
Abstract
Hymenoptera stings of the upper airway are rare events, but can result in rapid, life-threatening airway emergencies. The allergenic and toxic mediators that are released from the stings of bees, wasps, and hornets can cause local tissue inflammation and edema with subsequent upper airway obstruction. We report the case of a 15-y-old girl who suffered a bee sting to the uvula while zip-lining in Costa Rica. Shortly thereafter, she developed a choking sensation with associated dysphonia, odynophagia, drooling, and respiratory distress. She was brought to a rural emergency medical clinic where she was noted to have an erythematous, edematous, boggy uvula, with a black stinger lodged within it, as well as edema of the anterior pillars of the tonsils and soft palate. The stinger was removed with tweezers and she was treated with an intravenous corticosteroid and antihistamine. She had persistence of airway edema and symptoms until the administration of epinephrine, which resulted in clinical improvement shortly thereafter. In our review of this case and the existing literature, we emphasize the importance of early recognition and management of hymenoptera stings of the upper airway, which should always include immediate manual removal of the stinger, and in cases with significant upper airway edema, the administration of epinephrine should be considered.
Introduction
Hymenoptera include bees, wasps, hornets, and ants, and comprise over 115,000 different species. Stings from bees, wasps, and hornets are responsible for an average of 62 deaths per year in the United States. 1 A 2009 study from Costa Rica reported on hymenoptera sting fatalities over a 22-y period, with a total of 52 deaths over the study period (average 2 deaths per year). 2
Several reports of hymenoptera stings of the upper airway have been published in the medical literature. 3 -9 These events can be life threatening and require immediate recognition and emergency medical care.10,11 Bee stingers have microscopic barbs that detach from the bee with a barbed end that enables it to remain embedded in the target tissue. 12 Proximal to the stinger, there is often an attached venom sac with a mechanism that continues to pump venom into the tissue after detachment via a piston-like muscular injection mechanism. 13
A sting within the oropharynx is of significant concern due to the risk of upper airway obstruction induced by subsequent local tissue inflammation and edema. Rapid treatment, including manual removal of the stinger, is essential to promote positive patient outcomes.14,15
Case Report
A 15-y-old female with no past medical history and no known allergies was ziplining in La Fortuna, Costa Rica. While moving at high speed through the air with her mouth open, a bee flew into her oropharynx where it remained lodged for approximately 5 s, after which she coughed it out. Within minutes she developed a sensation of swelling in her posterior oropharynx with associated dyspnea, dysphonia, odynophagia, and drooling. Thirty minutes later, she arrived at a local emergency medical clinic where she was noted to be in moderate respiratory distress. Blood pressure was 115/70 mm Hg, heart rate 120 beats·min-1, respiratory rate 30 breaths·min-1 and oxygen saturation 98% on room air. Physical exam was notable for no stridor, no lip or tongue edema, clear lungs, and no skin rashes or urticaria. The posterior oropharynx was noted to have extensive edema of the uvula, anterior pillars of the tonsils, and soft palate (Figure 1A). A black stinger was noted to be lodged in the uvula, which was manually extracted with tweezers. She was treated with intravenous dexamethasone 10 mg and chlorpheniramine 10 mg, a histamine 1-receptor antagonist, with subsequent persistence of respiratory distress, choking sensation, and tissue edema. Epinephrine 0.1 mg was administered by slow intravenous push over 5 min (the intramuscular formulation of epinephrine was not available), with improvement in symptoms shortly thereafter. Over the next 2 h, the airway edema continued to diminish (Figure 1B), and she was discharged from the clinic on prednisone 40 mg and rupatadine 10 mg daily for 5 d. Mild airway edema persisted for 12 h (Figure 1C), and ultimately the patient made a full recovery.
