
Abstract
Envenomation by Scolopendra heros, the Texas redheaded centipede, can present variably. Although transient pain and erythema are often treated conservatively, complications may include cellulitis, necrosis, myocardial infarction, and rhabdomyolysis. We present a case of an elderly man who came to the emergency department with lymphangitis and dermatitis secondary to a centipede sting that awoke him from sleep. It is important to recognize the potential of centipede envenomation to have severe local and systemic manifestations.
Introduction
The Texas redheaded centipede, or giant desert centipede (Scolopendra heros) is the largest centipede found in North America. It is located in the southwestern United States and northern Mexico. Clinical manifestations of centipede stings are thought to occur as a result of cytolytic proteins in the venom. 1 We present a case of an older patient who developed localized lymphangitis and dermatitis after a Texas redheaded centipede sting.
Case presentation
A 79-year-old man arrived to the emergency department by emergency medical services 1.5 hours after a known centipede sting. The patient brought the centipede in a plastic bag, and it was identified as S heros, the Texas redheaded centipede (Figure 1). He reported pain and swelling to his left hand, with redness tracking up his left medial arm (Figures 2 and 3). The patient was noted to have 2 puncture marks to the palmar aspect of his left thumb and intact sensation and motor strength. In the emergency department, ice packs were applied to the involved area. New pen markings were drawn surrounding the lymphangitis, as erythema had already surpassed initial pen markings by emergency medical services. A radiograph of the left hand was negative for acute abnormality. Laboratory analysis revealed a white blood cell count of 7.2/µL, an erythrocyte sedimentation rate of 9 mm/h, a c-reactive protein level of 0.4 mg/L, a procalcitonin level of <0.10 µg/L, and no electrolyte abnormalities. The patient was given intravenous hydromorphone, diphenhydramine, and dexamethasone for symptom control. Given the acute onset of symptoms immediately after the sting, the lymphangitis and dermatitis were likely toxin related. However, to cover possible infectious etiologies, he was given intravenous vancomycin in the emergency department. He was admitted to an inpatient floor and was continued on intravenous clindamycin.
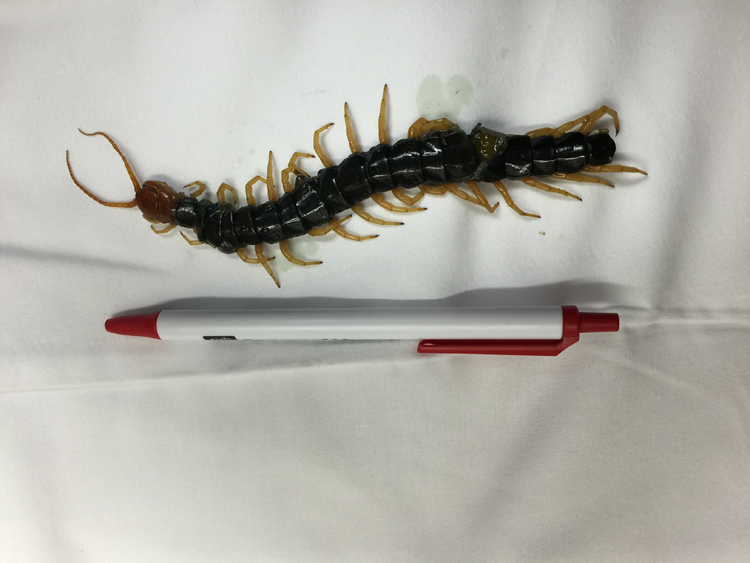
Texas redheaded centipede (Scolopendra heros).

Lymphangitis and dermatitis left forearm after centipede sting.

Lymphangitis, left forearm.
Twenty-four hours after the sting, his white blood cell count was 12.4/µL. He reported edema and mild pain, but the erythema was significantly improved. He was discharged after 2 overnight stays with a prescription for clindamycin and outpatient follow-up. Blood cultures were negative at 5 days. Twelve days after the centipede sting, the patient was seen in clinic. He was found to have a small, well-healing sting without foreign body, swelling, warmth, or erythema.
Discussion
Centipedes are arthropods of the subphylum Myriapoda, class Chilopoda. S heros is one of more than 2600 species of centipede. They are found in warm and tropical climates, favoring a temperature of 24 to 29°C and humidity of 75 to 80%. 2 These fast-moving, multisegmented carnivores span up to 20 cm. They spend most of their time underground and are largely nocturnal.3,4 Most stings occur during the night. They reproduce during the rainy season, during which time they are more likely to come in contact with humans. 5 Two small puncture marks and accompanying blood clots may be visible after a centipede sting. 6 Although commonly referred to as “bites,” centipedes actually inject venom through forcipules, pincer-like, modified legs that extend from the first segment behind their head. 2 Cases of centipede stings have been documented in Israel, Japan, the Philippines, the United States, Brazil, and Australia. 7 The most venomous stings are typically caused by select species of the Scolopendra genus, including Scolopendra subspinipes and S heros. Their cytolytic toxicity is attributable to a mixture of histamine, serotonin, phospholipase A2, and hemolytic and acidic protein in the venom. 13 However, because the venom is also antibacterial, infection is uncommon even when antibiotics are not prescribed. 2
Centipede stings commonly induce pain, erythema, and edema. A retrospective study of 98 cases reported these symptoms at a frequency of 94.9%, 44.9%, and 21.4%, respectively. 8 Of those cases, 89.8% occurred on the fingers and toes. Other systemic symptoms can occur, including pruritus, headache, nausea, vomiting, palpitations, cellulitis, necrosis, Well’s syndrome, myocardial infarction, and rhabdomyolysis.2,3 Delayed reactions as a result of a type III immune response are also common. 2 Symptoms are most often transient, localized, and require only supportive care.
Treatment of uncomplicated centipede stings includes pain reduction with ice pack application, systemic analgesics, and local anesthetics as needed. 2 ,6,7,9,10 Several studies have also suggested antihistamines, corticosteroids, and extremity elevation for the relief of pain, itching, and inflammation. 2 ,6,7,9,11,12 Tetanus prophylaxis is recommended and antibiotics have been suggested to prevent necrosis and secondary infection.6,9,24 Unfortunately, antivenom is economically unviable for any centipede venom and does not currently exist. 7 ,13,14 For complicated centipede stings, treatment should be aimed at addressing the complication. For example, this may include prescription of antibiotics for secondary wound infections and fluid resuscitation for acute kidney injury. 6
Although most stings are not life threatening, there have been at least 3 reported cases worldwide of death induced by centipede venom.3,9 The most frequently documented life-threatening cases are due to myocardial infarction. This has been demonstrated in 3 separate cases involving men aged 20, 22, and 60 years old. 3 ,9,15 The most severe encounter with S heros occurred in a 44-year-old woman bit on the right foot by a 15-cm centipede, which resulted in peroneal neuropraxia, compartment syndrome, and rhabdomyolysis. 1
Our case was complicated by lymphangitis and dermatitis and the patient recovered well. However, the aforementioned cases emphasize that those treating centipede stings should recognize the potential of centipede envenomation to have severe systemic manifestations.
Author Contributions: Study concept and design (SE, AJ), acquisition of the data (SE, MJ), drafting of the manuscript (MJ, SE, AJ), critical revision of the manuscript (SE, AJ), approval of final manuscript (AJ).
Financial/Material Support: None.
Disclosures: None.
Footnotes
☆
Case report poster presented at the 2016 American Academy of Emergency Medicine Annual Scientific Assembly, Las Vegas, NV.
Submitted for publication August 2016.
Accepted for publication November 2016.