
Abstract
Introduction
Foot-launched flying sports such as paragliding, hang gliding, and speedflying are popular recreational activities that all pose a significant risk of accidents resulting in injuries or fatalities. We describe the epidemiology, incident circumstances, and findings of forensic examinations of fatalities in these sports.
Methods
In this retrospective analysis, we analyzed different parameters of paragliding, hang gliding, and speedflying fatalities in the canton of Berne, Switzerland, between 2000 and 2018. The data sources were police reports, forensic medical reports, the Swiss Hang Gliding Association, and the Swiss Council for Accident Prevention.
Results
In the given period, 40 incidents resulting in 42 fatalities were recorded (2 incidents involved 2-seaters). Three of the 40 incidents did not fulfill the inclusion criteria and were excluded. The deadliest phase was midflight. Collapse of the glider (n=9; 36%) was the leading cause of accidents among paraglider pilots. Multiple trauma (n=21; 54%) was the most frequent cause of death. In the forensic examination, all deaths (n=39) were assessed as accidents.
Conclusions
The different categories of foot-launched flying sports varied in the causes of accidents and deaths. Fatalities in speedflying involved young pilots exposing themselves to high-risk situations. Fatalities may be prevented by enhancing education and training and promoting a cautious attitude among pilots.
Introduction
Foot-launched flying sports are popular activities in both the alpine and flat regions of Switzerland. The Swiss Hang Gliding Association (Schweizerischer Hängegleiter-Verband, SHV) was founded in 1974, soon after the first hang glider flight in Switzerland. The SHV is an association that coordinates flight training, conducts pilot examinations on behalf of the federal office of civil aviation, and promotes the interests of pilots. In 2018, the SHV had 16,798 members and included all foot-launched flying sports.
1
The SHV divides these sports into the following categories: paraglider, miniwing, hang glider, powered paraglider/hang glider, fixed-wing aircraft, and speedflyer. Each category requires a specific license. The paraglider license includes the miniwing and speedflyer, with the latter requiring an additional license. Miniwings (14–20 m2) and speedflyers (<14 m2) are smaller than paragliders (>20 m2). Speedflyers reach velocities up to 120 km·h-1 (
Based on a survey of 30,000 Swiss citizens, the Swiss Council for Accident Prevention (SCAP) estimated that 810 Swiss paragliders and 180 Swiss participants in other flying sports (hang gliding, powered paraglider/hang gliding, speedflying, flying a fixed wing aircraft, base-jumping, and skydiving) have an accident each year.
3
In the period of 2000 to 2017, 158 people died in Switzerland while flying a foot-launched glider (
Because the literature is sparse and not up to date, it is important to report on the epidemiological data to enable further research and develop safety measures. 5 The previously cited 2017 article was the first and only one to separate speedflying from paragliding. 5 The distinction of the different categories is important because each sport requires unique flight techniques and specific equipment and involves category-associated risk factors. Our aim was to investigate the epidemiology, circumstances of death, and forensic examination results of foot-launched flying sport fatalities.
Methods
We performed a retrospective analysis of fatalities that occurred between 2000 and 2018 during foot-launched flying sports in the large mountainous canton of Berne, which is 1 of 26 cantons in Switzerland. Paragliding, hang gliding, speedflying, fixed-wing aircraft, and miniwing categories were investigated. Fixed-wing aircraft fatalities were added to hang gliding owing to the shared flight techniques and common risk factors of the 2 aircraft types. The Institute of Legal Medicine of the University of Bern registered the date and location of the fatalities successively after they occurred. The SHV and SCAP also registered and reported the fatalities independently. The cases from these 3 sources were matched and verified using the files of the responsible public prosecutors’ offices (Jura-Lakeland, Emmental-Oberaargau, Midland, and Highland). The crucial source of data for our study was the files of the public prosecutors’ offices, including forensic (external inspection, autopsy, and toxicology testing), police (testimonies, photographic and cartographic documentation with the exact coordinates of the incident sites, photographic documentation of the gliders, and avionic data), and medical reports.