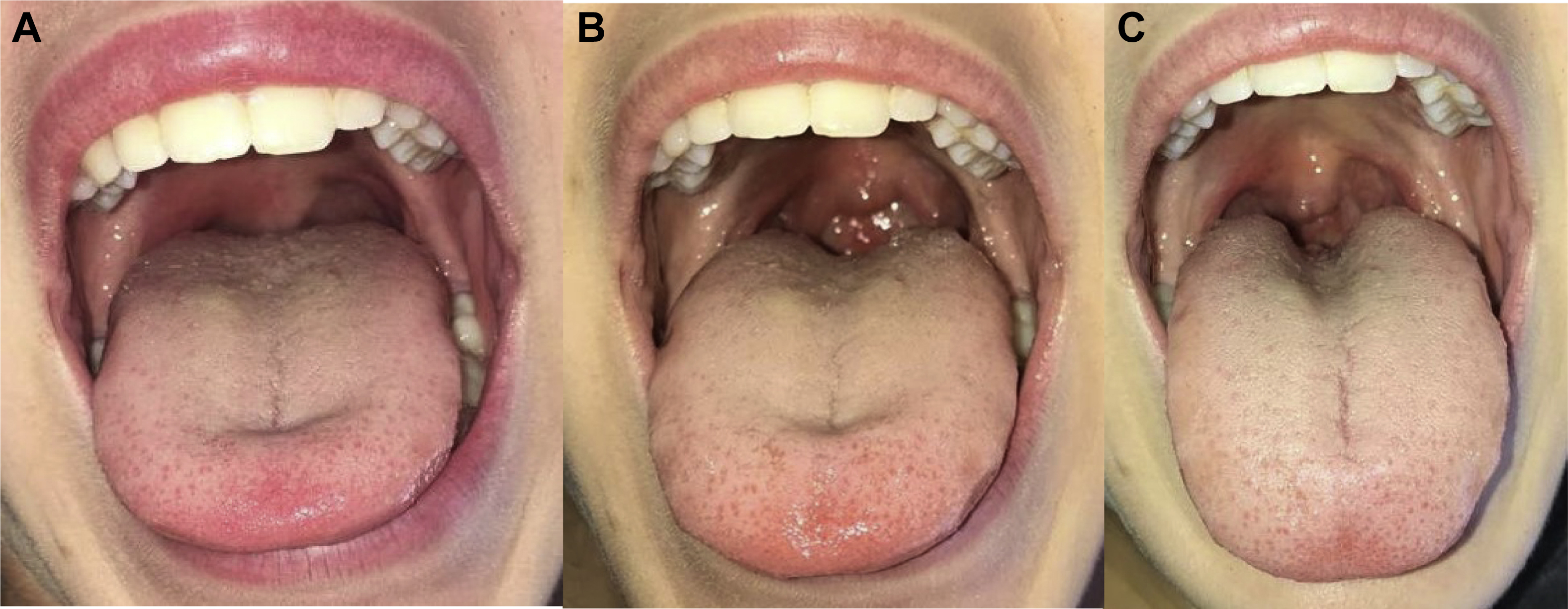
Edema of uvula, soft palate, and anterior pillars of tonsils. (A) After stinger extraction, prior to epinephrine. (B) Two hours after epinephrine administration. (C) Twelve hours after epinephrine administration.
Discussion
Although rare, awareness of the potentially life-threatening nature of hymenoptera stings to the posterior oropharynx, even in those without bee sting allergy, should be promoted among all emergency medical personnel. Clinicians should have increased suspicion of airway compromise and be exceedingly conservative in the management of oropharyngeal hymenoptera stings because even a local reaction can cause significant airway edema. It is crucial to perform a careful pharyngeal exam, and it is prudent to remove the stinger promptly. Rapidity of stinger removal with its attached venom sac is essential to prevent worsening of tissue inflammation and edema.14,15 Additional management strategies include the administration of corticosteroids, antihistamines, and epinephrine as deemed necessary by the treating clinician.
In the case presented here, epinephrine was used due to the lack of clinical improvement after stinger removal. The primary mode of epinephrine injection for anaphylaxis is intramuscular, with the intravenous route reserved for patients with circulatory collapse or impending respiratory arrest. 16 Epinephrine acts through the stimulation of alpha and beta receptors, with the alpha-1-adrenergic effects causing vasoconstriction in the precapillary arterioles of the skin and mucosa and smooth muscle contraction in the venous vascular bed, resulting in increased peripheral vascular resistance and blood pressure and reduction in vascular permeability and tissue edema. 17 The beta-2-adrenergic effects of epinephrine result in increased bronchodilation and decreased release of mediators of inflammation from mast cells and basophils. 18 The administration of antihistamines and corticosteroids is a mainstay of therapy to reduce the local inflammation caused by venomous insect stings, but in cases of significant upper airway edema, the addition of epinephrine may also be necessary.19,20 Additionally, after complete recovery, in vivo and in vitro diagnostic testing with skin tests utilizing hymenoptera venom extracts and analysis of serum for hymenoptera venom-specific IgE should be performed. 21 Large local reactions to hymenoptera venom can be caused by both IgE-mediated or cell-mediated allergic mechanisms. Systemic anaphylactic reactions are usually IgE-mediated, but can rarely be due to short-term sensitizing IgG antibodies or complement activation by IgG-venom complexes. 22 Allergy testing for hymenoptera venom is important in individuals who have had a large local sting reaction, as 5 to 15% will develop a systemic reaction with a subsequent sting. 23
Due to the potential for airway compromise, posterior oropharyngeal hymenoptera stings should receive prompt emergency medical treatment for stinger removal and the administration of potentially life-saving medications.
Footnotes
Acknowledgements
Author Contributions: Conception and design (ES, LL); data collection (ES); analysis and interpretation of results (ES); manuscript preparation (ES, LL); approval of the final version of the manuscript (ES, LL).
Financial/Material Support: None.
Disclosures: None.