
Abstract
Epinephrine autoinjectors are commonly used in urban environments for anaphylaxis. In remote environments, the effects of a single dose of epinephrine may diminish before one can access higher medical care. By retrieving additional epinephrine from common autoinjectors, a medical provider may be able to treat or delay decompensation of anaphylaxis in the field during evacuation. The new Teva epinephrine autoinjectors were obtained. The design of the mechanism was researched by studying patents and disassembling trainers and medication-containing autoinjectors. Multiple methods of access were tried to find the quickest, most reliable method that required minimal tools or equipment. A quick, reliable method of removing the injection syringe from the autoinjector using a knife was determined, as outlined in this article. The syringe plunger had a security design to prevent dispensing further doses from the syringe, so a long narrow object is also required to dispense additional doses. There are 4 additional doses of approximately 0.3-mg epinephrine in these Teva autoinjectors. Prior knowledge of epinephrine equipment and the devices that may be encountered in the field is important for providing life-saving medical care. The ability to retrieve additional doses of epinephrine from a used autoinjector can provide additional life-saving medication while evacuating to a higher level of medical care. This method does carry risks to rescuers and patients; however, it can potentially be life saving.
Introduction
Anaphylaxis is a life-threatening type 1 hypersensitivity reaction in which immunoglobulin-E–mediated degranulation of previously sensitized mast cells and basophils causes release of histamine and inflammatory mediators, which can lead to significant vasodilation, vascular permeability, and shock.1,2 Anaphylaxis can occur rapidly and be devastating in an austere environment. The lifetime prevalence of anaphylaxis is up to 2%, with a mortality rate of 0.7%.3,4
The most important intervention and first-line treatment is the administration of epinephrine. Medical providers frequently prescribe epinephrine autoinjectors to nonmedical personnel due to their ease of use. Most epinephrine autoinjectors are designed to provide a single dose of epinephrine. Due to the possibility of a biphasic reaction, epinephrine autoinjectors come in packages of 2. 5 Studies indicate that a second dose of epinephrine is required in 12 to 36% of cases with anaphylaxis. 6
Access to multiple autoinjectors is often lacking in the wilderness setting because of cost, size, or lack of preplanning. As a wilderness medicine provider, extracting additional doses of epinephrine from an autoinjector may be necessary. Hawkins et al 7 provided a comprehensive review on methods to retrieve additional doses of epinephrine from both pre- and post-2010 styles of EpiPen autoinjectors using the Roane State and Wilderness Medicine Outfitters methods as well as described methods for other autoinjectors. Robinson and Lareau 8 and Ganti et al 9 explored different techniques and autoinjectors as well. This article provides an update to research by outlining a method of extracting additional doses of epinephrine from the newer Teva autoinjector, which was approved by the US Food and Drug Administration (FDA) in 2018, which includes new challenges encountered due to the novel plunger mechanism used in this device. Extrication of additional doses is not approved by the FDA. 7 This method should only be performed when standard medication doses are unavailable in a wilderness setting. This technique should be practiced in a controlled setting prior to field use.
Methods and Results
No human subjects were used in this study.
A literature search for currently available epinephrine autoinjectors on the market was performed on PubMed with the aim to locate a cost-effective and commonly available model. At the time of this publication, the Teva autoinjectors were determined to be available at most large pharmacies in the United States, with a wholesale acquisition cost of around $300 USD with common insurance plans. Multiple Teva autoinjectors were obtained for use in this study. Patents for the autoinjector mechanism were studied to understand the mechanism and assembly of these autoinjectors. 10
Multiple methods of disassembly with various tools were attempted in order to access the remaining epinephrine doses. Failed attempts included trying to saw or cut through the outer housing, which was difficult with proper tools and too destructive to be a viable option for recovering the medication. The following method was the one that the authors concluded had the best chance of success in a wilderness setting with limited accessibility to tools. A video was created and is available to watch (see online Supplemental Video).