The following parameters of interest were extracted from the files for analysis: general epidemiological data, cause of death, results of the toxicology testing, causes of the incident, equipment (including paraglider difficulty classes), the pilot’s experience, and environmental factors. The paraglider difficulty classification ranged from the easy European Norm A to the difficult European Norm D classes.
We classified the weather conditions as follows: unproblematic (calm weather, normal or good conditions), problematic (gusty winds or strong winds [>25 km·h-1], increased turbulence, or fog in the flying area), and insufficient for classification (nonpilot witnesses or unknown). Nonpilot witnesses were not taken into account for evaluation of the weather conditions because they are inexperienced in assessing flight-specific weather.
Because of the importance of the files in our study, cases were excluded if their files were not found in the responsible public prosecutors’ offices.
Data were entered into Microsoft Excel before analysis. They are presented as mean±SD for continuous variables and percentages and are rounded to the nearest whole number for the categorical variables, if the denominator was greater than 9.
We investigated reports that included the results of an official case investigation conducted by the responsible department of public prosecution that owns the data. The files are publicly available for research purposes if the use is authorized by the department of public prosecution. The written request to use the files for this study was approved by the responsible public prosecutor’s office.
Results
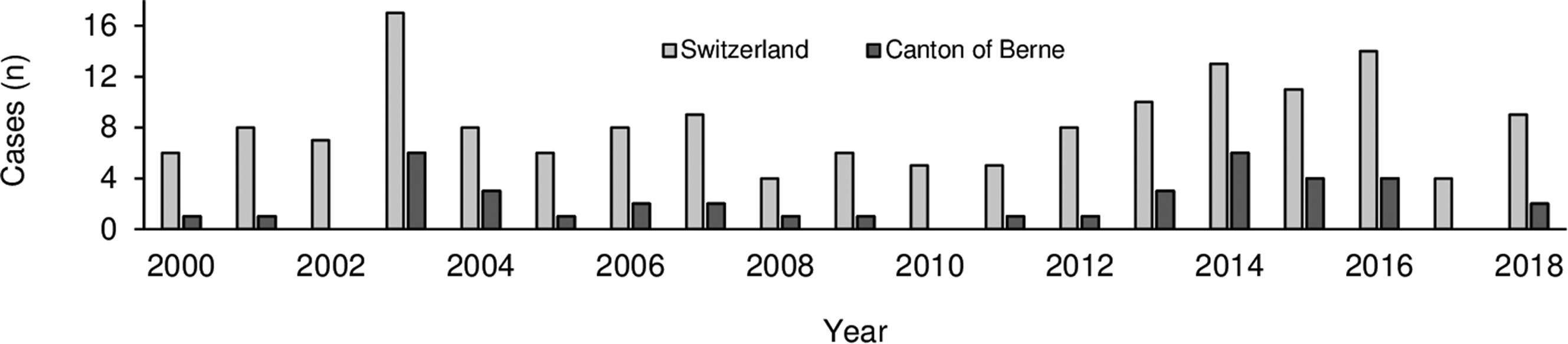
The number of cases registered in our institute corresponded to the number of cases registered by the SCAP and SHV. Forty-two fatalities occurred in all foot-launched flying sporting activities during the study period. Three files for these confirmed cases were not found in the public prosecutors’ offices and were excluded from further analysis. Consequently, the given results include 39 fatalities in 37 cases (4 people died in 2 tandem paragliding accidents). Paragliding accounted for 27 (69%), speedflying for 7 (18%), and hang gliding for 5 (13%) fatalities. No cases involving miniwings or powered paragliders/hang gliders were recorded. Therefore, 3 categories are shown: paragliding (P), hang gliding (H), and speedflying (S). The annual number of fatalities in the canton of Berne, as well as nationwide data, from 2000 through 2018 are shown in Figure 1. Speedflying information was included in the database from the beginning of 2008.
Annual number of fatalities in Switzerland (
The epidemiological results show that only 1 fatality with a female pilot (3%) was reported (hang gliding). The 2 other females were passengers in tandem paragliders. Table 1 and Figure 2 show the epidemiological results. The glider-specific age distribution shows the predominantly young age of the speedflyers.
