
Abstract
Nonfreezing cold injury (NFCI) is caused by prolonged exposure to cold, usually wet conditions and represents a separate pathological entity from frostbite. The pathophysiology of NFCI is characterized by vasoconstriction and microcirculatory disturbance. Iloprost, a synthetic prostaglandin analogue with vasodilatory properties is a recognized adjuvant treatment in frostbite; however, its role in NFCI is unclear. We present a case of a 29-y-old man with severe NFCI to both forefeet after prolonged immersion in cold seawater. Initial treatment with passive rewarming, analgesia and aspirin was initiated. Infusion of iloprost was used within 24 h from presentation and was well tolerated. This resulted in reduced tissue loss compared to the apparent tissue damage documented during the initial assessment. Delayed surgical intervention allowed minor debridement and minor toe amputations, maintaining the patient’s ability to ambulate. This case demonstrates the safe use of iloprost in acute NFCI and highlights the importance of delayed surgical intervention in patients presenting with severe NFCI.
Introduction
Nonfreezing cold injury (NFCI) occurs when tissues are exposed to cold temperatures (below 15oC) for prolonged periods of time, usually greater than 48 to 72 h. 1 Tissue freezing does not occur, differentiating NFCI from frostbite. NFCI largely affects extremities, most commonly feet exposed to cold and wet environments. A number of named conditions including “trench foot” and “immersion foot” are synonyms for NFCI, where either immersion or cold are the precipitating factors. 2
Proposed mechanisms of injury in NFCI have been extrapolated from animal studies. The true mechanisms have yet to be fully established in humans. There are several postulated mechanisms, including reperfusion injury after prolonged vasoconstriction. 2 Persistent vasoconstriction may result in capillary endothelial injury as well as leucocyte and platelet aggregation with subsequent microvascular thrombosis.2,3 Damage to nerve tissue occurs through both ischemic and direct cold-induced injury. 2 Upon rewarming, free radical formation results in further endothelial damage and tissue edema.1,2 Cold induced vasodilation attempts to disrupt persistent vasoconstriction, cycling every 5 to 10 min providing core temperature is maintained. 1 Although some of these mechanisms may be also found in frostbite, the key difference is that tissue freezing does not occur in NFCI.
NFCI provides diagnostic challenges and can present with few objective signs. 2 It often progresses through 4 clinical phases. 3 The initial cyanotic phase occurs where the extremity is insensate and painless due to severe vasospasm. 2 During rewarming, the prehyperemic phase begins with some circulatory improvement and a blanched or mottled appearance may be seen. 2 After rewarming, the hyperemic phase occurs, where the extremity is often painful, oedematous, and swollen. 2 Pulses may be present; however, there is frequently microcirculatory impairment evidenced by prolonged capillary refill time. 2 Hyperalgesia and paresthesias may also occur. 2 Blistering, eschar formation, and desquamation may occur in severe cases, although gangrene is rare. 2 The posthyperemic stage is characterized by abnormal response to cold such as rapid onset of vasospasm or hyperemia, as well as cold sensitivity and parasthesias that may persist years after injury. 2 Not all phases are always present and frequent overlap and varying durations of each phase occurs. 2 This variation is likely related to the severity of the vasoconstriction and the inflammatory process resulting from tissue damage. 2
Given the role of vasoconstriction in NFCI, iloprost has been proposed as possible treatment modality. Already a recognized treatment of acute frostbite, iloprost is a synthetic prostaglandin I2 analogue with vasodilatory properties. 4 It has an inhibitory effect on platelet aggregation and also stimulates release of endogenous tissue plasminogen activator, resulting in a thrombolytic effect. 5 The intravenous infusion is started at 0.5 mcg·kg·min-1, incrementally increased every 30 min by 0.5 mcg·kg·min-1, up to a maximum of 2 mcg·kg·min-1. Common side effects such as sweating, headache, or hypotension can be managed with reduction of infusion rate. The infusion is commonly prescribed for 5 to 8 d.
Case Presentation
A 29-y-old man with a history of substance abuse presented with severe pain and numbness in his feet, having spent 3 d trapped in a tidal cave on the coastal shoreline. The patient had no previous history of cold exposure. During this time, both feet, in socks and shoes, were intermittently submerged in sea water. Ambient temperatures at the time of injury ranged from 4 to 10°C with an average seawater temperature of 10°C. He was found hypothermic with a tympanic (infrared) temperature of 34°C. On presentation to the emergency department, he remained cold-stressed at 35.8°C on tympanic reading but was hemodynamically stable. Both feet were cold, pale, and without discernable capillary refill up to the ankle. Pulses were absent, but bilateral weak monophasic extremity doppler signals were present. Blood tests showed an elevated white cell count of 22.3 109·L-1, normal electrolytes, and renal function but a creatinine kinase of 21454 u·L-1. A working diagnosis of a severe NFCI was made.