The initial dose was dispensed from the autoinjector per the manufacturer’s guidelines: remove the blue safety cap, twist off the yellow end cap, and dispense epinephrine into the outer thigh (a patient analog was used in this case). Once the initial dose has been dispensed, there will be an orange plastic sheath deployed around the exposed needle to prevent accidental needle-stick injury (Figure 1D).
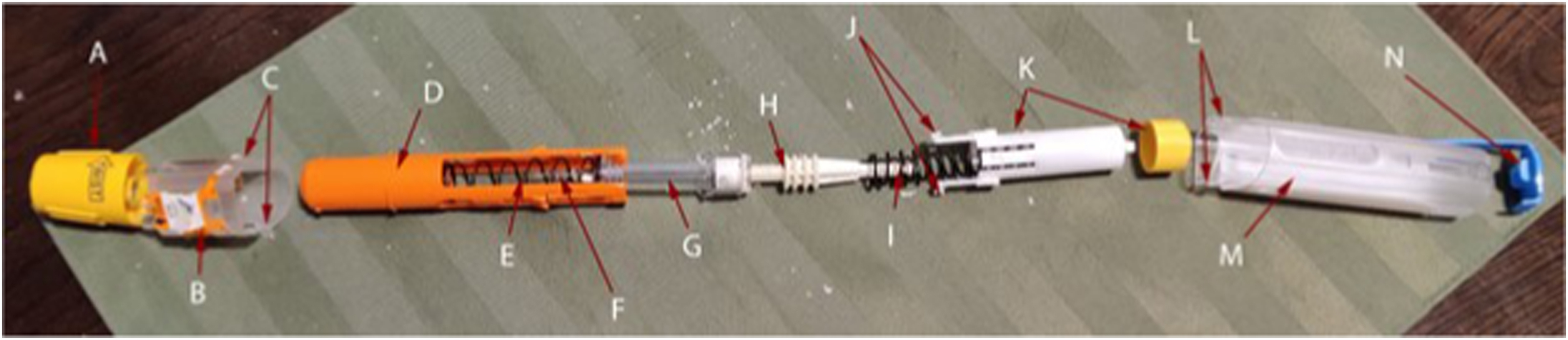
Expanded view of a broken down Teva epinephrine autoinjector. A, Yellow safety cap. B, Front outer plastic shell. C, Front part of the outer shell retaining clips. D, Orange plastic needle sheath. E, Spring for needle retraction. F, Needle. G, Syringe containing epinephrine. H, Plunger. I, Autoinjection spring. J, White plastic clips that attach to the syringe and keep the spring compressed. K, Initial dose autoinjector firing mechanism. L, Outer shell plastic clips that attach to the retaining clips on the front outer shell. M, Back outer plastic shell. N, Autoinjector safety clip.
Extreme care must be taken to prevent the needle from injuring another person or becoming contaminated as there is no cover or protection for it.
Removal of the Outer Shell (Figure 2A–E)
First, locate the seam on the outer clear plastic shell that divides the autoinjector into 2 parts. This is located near the orange sheath end of the autoinjector and is partially obscured by the label. The label needs to be scored with a knife along the seam so that the 2 clear plastic shell pieces separate. The seam travels diagonally up the sides of the autoinjector and straight across the front and back (Figure 2A). Caution should be taken when using a knife, and personal protection, such as leather gloves, should be used if available.
