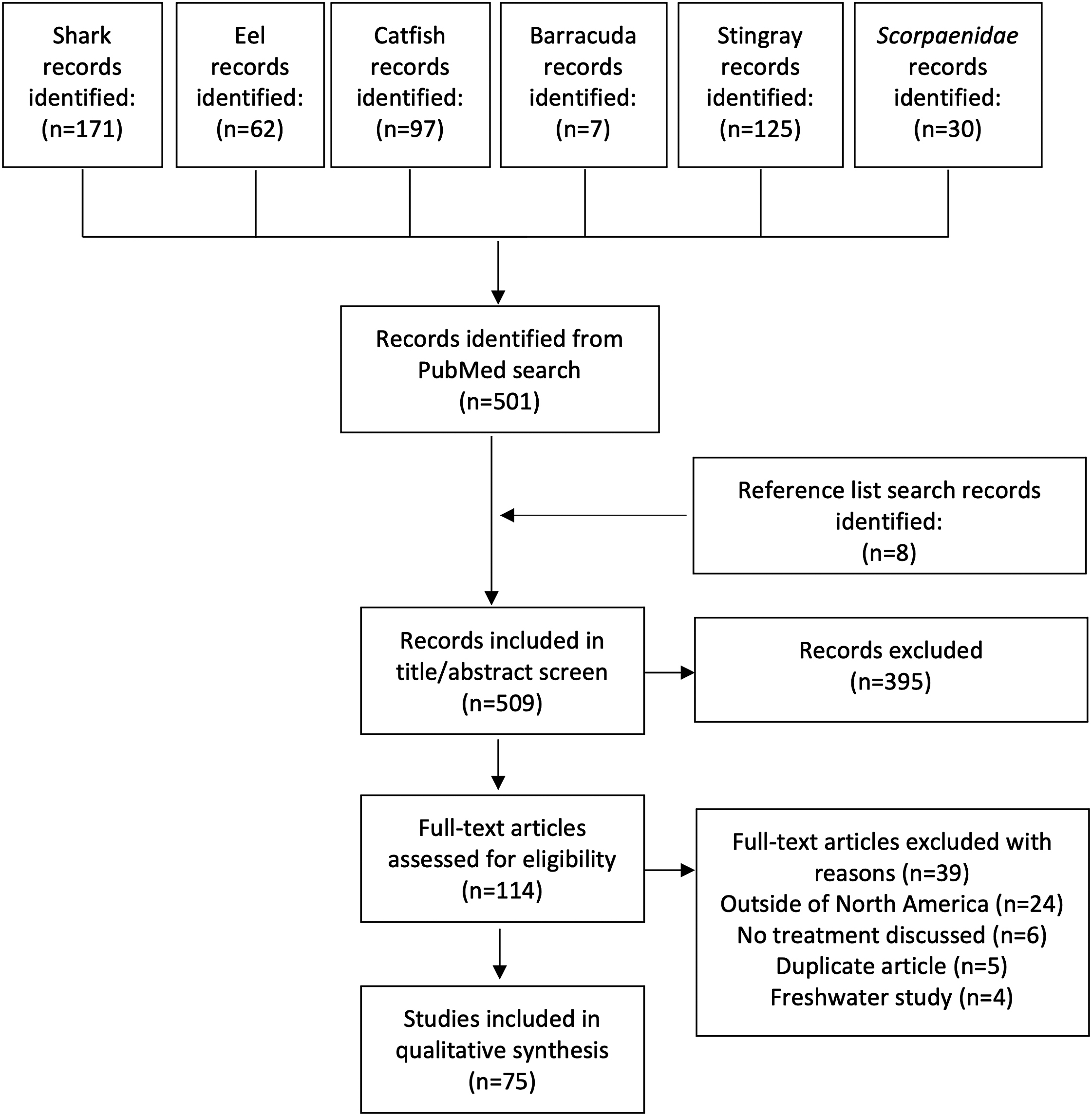
Flow diagram demonstrating article screening and selection process.
Results
The initial PubMed query yielded articles meeting our criteria pertaining to sharks, eels, catfish, barracuda, stingrays, and Scorpaenidae. Articles were excluded for geographical irrelevance, lack of discussion about treatment, duplications, or discussion only pertaining to freshwater trauma (Figure 1). After the reference lists were searched, 8 additional articles were included. Subsequently, 2 authors determined the eligibility of each article, and 43 articles were selected for inclusion, of which 37 were case reports or case series. An overall summary of the data is provided in the online Supplemental Table.