Initial treatment of cold exposure was started with patient warming and passive rewarming of both feet, intravenous paracetamol analgesia, and intravenous fluids. Paracetamol was initially chosen because of concern for acute kidney injury with the high creatinine kinase. Repeat renal function testing was normal, however, with the patient maintaining good urine output without myoglobinuria. Computerized tomographic angiography (Figure 1) demonstrated reduced contrast flow in all 3 runoff vessels consistent with severe vessel spasm without any occlusive lesions. On telephone discussion with author CI of the British Mountaineering Council frostbite advice service, aspirin 75 mg and ibuprofen 400 mg were also administered.
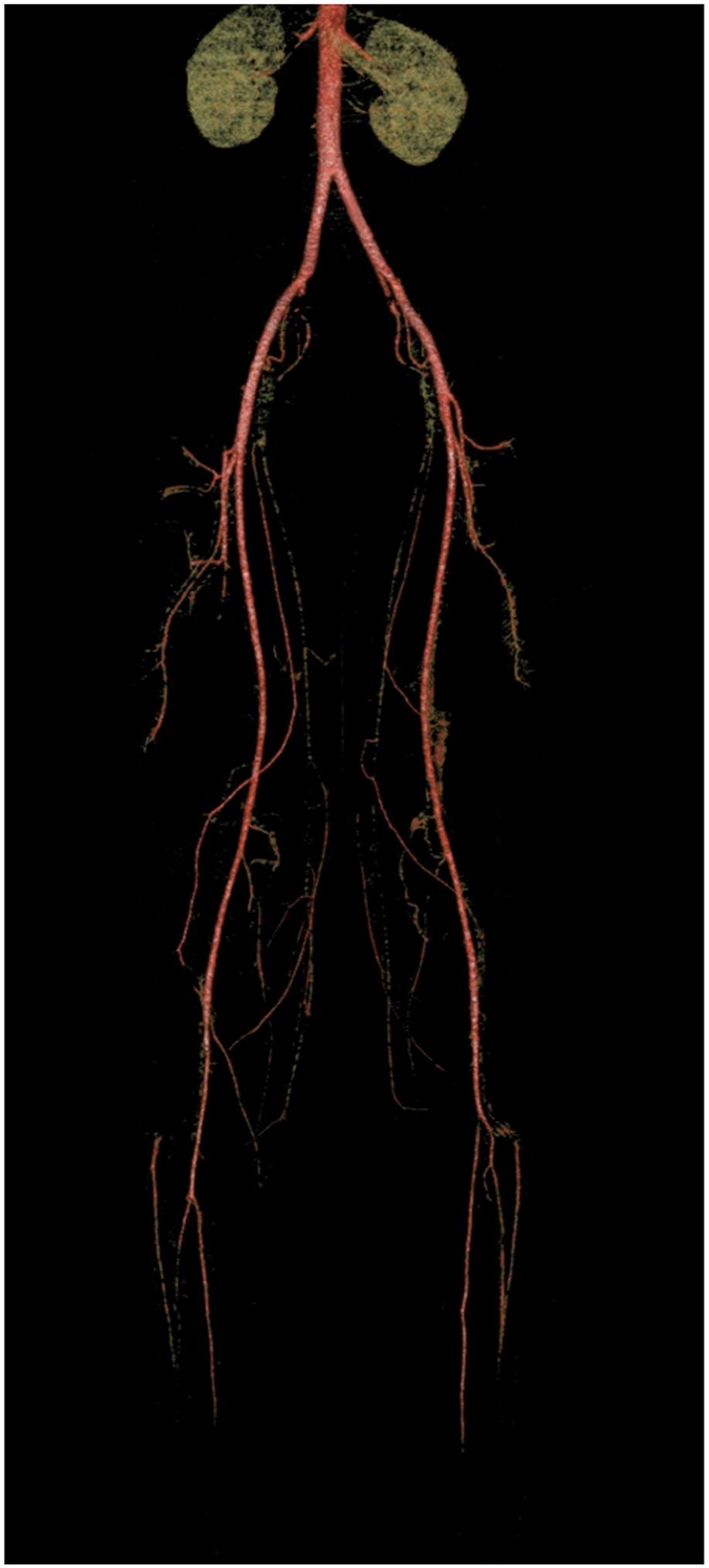
Computed tomography angiogram reconstructions demonstrating intact major vessel with spasm of pedal arteries bilaterally.
