
Abstract
Introduction
After a scorpion sting, patients commonly present to hospitals with pain. Our study sought to compare the analgesic efficacy of IV paracetamol, IV dexketoprofen trometamol, topical lidocaine, and placebo in patients reporting pain after presenting with a history of scorpion sting.
Methods
This double-blind, randomized, placebo-controlled study was conducted in the emergency department of a tertiary hospital. Adult patients who presented with the complaint of pain after a scorpion sting and did not have systemic findings were randomly assigned to 1 of the following 4 groups: IV paracetamol, IV dexketoprofen trometamol, topical lidocaine, and placebo. The visual analog scale scores were measured at the time of presentation to the emergency department and at 30 and 60 min to determine the pain intensity.
Results
The study included 106 patients, of whom 30 were in the paracetamol group, 26 in the dexketoprofen trometamol group, 25 in the topical lidocaine group, and 25 in the placebo group. We did not find a different analgesic effect among the groups in the first 30 min (P=0.185). IV paracetamol, dexketoprofen trometamol, and topical lidocaine did not show different analgesic effects in the first 60 min (P>0.05). IV paracetamol and dexketoprofen trometamol were found to provide a more effective analgesia than the placebo at 60 min (P<0.05). The analgesic effects of topical lidocaine and placebo did not differ (P=0.330).
Conclusions
IV paracetamol and IV dexketoprofen trometamol provided analgesia in the first 60 min, similar to topical lidocaine but superior to placebo.
Introduction
Scorpion stings occur globally, especially in Africa, the southwestern United States, Latin America, South Asia, and the Middle East, and they cause significant health problems. Among the approximately 2700 known species, 30 species reportedly are dangerous to humans. 1 -3 Our study was conducted in southeastern Turkey where a higher number of scorpion stings are seen compared to other parts of the country, and the most common species are Androctonus crassicauda, Leiurus quinquestriatus, Mesobuthus gibbosus, and Mesobuthus eupeus species that belong to the Buthidae family. 4 Although scorpion stings are rarely fatal in developed countries, they are still a significant contributor to mortality from envenomation in developing countries. 1 This situation can be explained by the fact that health authorities in developed countries properly organize the management of scorpion stings. 3 According to recent studies, 7 regions in the world where scorpion stings are at high risk have been identified. These are north Saharan Africa, Sahelian Africa, South Africa, South India, Near and Middle East, and Latin America, east of the Andes. Globally, the estimated annual number of scorpion stings exceeds 1.2 million and the number of deaths exceeds 3250 (0.27%). 3 Deaths from scorpion stings are usually due to pulmonary edema and cardiogenic shock, whereas post-sting anaphylactic shock can also cause mortality.1,5 The type, age, and size of the scorpion, nutritional status, number of stings, venom injection depth, the sting being located closer to the head and neck, and age and health status of the patient may affect the clinical course. 6
Scorpion venoms are mixtures of many biologically active components, some of which are hemolysins and neurotoxins; the latter often act on ion channels. 7 When bound to these channels, inactivation is inhibited, leading to neuroexcitation and thus prolonged depolarization. 1 Because of these properties, scorpion venom can cause neurological, cardiovascular, hematological, and renal effects and local findings, such as pain, redness, burning, and swelling. 8 Scorpion stings more frequently cause local effects rather than systemic envenomation. Pain is usually sudden, intense, and persistent; recurrence/relapse after recovery may occur. 9 The main pathogenesis of pain is the sensitization of nociceptors via substance P and serotonin release at the site of the sting or the increase in smooth muscle contractions through the inhibition of potassium channels by the toxin. 10 In most cases, the pain lasts for 2 h after the scorpion sting and can last for an average of 15 h and sometimes 24 h. Also, this pain can refer throughout the regional dermatomes.3,11
The main elements in the management of scorpion stings are fluid replacement, tetanus vaccine, antivenom administration, use of analgesics, and use of antibiotics if necessary. Although it is the most effective method, the use of antivenom has been further challenged because it may lead to allergic complications. 12 Pain relief is the major concern in the first response to scorpion sting in the emergency department (ED). Paracetamol, ice application, and lidocaine have been recommended as analgesics in scorpion stings. However, there are insufficient studies in the literature to clarify which method is more effective. 9
In this study, the analgesic efficacy of IV paracetamol, IV dexketoprofen trometamol, topical lidocaine, and placebo was compared in scorpion stings, which account for a large number of presentations to the ED in our region.