Epidemiological data, absolute and relative numbers
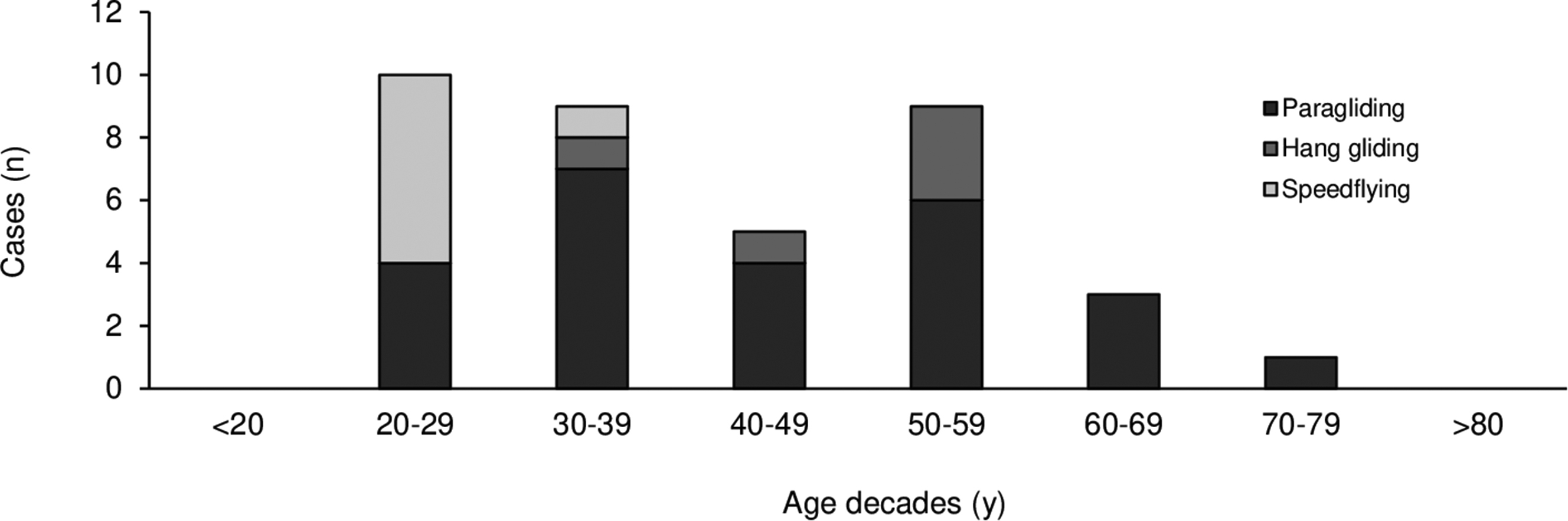
Number of fatalities for the different age decades.
Table 2 shows the accident circumstances. Most of the 37 accidents occurred midflight, followed by take-off and landing. After successful take-off, 17 accidents (65%) occurred in the first 10 min of the flight. The accident happened after more than 1 h in only 1 case. The 2 incomplete preflight checks indicated in Table 2 were due to insufficiently closed harnesses with open leg belts, causing a fall out of the harness. Equipment failure was not blamed for any fatal accidents; however, in 1 case improper maintenance of the equipment resulted in death. In this case, a test pilot shortened the paraglider’s lines using knots and placed them incorrectly. As a consequence, the lines were destabilized, and they all ripped during a spiral dive. For 28 victims (72%; 17P, 4H, 7S), the use of a helmet was verified in the documents. For the other cases, no information on helmet-wearing was available. As shown in Table 3, the rescue parachute was deployed in only 5 of 23 possible situations (22%; 5P), and in only 1 case (4%; 1P) was the parachute able to fully deploy. This pilot had a nonsteerable rescue parachute. He was unable to avoid collision with a rock face and fell to his death. In 12 cases, the height above the ground was ≤100 m for the event causing the accident.
Accident circumstances; collision with objects includes objects on the ground and in the air
Rescue parachute use, pilot experience, and environmental parameters
Note that in the cases in which the rescue parachute status was unknown, use of it was impossible.
“Event” refers to the altitude where the problem started to develop. In the cases of take-off errors, the altitude of the launch site is indicated.