Sharks
The literature search revealed 8 articles pertaining to shark-related injuries in North America and the Caribbean. 6 -13 These included 5 case reports6,7,9,10,12 and 3 retrospective case series.8,11,13 Treatments in all cases included wound irrigation, exploration, and debridement. Surgical repair of the wound occurred in 4 case reports. One retrospective case series of 96 patients sustaining shark-related injuries reported a mortality rate of 8%, significantly higher in patients with vascular injury (20% vs 4%). 11 The authors reported operative interventions on 55% of patients. Factors associated with need for operative repair included musculotendinous or vascular injury. 11 Another retrospective series evaluated 61 patients in Hawaii 13 and included 4 (7%) fatalities and 10 (16%) patients who required operative intervention.
Antibiotics were administered in all case reports describing shark-related injuries. Antibiotics given were topically in 1 case (mupirocin ointment), 10 orally in 1 case (cephalexin and ciprofloxacin), 7 and intravenously in the remaining 3 cases (ceftriaxone, 12 cefazolin, metronidazole, clindamycin, 9 first-generation cephalosporin 6 ). Empiric antibiotic regimens were changed after wound culture in 2 cases; monotherapy with ceftriaxone was converted to a dual-drug regimen of vancomycin and ticarcillin after wound cultures grew Acinetobacter, Bacillus, Staphylococcus epidermidis, and Bacteroides in 1 case, 12 and a multidrug regimen of cefazolin, metronidazole, and clindamycin was converted to vancomycin, ceftazidime, caspofungin, and metronidazole after wound cultures grew Candida glabrata, Bacillus pumilus, and Bacillus megaterium. The initial antibiotic regimen was successful in 1 case in which an IV first-generation cephalosporin (cefradine) was used to treat Vibrio carchariae infection. 6 In 2 cases, antibiotics were prescribed prophylactically, and neither patient developed an infection: in 1 case, the patient received oral cephalexin and ciprofloxacin, 7 and in the other, topical mupirocin ointment. 10 In 1 retrospective case series, 6 of 11 patients were treated with antibiotics, including monotherapy with ciprofloxacin (3 patients), doxycycline (2 patients), or clindamycin (1 patient). 8 Cultures from the infected wound grew Morganella morganii and Enterococcus faecalis. The third retrospective case series evaluated 61 patients who sustained shark-related injuries in Hawaii. 13 Twelve patients received antibiotic prophylaxis with multidrug regimens that included doxycycline, and the authors reported only 1 infection caused by Pseudomonas aeruginosa. This patient was started on cefepime and underwent subsequent wound debridement with resolution.
Barracuda
Barracuda have been described in subtropical waters of Florida, the Caribbean, and Hawaii. 14 Our literature search revealed 4 review articles 14 -17 that addressed barracuda-related injuries and 2 textbooks that described individual cases18,19 but no primary case reports or case series. One of these texts described 5 cases of barracuda-related injuries. 18 In 3 cases, significant lacerations required surgical repair, while in the remaining 2, the injuries were minimal. The author described 2 women bit by barracuda while swimming with shiny barrettes, 1 of which required surgical extraction of embedded teeth. The author hypothesized that the barracuda mistook the barrette for a silvery fish. The other text described a total of 29 barracuda attacks. 19 Of the 16 cases that occurred in our designated study location, detail was provided regarding treatment and outcome in 11 cases. These reports were derived from journal articles (n=3),20,21 other textbooks (n=3),22,23 newspaper articles (n=3), and personal communications with a colleague (n=2). The author reported 3 fatalities, suture repair in 5, surgical intervention in 2 (operative debridement in 1 and amputation in the other), and hypovolemic shock requiring fluid resuscitation and hospitalization in 1.
There were no studies describing the specific microbiology of barracuda oral flora or bite wound infections, and there are limited reports on antibiotic use. Several reviews recommended similar antimicrobial coverage as in shark bites. 14 -16
Eels
Several species of moray eels are found on both coasts of North America and in the Caribbean and Hawaii. This literature review revealed 1 case report and 1 small case series of 3 patients for a total of 4 cases.24,25 Three cases involved lacerations to the hand for which direct pressure was sufficient to stop bleeding. 24 The remaining case involved an avulsion wound to the forearm, and bleeding was controlled with a cloth tourniquet until the patient reached a medical facility. 25 Two injuries occurred with eels in captivity, 24 and 2 occurred in scuba divers.24,25 All cases underwent wound exploration, and radiographic imaging was obtained in 2 cases.