Methods
This randomized, double-blind, placebo-controlled study was conducted between September 1, 2020, and August 31, 2021, in the ED of a tertiary hospital with 350,000 annual patient admissions. The hospital is located in southeastern Turkey, and the patients included in the study were also from that region. The study was designed as a superiority trial to determine which drug would provide better analgesia in scorpion stings. Written consent was obtained from all patients before inclusion in the study. Ethical approval was received from the central ethics committee (number: 2019-5-1, date: March 28, 2020), the Turkish Medicines and Medical Devices Agency (ID: 20-AKD-100), and the study was registered at
All patients aged 18 y and older, who presented to our ED with the main complaint of pain after scorpion stings, which were determined as grade I, were included in the study in a consecutive manner. Patients who refused to participate in the study, those with grades II to IV scorpion stings, those with known allergies to the drugs to be used in the study, pregnant women, patients with renal disease, and patients who had taken analgesics within 6 h before presenting to the ED were excluded. The cases who were admitted to the ED more than 6 h after the sting were also excluded. Patients were screened for eligibility in the study for 24 h a day and 7 d a week. A senior emergency medicine resident or emergency medicine specialist determined patients’ eligibility for enrollment. Unfortunately, the presenting patients did not provide scorpion specimens for identification and described features were insufficient for the assignment of the possible species responsible for the sting(s). Although some of these stings may be considered “presumed,” the patients presented with history and signs/symptoms fully consistent with scorpion sting/local envenoming.
In the evaluation of eligibility for inclusion in the study, the grading of scorpion stings was performed as follows: grade I if there were only localized reactions such as pain and/or paresthesia at the site of the scorpion sting; grade II if fever, chills, profuse sweating, nausea, vomiting, diarrhea, hypertension, and priapism were present; grade III or IV if there were systemic symptoms such as cranial nerve abnormalities, somatic skeletal neuromuscular dysfunction, nausea, vomiting, and pulmonary edema. 14
As the 4 inventions being compared included IV and topical delivery methods, all participants received 2 interventions: 1 IV and 1 topical. A topical drug, not exceeding 5 g in total, was applied to and around the site of the scorpion sting. The placebo group received both 100 mL of normal saline IV and an ointment with the same color, hardness, and odor as lidocaine. The lidocaine group received both 100 mL of normal saline IV and 5 g of 5% topical lidocaine (Anestol ointment; Sandoz). The test IV groups either received 1 g of IV paracetamol (Perfalgan; Bristol Myers Squibb) or 50 mg of IV dexketoprofen trometamol in 100 mL of normal saline (Arveles; UFSA) and the placebo topical application. The package of the serum and cream used was covered so that the label was not seen. All the IV administered drugs had the same color and package shape. In patients with insufficient pain relief after 60 min, 1 mg·kg−1 tramadol in normal saline was applied as an IV infusion (Madol ampule 100 mg; Koçak Farma) as a rescue medication. All the treatments were performed following local wound care practices, and tetanus prophylaxis was performed in cases where required.
Randomization blocks were created on the computer by a person blinded to the study. The group to which each patient was assigned was determined by letters written in an opaque envelope. A senior emergency medicine resident or emergency medicine specialist identified the patient to be included in the study, and one of them obtained written informed consent from the patient. Afterward, the preprepared envelope was opened by the nurse who prepared the medicines. In this envelope, statements such as group A-treatment X and group B-treatment Y were written. Another nurse who was blinded to the identity of the medication was responsible for treating the patient. At the same time, the doctor recorded the first visual analog scale (VAS) measurement before starting the treatment. The doctor who followed the treatment made VAS measurements again at 30 and 60 min and recorded them in the patient’s file. The data obtained with these code names were given to the statistician. The statistician also was blinded to group and medication. The physician, nurse, patient, and statistician remained blinded to the drug groups of the patients until after the last patient completed the study and the statistical analysis was completed. At this stage, the groups were identified for the team writing the article and evaluating the results.
The 100-mm VAS (0, no pain to 100 mm, excruciating pain) was used to measure the pain intensity. It is based on the fact that the patient indicates the pain that they feel by marking on a line, and it is frequently used in healthcare for measuring pain intensity and pain follow-up. 15 Previous VAS scores were not made available to the patient. Then, a different physician measured this marking place with a ruler from point 0 (cm scale ± 0.5 mm). Pain measurements were performed at the time of presentation and at 30 and 60 min. Drug side effects were investigated by the physician who followed up the patient by observing and asking them. If there was no regression or improvement in their pain after 60 min, rescue medication was administered.