Figure 3 shows the distribution of fatalities for different glider difficulties. The proportion of glider-associated fatalities was higher among more demanding paragliders. Additionally, 2 aerobatic (5%), 2 tandem (5%), and 1 unknown paraglider (3%) were reported.
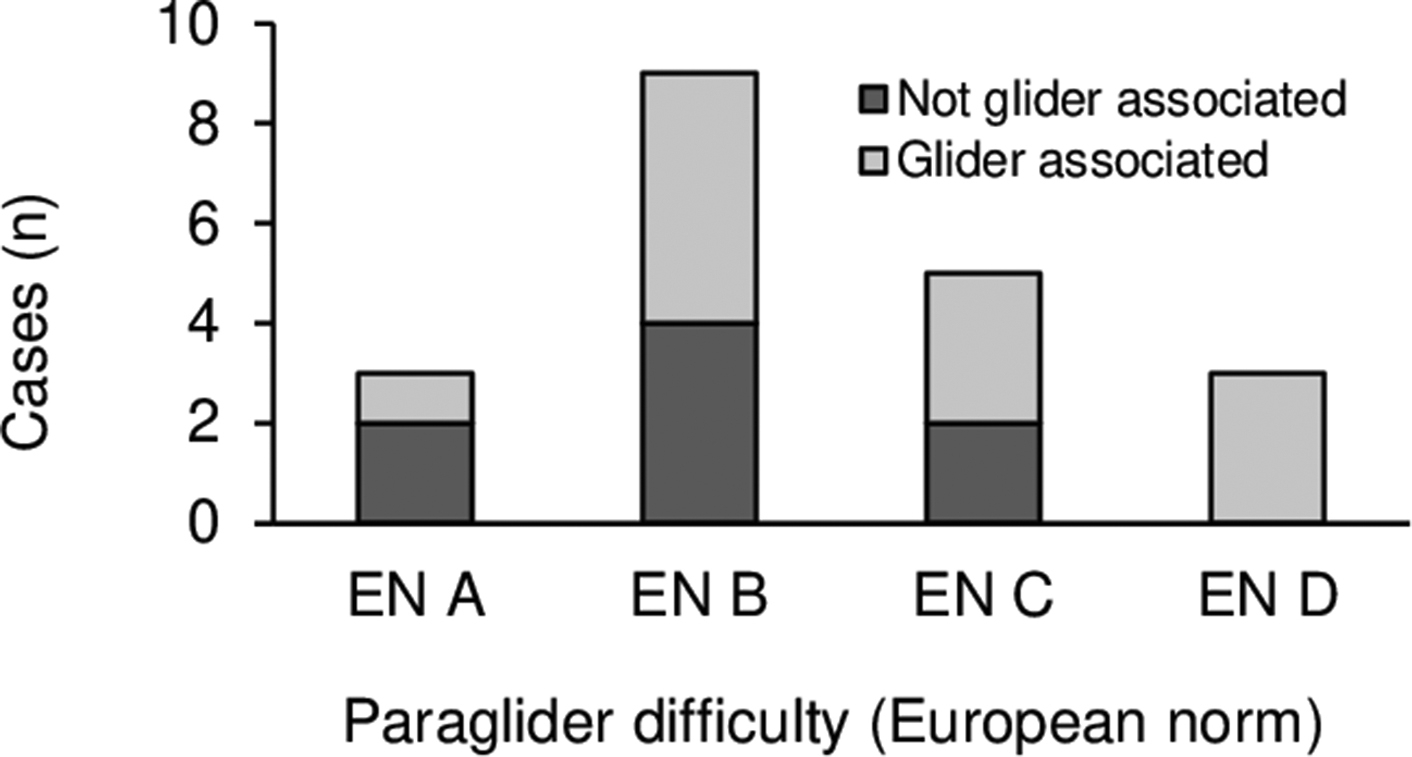
Number of fatalities and association with different glider difficulties in paragliding. Not glider-associated: incomplete preflight check, collisions; glider-associated: take-off errors, collapses, oversteering, spiral dive.
Data regarding the years of experience and number of flights were rare and mostly incomplete. Table 3 shows the available data on the pilots’ experience. Five of 7 speedflyer pilots had held their license for ≤2 y. Because the literature on speedflying is scant, a short description of all speedflying fatalities is listed in Table 4.