In the case series, all patients received tetanus vaccination and antibiotic prophylaxis with either cefuroxime (n=1) or ciprofloxacin (n=2); no wound infections were reported. 24 The authors did not culture the wounds but did culture mouths of 2 captive moray eels and found the following species: Vibrio, Micrococcus, coagulase-negative Staphylococcus, and Pseudomonas putrefaciens. The authors reported that all Vibrios species and P puterfaciens were sensitive to cefuroxime, ciprofloxacin, trimethoprim-sulfamethoxazole, and tetracycline.
There was 1 notable case in which an unprovoked moray eel bit a diver’s arm, resulting in significant tissue loss and neurovascular damage requiring operative exploration. 25 The postoperative course was complicated by a wound infection after 1 week despite treatment with an unspecified antibiotic, which resolved with wound re-exploration, skin grafting, a course of IV monotherapy with ciprofloxacin, and hyperbaric oxygen therapy. Despite hand physical therapy, the patient had significant ulnar nerve palsy at the 9-mo follow-up.
Catfish
There were 4 reports on saltwater catfish, which included 2 retrospective case series26,27 and 2 case reports.28,29 One retrospective case series on 83 total catfish-related injuries in Mississippi reported that 39 injuries were inflicted by saltwater species. 27 Of these cases, 16 required catfish spine extraction, and radiographs were taken in 4. A catfish spine was found near the radial artery in 1 patient, prompting further imaging with computed tomographic angiography; the outcome was ultimately an uncomplicated operative removal of the spine. One patient presented with digital dry gangrene and required amputations of the third and fifth digit. 27 One patient was treated with hot water immersion (HWI) and had significant improvement in his localized pain. 27
In addition, in 3 cases, IV antibiotics were administered. 27 The authors reported that 26 patients presented with clinical evidence of infection (eg, redness, swelling) and 2 patients had positive cultures growing Micrococcus, Staphylococcus epidermidis, and Streptococcus, but the authors did not specify whether these cases were in freshwater or saltwater. They further reported that only 1 patient did not respond to their initial antibiotics (oral cephalosporin), and the infection resolved after switching to oral ciprofloxacin.
Empiric antibiotic regimens described included multidrug regimens consisting of IV clindamycin/gentamicin (n=1), 27 cefotaxime/aztreonam (n=1), 27 piperacillin-tazobactam, vancomycin, doxycycline, and clindamycin (n=1), 29 or monotherapy with ceftriaxone (n=1). 28 Prior to receiving the last regimen, the patient developed fever and leukocytosis shortly after presentation to the emergency department and was found to have necrotizing fasciitis requiring several operative debridements. 29 However, the patient’s wound cultures were negative and the infection ultimately resolved with 9 d of the multidrug regimen consisting of piperacillin-tazobactam, vancomycin, doxycycline, and clindamycin followed by 6 d of outpatient IV piperacillin-tazobactam and doxycycline.
Stingrays
Fifteen articles described stingray-related injuries, including 6 retrospective case series4,30-34 and 1 prospective case series 35 on a total of 814 patients. There were an additional 8 case reports for a total of 822 patients.2,5,36-42
The 2 case series published in 1953 and 1957 described historic regimens, including codeine, meperidine, penicillin, and phenobarbital,30,31 as well as cryotherapy. 31 Since then, HWI has emerged as a means of reducing pain by mitigating the effects of the stingray toxin. HWI was used to treat local pain in 1 prospective case series, 35 4 retrospective case series,4,32-34 and 1 case report 2 for a total of 422 patients. One case series showed complete resolution of pain and no wound complications in the HWI group compared with persistent pain and wound complications (including local necrosis, abscess formation, and chronic draining sinus tract) in the group receiving no heat treatment. 32 These findings were redemonstrated in 2 subsequent case series; 1 found that 69% of patients reported adequate pain relief with HWI and no pain medications 33 and another found 88% of patients reported complete resolution of pain with HWI alone. 34 The prospective case series treated 22 patients with HWI and reported statistically significant reductions in average pain score. 35 The case report described improvement in local pain after HWI, but the patient was not given antibiotics and presented 4 d later with necrotizing fasciitis. 2