The primary outcome measure was the change in the VAS pain score at 30 and 60 min. We had planned to measure at 15, 30, and 60 min in the study. However, after the study started and several patients were recruited, we observed that the analgesics did not show any effect within 15 min. For this reason, we changed the VAS measurement times to 30 and 60 min and adjusted the outcome measurements accordingly. The secondary outcome measures were the need for rescue medication and drug side effects.
The sample size was estimated using G-Power for Mac OS X (version 3.1.9.2; Universitat Düsseldorf). To detect 15-mm differences in VAS scores, 8 assuming a 2-tailed alpha value of 0.05 and a standard deviation of 19 mm according to a study on analgesic use in back pain, 16 we calculated that there should be a minimum of 27 patients in each group to reach 80% power.
In the study, the conformance of numerical data to the normal distribution was determined with the Shapiro-Wilk test, and Levene’s statistics were used for the homogeneity test of variances. At baseline, groups were compared as appropriate using either the 1-way analysis of variance or the Kruskal-Wallis H test. A repeated-measures mixed-model analysis of variance was used for simultaneous statistical analysis of pain scores at 30 and 60 min to compare the treatment groups. Group differences were identified pairwise using the Tukey honestly significant difference test or Bonferroni’s multiple comparisons. As appropriate, categorical variables were compared using the χ2 test or Fisher exact χ2 test. Results were reported as counts and percentages. A P value of <0.05 was considered statistically significant. Results were reported as mean±SD or median (interquartile range). All the data were analyzed using SPSS version 22.0 and Graphpad version 8.0.2.
Results
A total of 161 patients were identified to have presented to the ED with scorpion stings during the study period. Of these, 8 refused to participate in the study, 15 had taken analgesics before presenting to the ED, 3 were allergic to analgesics, 12 had systemic envenomation findings, 2 were not able to cooperate (intellectual disability), and 1 was pregnant; therefore, these patients were excluded from the study. The remaining 120 patients were randomized into 4 groups (30 individuals in each group). After inclusion in the study, 4 subjects in the dexketoprofen trometamol group, 5 subjects in the topical lidocaine group, and 5 subjects in the placebo group were excluded from analysis because of deviations in following the protocol (request for withdrawal of data use). The excluded cases did not receive allocated interventions. Ultimately, the study was conducted with 106 patients. A participant flow diagram is shown in Figure 1.