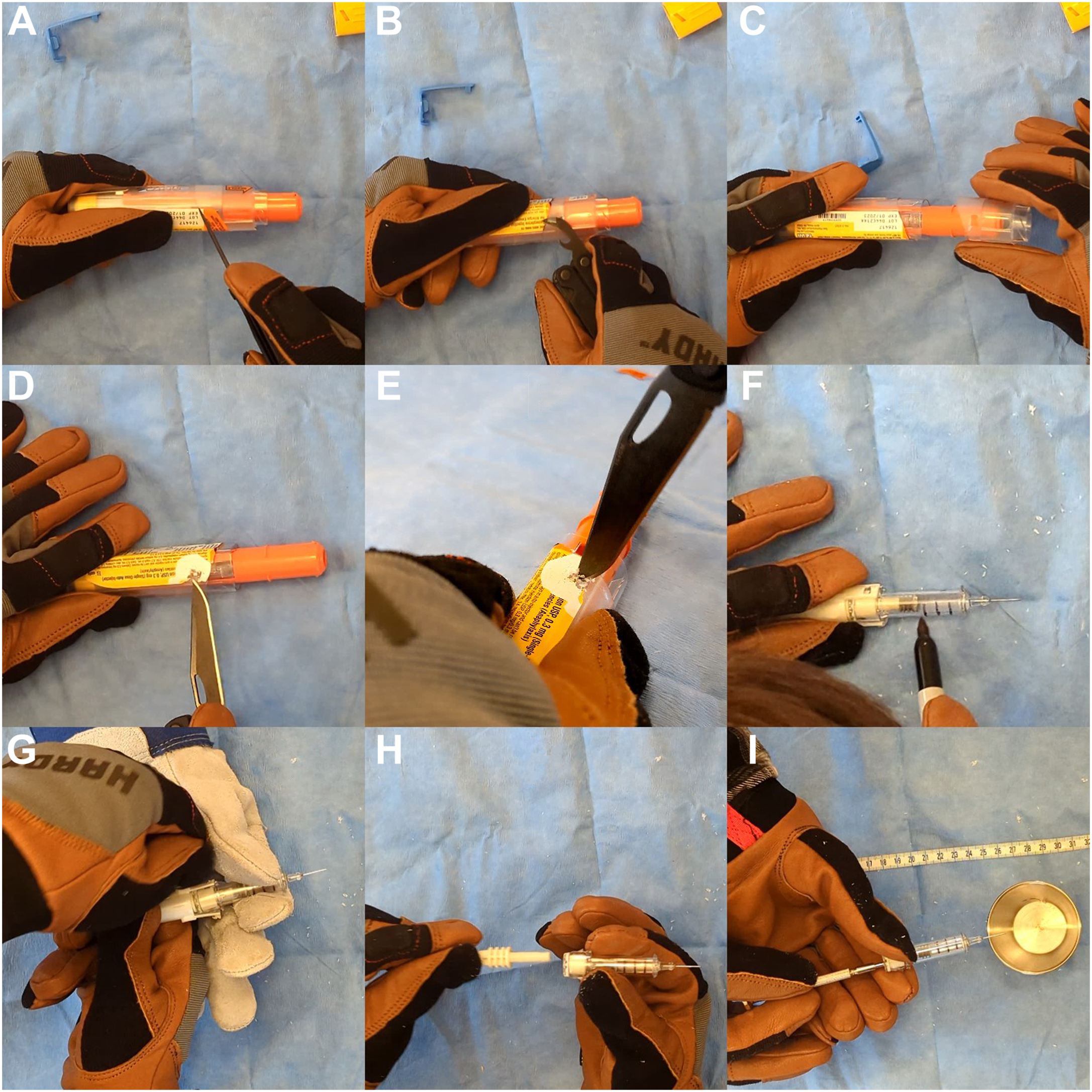
Steps for accessing additional doses of epinephrine: A, scoring label with a knife along the seam between the front and back of the outer plastic shell; B, using a can opener to slide under the retaining clips on the outer shell and prying up until they break on both sides; C, removing the front of the outer plastic shell; D, scraping off label to expose small, square, white clips holding the remainder of the outer shell in place; E, drilling out the small white clips on both sides until below the outer shell plastic; F, removal of outer shell exposing the syringe, marking the syringe for remaining 4 doses; G, prying open clips of the spring-loaded autoinjector mechanism that are attached to the syringe; H, demonstration of the plunger unable to push further into the syringe; I, using a screwdriver to advance the rubber stopper and dispense medication.