Data on radiographic imaging have been reported in 2 retrospective case series33,34 and 6 case reports.2,37-40,42 One series obtained x-ray imaging in 68 of 120 patients (57%) and found 1 retained stingray spine (2%). 33 The other series reported either wound exploration or radiographs in 272 of 485 cases but did not specify the proportion of patients who received radiographs. 34 The authors reported that a foreign body was detected in 45 of 485 cases (9%). 34 Of the case reports, 3 obtained initial plain x-rays, which found foreign bodies in 2 cases.2,39,40 In 1 case, the patient sustained a stingray injury to the ulnar aspect of the wrist but did not have radiographs taken. 38 Over the next month, the patient developed a right middle finger extension deficit and a subsequent radiograph demonstrated 2 retained spines, which had lacerated the extensor digitorum communis and caused extensive tenosynovitis with copious purulence. He required operative removal of the spines and was treated with doxycycline for 2 wk. In 2 cases, imaging other than x-ray was obtained: (1) an arteriogram demonstrated a superficial femoral artery pseudoaneurysm in a patient who presented with sensory changes, hematoma, and a pulsatile mass to the proximal thigh from a stingray penetrating injury 2 wk prior, 42 and (2) computed tomography of the chest demonstrated a pneumothorax and transcardiac stingray barb in a patient struck by a stingray in the chest. 37
Regarding infection, 1 retrospective case series reported 90 of 119 patients (75%) received antibiotics. 34 The authors divided the patients into 2 groups: Group 1 presented shortly after injury, and 71 of 100 patients received antibiotic prophylaxis, while Group 2 presented more than 24 h after injury, and all 19 patients received antibiotics. In the immediate presentation group, there was 1 infection (2%) in the subset of patients who received antibiotics and 5 infections (17%) in the subset that did not. The 2 patients who sustained infections while on antibiotics were initially treated with levofloxacin, and their infections resolved after switching to either cephalexin or piperacillin-tazobactam. In Group 2, 2 patients who were already on antibiotics (1 on cephalexin and the other on ampicillin-sulbactam) presented with local infections, and both were changed to ciprofloxacin with resolution of infection. Another patient started on levofloxacin in the emergency department presented the following day with worsening symptoms, so IV piperacillin-tazobactam was added without further complications. Another retrospective database study on stingray-related injuries reported administration of tetanus vaccination in 17% of cases, systemic antibiotics in 13%, and topical antibiotics in 1%. 33
Scorpaenidae
A review of literature yielded 8 studies on Scorpaenidae, which consisted of 7 case reports (1 article described 2 cases)17,43-48 and 1 retrospective case series 49 for a total of 59 cases. Outcomes were only present in 38 patients in the case series (3 scorpionfish, 35 lionfish) for a total of 5 scorpionfish43,48,49 and 41 lionfish17,44-47,49 cases. In the case series, HWI was used in all 38 patients for symptom management and resulted in complete pain relief in 24 h in 80% and moderate relief in 14% of patients. 49 There was 1 scald injury (2%) and 1 hypotensive patient requiring IV fluids (2%). There were 4 reported infections (8%), one of which required hospitalization for wound debridement and intravenous antibiotics. No information regarding the identity of antibiotics or culture results was provided.
In the case reports, HWI was used in 5 of 8 cases and provided adequate pain relief, requiring no further pain control in 2 of 5 cases.17,43 In the other 3 cases, further pain control was required, including the use of vesicle debridement, 45 digital nerve block, 46 or opioids. 47 One patient was treated with ice and had no relief, 44 1 patient’s symptoms resolved spontaneously, 48 and the pain control in the final case was not described. 45 There were no infectious complications among case reports, but wound healing was complicated by bullae or vesicle formation in 3 cases.
Discussion
We present a review of the emergency management, microbiology, and antibiotic treatment for marine penetrating trauma in North America, the Caribbean, and Hawaii. While the literature lacks controlled studies on antibiotic usage, this compilation of reported data may assist providers in determining the appropriate initial management, imaging modalities, pertinent microbiology, and antibiotic treatment.
For initial treatment, the literature was largely in agreement regarding thorough wound irrigation, debridement, and exploration to remove all foreign objects and debris. Tetanus prophylaxis was universally recommended. Wound cultures were not reported in a large majority of the articles reviewed, but there were 3 case reports in which initial antibiotic regimens were changed after cultures returned9,39,40 and another one in which culture results guided initial antimicrobial choice. 5 As such, we recommend obtaining wound cultures when managing these injuries. However, more evidence is needed before firm guidelines can be made. The literature was strong in detailing the importance of removal of retained foreign material (eg, stingray spines) as well as HWI (42–45°C for 30–90 min) to neutralize the heat-labile stingray toxin and provide pain control. HWI was frequently employed to improve symptoms in envenomations from catfish, stingrays, lionfish, and scorpionfish and improved symptom burden in 69% to 88% of stingray and 40% of Scorpaenidae injuries.33,34,49 However, in the 5 case studies on Scorpaenidae injuries, 3 patients required further pain control after HWI (ie, opioids, debridement, nerve block), which suggests that more research must be done to verify these results and determine the role of adjunctive treatments.