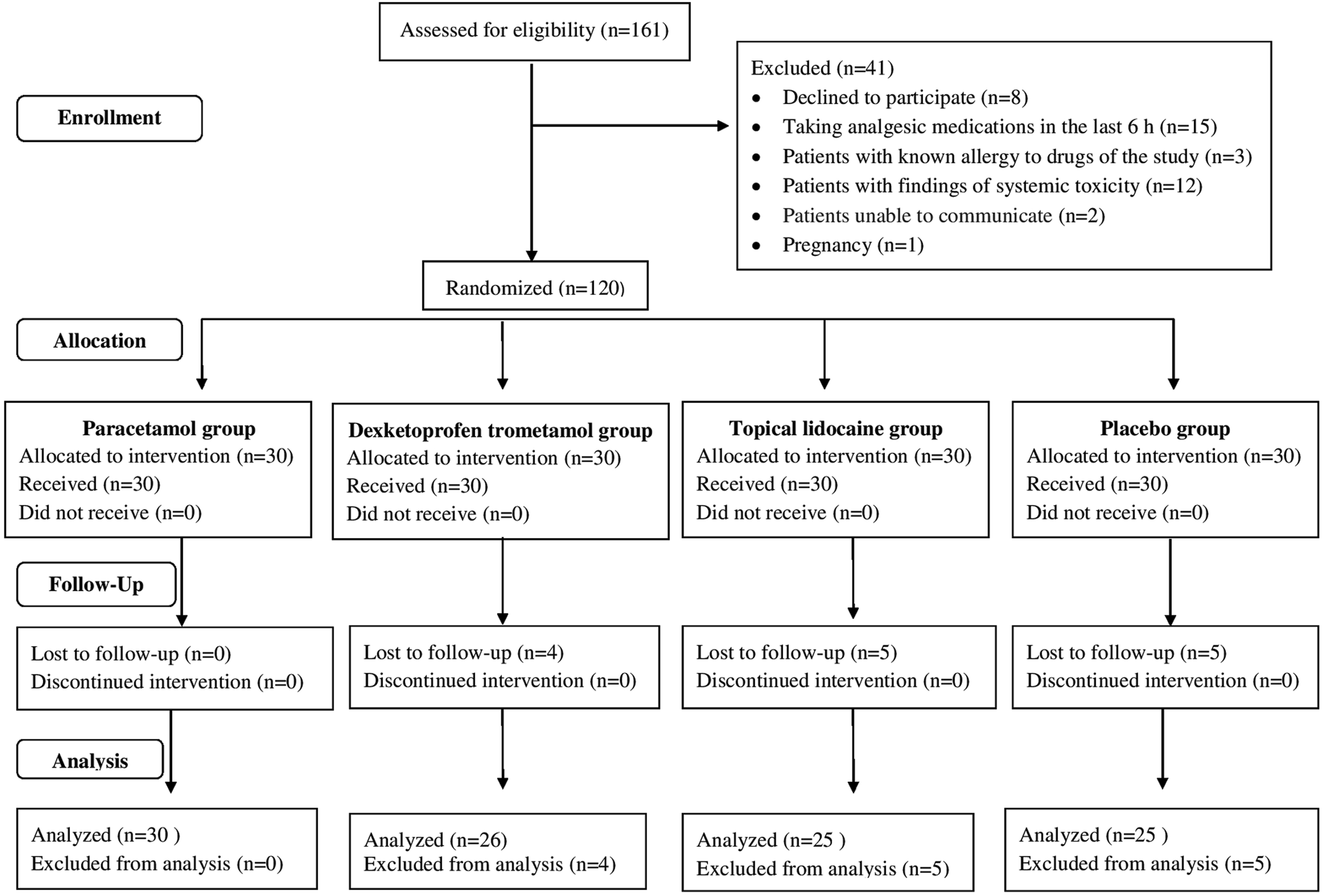
Participant flow diagram.
Among the patients included in the analysis, 1000-mg IV paracetamol was given to 30 subjects, 50-mg IV dexketoprofen trometamol to 26 subjects, and topical lidocaine ointment not exceeding 5 g to 25 subjects. Twenty-five people were included in the placebo group. The age of the whole sample was 43±17 y, and no significant difference was found between the groups (P=0.127). The female ratio was 57%, and there was no significant numerical difference between the groups in terms of sex (P=0.796). The heart rate of the patients was 91±15 beats·min-1 and the mean arterial pressure was 91±14 mm Hg, and neither significantly differed between the groups (P>0.05) (Table 1).
Characteristics of patients
MAP, mean arterial pressure; VAS, visual analog scale; VAS0, visual analog scale score at presentation; WBC, white blood cell.
Arrival time is presented as median (interquartile range); age, pulse, MAP, WBC, and VAS0 are presented as mean±SD.
The scorpion stings were mostly located in the right upper extremity (35%), followed by the right lower extremity (23%), upper left extremity (19%), lower left extremity (15%), multiple areas (5%), and trunk (4%). Sixty-seven percent of the scorpion sting presentations occurred in June, July, and August.
There was no statistically significant difference between the groups regarding the VAS scores obtained at the time of presentation (P=0.212, Table 1). Between the time of presentation and 30 min, there was no significant difference in the VAS change scores among the 4 groups (P=0.185). There was a significant difference among the 4 groups in the VAS change scores at 60 min (P<0.001). The post hoc test indicated no significant difference among the 3 drug groups, but the patients in the placebo group had significantly less pain reduction than those in the paracetamol and dexketoprofen trometamol groups. The VAS score changes were not significantly different between the topical lidocaine and placebo groups for 0 to 60 min (P=0.330). Changes in VAS score within 30 and 60 min were statistically significant in the paracetamol (P=0.0013) and dexketoprofen trometamol groups (P<0.0001) but not in topical lidocaine (P=0.0858) and placebo groups (P=0.5904) (Table 2).
Comparison of theVAS score changes between the treatment groups
A one way repeated measures Anova test showing the P value of the treatments effect
The groups sharing the same superscript letter are not significantly different (P<0.05, Tukey’s test)
The Bonferroni adjustment was used for pairwise comparisons.