Next, there are 2 plastic clips holding the 2 parts of the clear shell together. They are located under the label on both sides closest to the orange sheath covering the needle (Figure 1C and L). Remove the label to expose these clips and then slide a metal object under the plastic containing the clip. A screwdriver, knife, or pocket can opener works well for this (Figure 2B). Pry back on this plastic that is holding in the clip until it breaks. Repeat on the other side.
With both clips broken and the label cut off the seam, the smaller part of the clear plastic outer shell (Figure 1B) should slide off the autoinjector and expose more of the orange shaft covering the needle (Figure 2C).
There are 2 smaller clips, sized at about 2×2 mm2, roughly 1 cm away from the end with the orange sheath. These may be felt through the label. Scrape away the label with a knife or fingernail to expose these 2 small, white plastic clips set below the surface of the clear plastic shell (Figure 2D). Use a sharp knife placed into this clip and start twisting it to “drill” out the white plastic clip. Continue drilling until the white plastic clip is below the level of the clear plastic outer shell (Figure 2E). Repeat the process for the matching clip on the other side.
Removal of the Syringe From the Sheath (Figure 2F–H)
Once both these clips are destroyed, the outer plastic shell (Figure 1M) should slide off the orange needle sheath, which will come out attached to the syringe. There are 2 orange arms that extend off the needle sheath (Figure 1D) and attached to the white plastic housing behind the syringe (Figure 1K). Pry these 2 orange arms apart to unclip them and remove the orange sheath. Caution will need to be taken here and for further steps as there will be an exposed used needle.
Measurement and Dispensing Medication From the Syringe (Figure 2H and I)
Now that the needle and syringe are exposed, draw 3 lines on the plastic syringe to divide the remaining doses into quarters, which should be approximately 0.3 mL (0.3 mg) of epinephrine (Figure 2F). Previously studied autoinjectors allowed for drawing up air into the syringe to measure and dispense additional doses; however, due to the plunger shaft not being attached to the rubber plunger stopper, that method is not possible with this type of autoinjector.
The next step is to remove the white plastic housing, which is spring loaded (Figure 1K). A firm grasp on the syringe is necessary to prevent the needle end becoming projectile. A second person can make this easier and safer. There are 2 white clips that attach the spring-loaded end to the clear plastic syringe. By prying these 2 clips apart with your hands, the spring and white end will forcefully spring off the syringe (Figure 2G).
The remaining doses are not clearly marked or measured on the syringe. This can be done by marking the outside of the syringe into 4 equal parts prior to administration of subsequent doses. This may be performed with a marker or by scratching indentations into the side of the syringe (Figure 2F).
The shaft of the plunger (Figure 1H) has been crafted such that it cannot be further advanced into the syringe (Figure 1G) to dispense more doses. The rubber plunger seal is not attached to the plunger shaft, so air cannot be drawn up into the syringe to assist with dispensing additional doses (Figure 2H). The user will have to find a long, narrow object with a diameter of ≤0.5 cm and a length of at least 6.5 cm, such as a screwdriver, piece of stiff wire, or stick, to push the plunger farther to dispense additional doses (Figure 2I). This object will not come in contact with the sterile medication fluid and will only be used to advance the rubber plunger, which maintains a sterile barrier between the object and medication. The exposed needle can be stored in the yellow end cap that was removed during initial administration for rescuer safety and to prevent contamination between administrations Figure 3.

Storage of exposed needle in the end cap of the epinephrine autoinjector.
The above method was found to be the quickest, most reliable way of retrieving additional doses of epinephrine from the Teva epinephrine autoinjector. Although this method requires prior knowledge and practice, it can be done in under 3 to 5 minutes, which should allow additional doses to be dispensed in the appropriate amount of time.