The use of imaging studies in marine penetrating trauma represents another area without agreement in the literature. Shark teeth and the barbs of catfish, stingray, and Scorpaenidae are radiopaque, though fragments of the integumentary sheath can be radiolucent, and may be better detected by bedside ultrasound.7,50,51 In a retrospective review of 119 stingray injuries at a single institution, the authors reported no retained barbs detected by radiography. 34 However, 1 case report described a patient who sustained a stingray puncture wound to the arm, resulting in a permanent neurologic deficit in the hand. 38 Furthermore, local tissue necrosis was described in 2 studies due to persistent envenomation from a retained barb.17,52 Based on the results of this review, we recommend that, after irrigation and debridement, the clinician obtains radiographic imaging. Bedside ultrasonography or magnetic resonance imaging can detect radiolucent foreign bodies and may be helpful in cases when retained foreign material is suspected but not visualized on radiographs.50,51,53
The literature revealed myriad strategies regarding the use and choice of antibiotic. In the absence of comparative trials, evidence-based recommendations are difficult. One multicenter case series on 11 patients with shark-related injuries did not provide any antibiotics to 5 patients with relatively minor injuries and reported only 1 infection (cultures revealed Morganella morganii and E faecalis). 8 However, others argued that the plethora of bacteria cultured from the marine environment and shark teeth warrant antibiotic prophylaxis in all cases of shark bites. 54 -56 Vibrio and Pseudomonas were the predominant species cultured from moray eel mouths. 24 Gram-positive (including S aureus), gram-negative (including Pseudomonas), and anaerobic bacteria were described in most microbiological studies.2,29,56-59 Thus, for significant traumatic injuries involving marine species, prophylactic oral treatment with broad-spectrum coverage for gram-positives (including S aureus) and gram-negatives (including Pseudomonas) seems reasonable. An appropriate oral antibiotic selection may include 1 or more of the following antibiotics: trimethoprim-sulfamethoxazole, ciprofloxacin, doxycycline, clindamycin, or second- or third-generation cephalosporins. Intravenous regimens should be reserved for treatment of infections rather than prophylaxis, except in cases of severe wounds requiring hospitalization. Potential intravenous regimens for treatment include vancomycin, ciprofloxacin, doxycycline, clindamycin, piperacillin-tazobactam, third- or fourth-generation cephalosporins, or carbapenems. For unresolved infections, clinicians must maintain a high index of suspicion for fungal and atypical mycobacterial infections, such as Mycobacterium marinum. 12
Limitations
The primary limitation of this review is derived from the low level of evidence of our sources. Most of the literature consists of relatively small retrospective case series or case reports with variable follow-up. There were no controlled studies regarding which wounds required antibiotics or which antibiotics were most efficacious. The level of evidence differed by species, with sharks and stingrays having a significantly larger number of reports. Furthermore, our review only included studies written in the English language that were found in the PubMed search engine, which likely omitted reports published in books and conference proceedings. Moreover, there are many cases of marine penetrating trauma that are not published each year, further limiting the generalizability of our data.
Conclusions
Marine penetrating trauma, though rare, can potentially cause serious morbidity or mortality. Results of this literature review suggest that most authors recommend identification of the offending species, thorough irrigation of the wound, utilization of imaging studies to identify retained foreign material when suspected, debridement if necessary, administration of tetanus prophylaxis, and use of prophylactic antibiotics to cover common marine flora and the skin and oral flora of the offending species. The majority of the literature discusses microbiology and antimicrobial management of shark, stingray, catfish, and Scorpaenidae injury, but further studies delineating microbial oral flora of species such as eels and barracuda are needed.
Footnotes
Acknowledgements
Author Contributions: idea inception (IMA); study design (ALB, IMA); data retrieval (KCP, ASH); data analysis (KCP, ASH); manuscript composition (KCP, ASH); manuscript editing (ALB, IMA); manuscript final approval (ALB, IMA, KCP, ASH).
Financial/Material Support: None.
Disclosures: None.
Supplemental Material(s)
Supplementary material associated with this article can be found in the online version at
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.