Figure 2 presents the graph of the changes in the VAS scores at 0, 30, and 60 min and reveals the differences among the study groups. Rescue medication was required in 39% (n=41) of the whole sample, and no adverse drug effect occurred in any patient. There was no significant difference among the groups in the percentage requiring rescue medication (P=0.2566); 27% in the dexketoprofen trometamol group, 33% in the paracetamol group, 44% in the topical lidocaine group, and 52% in the placebo group.
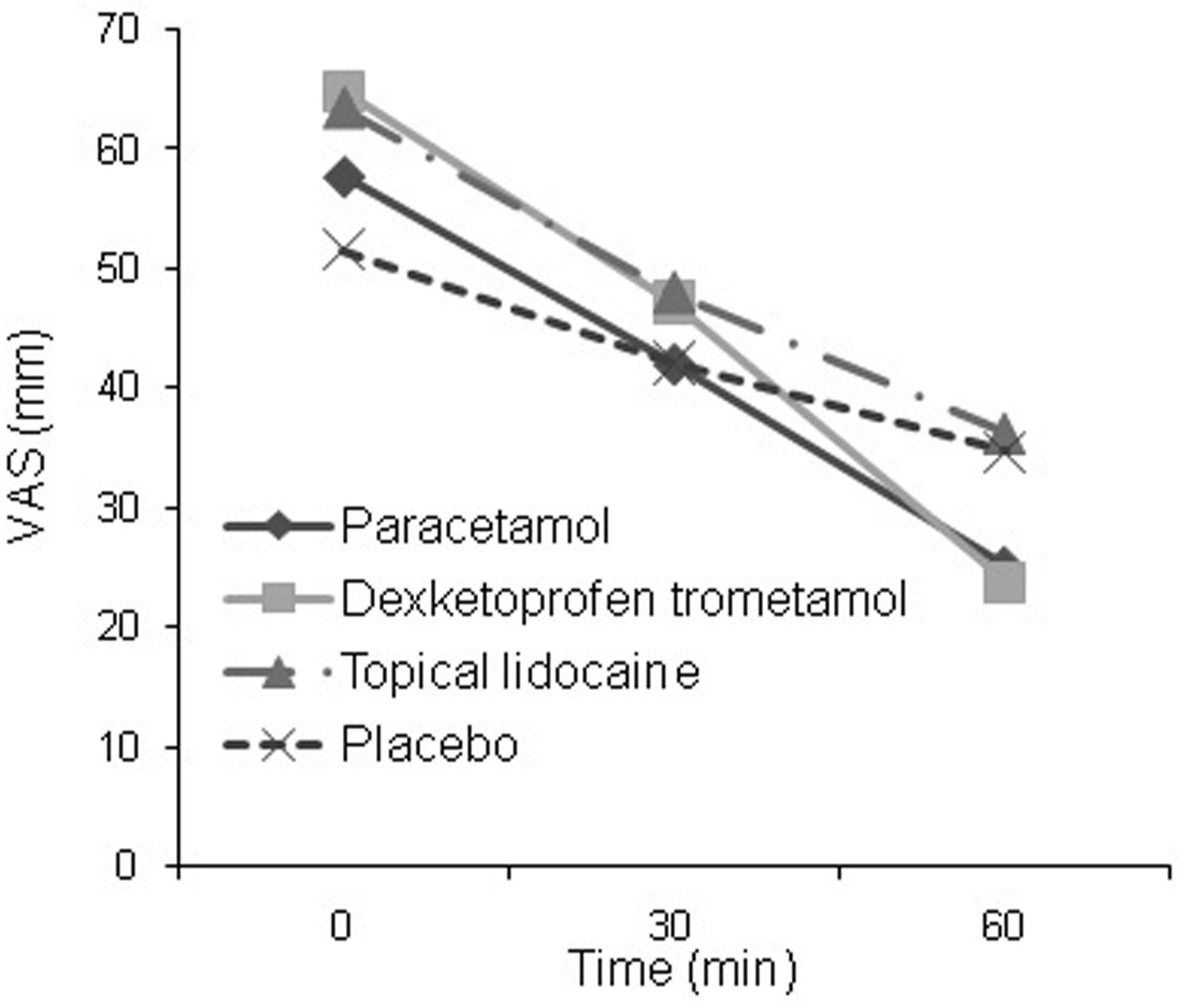
Mean VAS scores of the patients in intervention group.