Discussion
This study was performed only on the Teva brand of autoinjectors. As new brands and designs of epinephrine autoinjectors are developed and released, this will warrant further research in the future.
An important consideration when attempting this process is that like some previously studied autoinjectors, 9 there will be an exposed needle while preparing further doses. This will require extra care and awareness to prevent damage or contamination of the needle. There is also a heightened risk of needle-stick injury.
The autoinjectors studied included approximately 4 extra 0.3-mg doses of epinephrine, giving the user up to 5 doses in total. Standard epinephrine dosing is 0.3 to 0.5 mg. The first dose of epinephrine administered by the autoinjector is premeasured and allows for rapid administration. The protected plunger in this model of autoinjector requires a tool or object to depress the rubber stopper in order to administer additional doses of epinephrine. This makes exact administration more difficult and requires some creativity on the part of the person performing this process. This may limit the accuracy of dispensing subsequent doses. This method of estimating additional doses is imprecise, and the amount of remaining medication may vary slightly among autoinjectors; however, standard epinephrine dosing has a varied range, and some variation in precision on dosing autoinjectors is already accepted. Additionally, the optimal dose of epinephrine is unknown. 5 Dose precision is less important than delivering some amount of life-saving medication for anaphylaxis.
Retrieval of additional doses from this particular brand of autoinjector required more tools when compared to those used with previously documented examples. Thus, it requires prior knowledge to safely and confidently access the extra doses of medication.
A multitool pocket knife was used as such tools are common in the backcountry. Previous literature addressed accessing epinephrine from autoinjectors using similar tools. 8 The 2 main components used were a can opener (which acted as a pry bar) and the blade of a knife, which was used to “drill out” 2 small plastic tabs on the side of the device (Figure 2E). Any flat, strong tool that is narrow enough to fit under the plastic tabs could be used for prying the outer shell, such as a flat-head screwdriver or strong knife blade. Drilling out the small plastic tabs could be achieved with anything sharp that can be rotated, with a knife blade being the most efficient choice.
The recommendation to carry vials of epinephrine is likely to be made when discussing the difficulties of access through destruction of an autoinjector. Vials would allow access to multiple doses of epinephrine and are typically much cheaper than the autoinjector. However, a benefit of the autoinjector is that it is an easy-to-use, self-contained device that has both the needle and medication already prepared. On the other hand, glass ampules are more prone to breaking, and needles would need to be kept in the same kit and be accessible. One method of carrying and administering epinephrine is not recommended over another; however, these considerations need to be balanced when making this decision for personal use or for an expedition. Additionally, medical personnel may come across a patient who carries one of these epinephrine autoinjectors for personal use and may need to be assisted with retrieval of additional doses.
This study was meant to explore the process of acquiring extra doses from these new Teva epinephrine autoinjectors. The process demonstrated in this study was the result of multiple practice runs, resulting in the complete destruction of 3 autoinjectors, and a review of patents to understand the mechanics of the device. This trial and error would not be a process easily performed in a wilderness or austere setting. Practice of this method prior to use in the field would be beneficial. While access to additional medication to treat anaphylaxis in the backcountry is beneficial, even when obtained correctly and all 5 doses of epinephrine are available, evacuation to a higher level of care is still recommended.
Conclusion
Anaphylaxis is a life-threatening condition, with the first-line treatment being epinephrine. This study documents a novel approach to extracting epinephrine from the Teva autoinjector in field environments. This allows an additional 4 doses of epinephrine, which may be life saving in the case of refractory anaphylaxis or a biphasic reaction. In a wilderness setting, this may be the only option due to prolonged extrication or distance to definitive care. We recommend practicing this method prior to field use.
Footnotes
Acknowledgements
Author Contributions: All authors conceived of the study, performed the investigation, created videos and images, drafted the manuscript, as well as reviewed, edited, and approved the final manuscript.
Financial/Material Support: None.
Disclosures: None.
Supplemental Material(s)
Supplementary material associated with this article can be found in the online version at