Despite initial management, the patient was still experiencing severe pain and pregabalin was added alongside opiate analgesia on advice from anesthesiology. Passive rewarming of the feet was stopped at this point and the feet were lightly dressed.
The patient was admitted to the high dependency unit for ongoing pain management and monitoring of renal function. A fentanyl epidural and morphine patient-controlled analgesia pump was provided due to ongoing intractable pain. In the high dependency unit, dusky discoloration was noted in all toes, more severe on the plantar surface of both feet. After further telephone discussion with author CI, an iloprost infusion was started within 24 h of presentation. This was continued initially for 5 d but extended to 10 d because the initial 5 were tolerated well and clinical improvement was noted (Figures 2 and 3).

After 6 d of iloprost infusion.

Improvements in appearance seen on Day 13 after 10 d of iloprost infusion.
On days 5 to 7 of iloprost infusion, the patient reported sweating and headaches. This resolved with reduction of the infusion rate. Pain control improved throughout the course of the infusion. A rise in serum transaminases was also noted at this time, returning to normal on discharge. Two weeks after initial presentation to hospital, the patient was discharged to a rehabilitation hospital on paracetamol, ibuprofen, and aspirin for ongoing rehabilitation. Aspirin was continued until surgery with the aim of further reducing any tissue loss secondary to microvascular thrombosis.
Sixteen weeks after admission, elective debridement of both feet was performed. Bilateral distal hallux amputations, left second, right fourth and fifth toe amputations were performed under regional anesthesia. The patient retained a significant amount of tissue on both hallux amputations sites and was ambulatory on discharge from a community hospital. The distal toes had remained painful and regular paracetamol analgesia was still required for walking although outside the affected area no abnormal sensation was reported.
The patient recovered well postoperatively but was lost to follow-up despite multiple efforts to contact him.
Discussion
To the best of our knowledge, this case represents the first use of several treatment strategies. Initial management with aspirin, as used in frostbite, was used to reduce cold-induced platelet aggregation. 6 Ibuprofen was chosen as analgesia in addition to suppressing the inflammatory response. This was used alongside recommended basic management including passive rewarming and limb elevation.1,6 Given the history of substance misuse, computerized tomographic angiography was used to rule out occlusive lesions. In this case, it demonstrated the marked vasospasm typical to NFCI.
Iloprost was utilized in this acute setting with the rationale of reducing the extent of tissue injury in the affected extremities through its vasodilatory and thrombolytic effects. Further administration did result in side effects, although these rapidly resolved on reduction of infusion rate. Previously reported use of iloprost in NFCI describes a single patient who experienced NFCI 20 y prior to presentation with chronic pedal pain and loss of function. 7 After treatment with iloprost, a 4-wk improvement was noted. 7 Recurrence of symptoms occurred after this period and subsequent infusion resulted in worsening symptoms and increasing analgesic requirements. 7 In chronic settings, tissue damage has already occurred and may explain the poor response to iloprost. Attempting to reduce the length or severity of the microcirculatory disturbance and therefore tissue damage in the acute setting appears beneficial. Unfortunately, the patient was lost to follow-up. Therefore, it is unclear whether there was any long-term benefit in iloprost administration in NFCI.
Pain management was challenging in this case given the history of substance misuse. Neuropathic pain is often treated with amitriptyline (50–100 mg orally) with or without pregabalin. 2 Currently, there is no evidence of the most effective agent against neuropathic pain in NFCI, although amitriptyline has been the first line agent in the UK armed forces protocol since 1982. 2 Involvement of anesthesiology for consideration of regional block or epidural may be appropriate and was key to successful pain management in this case.8,9 Unfortunately, it was not clear from the documentation as to why pregabalin was chosen as opposed to amitriptyline. This is likely due to the lack of awareness in managing NFCI.
This case also highlights the importance of delayed surgical management in NFCI. Surgical management is undertaken once the full extent of the injury is understood, as demarcation can take several days to months. 3 The extent of the apparent tissue damage changed significantly during the patient’s inpatient stay; early surgery would have resulted in unnecessary loss of viable tissue. Therefore, surgical treatment should be delayed in line with recommendations for frostbite.6,10
Conclusions
NFCI is an entity with variable presentation and history of exposure to cold and wet conditions should alert the clinician to its possibility. Key factors in the management of NFCI include passive rewarming, analgesia, and delayed surgical management. Iloprost may have a role in the acute management of NFCI.
Footnotes
Acknowledgements
Author Contributions: Data acquisition (AT, TL); drafting and critical revision of manuscript (AT, TL, SV, CI, RB); approval of the final manuscript (all authors).
Financial/Material Support: None.
Disclosures: CI is advisor for UK frostbite advice service.