Discussion
The most common symptom after a scorpion sting is pain at the site of the sting.6,7,12,17,18 In cases of scorpion stings without systemic findings, providing analgesia is one of the most important steps of emergency intervention. However, as stated in a meta-analysis, there are insufficient studies that determine the analgesic(s) that are most effective for scorpion stings. 1
The only study in the literature comparing analgesics for scorpion stings was undertaken in Turkey. 9 The authors compared the analgesic efficacy of paracetamol, topical lidocaine, and ice application methods but did not use a placebo. Among these methods, topical lidocaine was reported to provide more effective analgesia. They obtained a median 40-mm VAS score decrease with topical lidocaine in the first 60 min, whereas our study showed a mean decrease of 27 mm with topical lidocaine, 33 mm with paracetamol, and 41 mm with dexketoprofen in the same time. 9 We did not find that IV paracetamol, IV dexketoprofen trometamol, topical lidocaine, and placebo had different analgesic effects in the first 30 min. IV paracetamol and dexketoprofen trometamol showed analgesia equal to that of topical lidocaine and superior to that of placebo in the first 60 min. No differential analgesic effects of topical lidocaine and placebo were found in the first 60 min.
The topical form of lidocaine, a local anesthetic agent, can be used in the management of acute and chronic pain due to its few systemic side effects and effective analgesic properties. 19 In the literature, effective analgesia was achieved with the preprocedural application of topical lidocaine 20 for arterial gas sampling 21 for thoracentesis and abdominocentesis. Topical lidocaine has also been suggested to be more effective than paracetamol and ice application for pain relief of scorpion stings. 9 We determined that topical lidocaine provided analgesic efficacy similar to paracetamol and dexketoprofen trometamol. We did not find any study comparing topical lidocaine and IV dexketoprofen trometamol in the literature. In studies comparing IV lidocaine and IV dexketoprofen trometamol in patients with migraine, the former was shown to provide a more effective analgesia than the latter.22,23
Different treatments have been tested in the literature for the management of pain caused by scorpion stings. It was reported that the use of alcohol in scorpion stings did not provide sufficient analgesia. 24 In addition, effective analgesia was provided in 1 case where chloroquine was used 25 ; however, apart from this single case report, there is no other study on chloroquine in the literature. Other studies suggest that the use of nonsteroidal anti-inflammatory drugs such as aspirin may provide symptomatic benefits, but caution is warranted as it may cause Reye’s syndrome in children; IV non-steroidal anti-inflammatory drugs may also be contraindicated in patients with increased risk of renal insufficiency. Despite being very effective, morphine and its derivatives or analogs (codeine and tramadol) should be avoided because opioid receptor agonists inhibit noradrenaline reuptake, which may potentiate their effects. They may also worsen the patients’ respiratory function by causing respiratory depression. 26
Limitations
There were some limitations to our study. First, the number of patients in the groups was not equal. We planned to study an equal number of patients in each group; however, some of our patients were excluded from the study during follow-up, and those who dropped out caused the number of patients in the groups to be unequal. Additionally, the 4 groups had significantly different dropout rates, and this implies that the blinding may not have been effective or that the equivalence at baseline may not have been maintained. The pattern observed in ineffective blinding and dropout is consistent with a negative preference for topicals and a strong positive preference for IV groups. Second, we measured patients’ pain with the VAS, which is a subjective scale, and the pain threshold of individuals was different for each person. Third, we did not know the species of scorpions that caused the envenomation, which is an important limitation. Fourth, the follow-up time (1 h) was limited because of the overcrowded nature of our ED. Finally, the fact that we did not register the patients who came 6 h after the sting and consequently we did not have patients’ data was an important limitation.
Conclusions
We found that paracetamol and dexketoprofen trometamol provided superior analgesia compared to placebo in the first 60 min after local envenoming from a scorpion sting that did not cause systemic symptoms. In secondary analyses, we did not observe a difference in analgesic efficacy between paracetamol and dexketoprofen trometamol or between paracetamol and topical lidocaine. The analgesic effects of topical lidocaine and placebo were comparable.
Footnotes
Acknowledgments
The authors are indebted to the nurses of their clinic for their help with patient care. The authors gratefully acknowledge the assistance of Associate Prof Fatih Üçkardes, for his contribution to the statistical editing.
Author Contributions: study concept and design (KT, EY); acquisition of the data (İA, NA, EA); analysis of the data (UG, KT); drafting of the manuscript (EY); critical revision and approval of the final manuscript (all authors).
Financial/Material Support: None.
Disclosures: None.