Event description and assumed causes of fatal speedflying accidents
Data on the environment are presented in Table 3. In 2 cases, the altitude of the accidents was >4000 m above mean sea level (4100 m and 4080 m, 5%; 1P, 1S, respectively). In both cases, take-off errors occurred after climbing the summit of a mountain. Three of the 6 cases from 2500 m to 4000 m (16%; 4P, 2S) were also caused by take-off errors. These alpine take-offs were characterized by ice, firn, and rocks. All of the speedflying fatalities occurred in the 15-km-long Lauterbrunnen valley.
When an event occurred during the flight (n=22), the altitude above ground was 0 to 50 m in 4 cases (18%; 2P, 1H, 1S), 50 to 100 m in 8 cases (36%; 6P, 1H, 1S);=, and over 150 m in 7 cases (32%; 7P). In 3 of 22 cases, this information was not provided. Take-off and landing errors, direct collisions with the ground, and unclosed harnesses were excluded, resulting in 22 cases.
The medical data and forensic examinations revealed that autopsies were performed for only 10 victims (26%) and revealed pre-existing medical conditions in 3 cases (30%): 1) atheromatosis, 2) coronary heart disease and pulmonary emphysema, and 3) atheromatosis and atherosclerosis. For the individual with the coronary heart disease, the report discussed whether this finding could have been relevant as the cause of the incident. The most likely cause of death for each victim, obtained from an external inspection and rarely from autopsy, is listed in Table 5. In 1 case, the manner of death was initially considered suicide because the pilot did not close the harness correctly. However, witnesses reported later that the pilot fought for his life, holding onto the harness. Therefore, the case was finally assessed as an accident. Consequently, all incidents were thus assessed as accidents. One person (3%; 1P) was conscious, and resuscitation was not necessary when found. The death, due to cerebrocranial trauma, occurred the same day after admission to the hospital.
Forensic examination and toxicological analysis, absolute and relative numbers
CCT, craniocerebral trauma.
Discussion
The number of foot-launched flying sport fatalities registered at our institute, SCAP, and with SHV were congruent. Therefore, it can be assumed that most cases in the area being studied were known. Three cases were excluded because the corresponding files were not available. The SCAP had 16,798 members nationwide at the end of 2018; however, once a license has been obtained, it is not mandatory to be an SHV member. 1 Because the exact number of active pilots and the number of accidents in the canton of Berne itself are unknown, it was not possible to calculate mortality rates. Among the British Hang Gliding and Paragliding Association, member fatality rates (fatalities per 100,000 participants per year) of 40 from hang gliding and 47 from paragliding were reported; the rates for speedflying were not available. 5
The distribution of fatal accidents over the years in the canton of Berne and throughout Switzerland showed a similar dynamic (Figure 1). Although the absolute numbers did not increase, the number of active pilots and nonfatal accidents increased1,3 (
The sex distribution in this study (92% male, 8% female) showed a slightly higher proportion of males than in other studies. In Austria, 86% were male and 14% female, and in Great Britain, 88% were male, 9% female, and 3% unknown.5,6 Both studies included fatal and nonfatal accidents. The relative risk of crashing was found to be higher in females. 6 The rates for deadly accidents for each sex could not be calculated because the SHV does not record members’ sex.
Detailed analyses of nonfatal accidents have shown that the midflight 6 or landing7,8 phases are the 2 most dangerous phases of the flight in terms of the absolute numbers of accidents. In Switzerland, between 2011 and 2017, the landing phase resulted in most of the nonfatal accidents, mostly followed by the take-off phase. 9 -15 Our study found that most fatal accidents in the canton of Berne occurred midflight, followed by the take-off phase. The transformation of the higher potential energy during the take-off and mid-flight phases to kinetic energy during a fall could be the reason for the more severe impact. In contrast, rough landings, especially in difficult terrain, 7 tend to result in lower extremity and spinal injuries. 8
Table 2 shows certain category-specific differences for the causes of the accidents. Glider collapse was the most frequent cause of fatal accidents in this study (24% of all cases, 36% of all paragliders). In 409 consecutive paragliding accidents in Germany, the collapse of the canopy was the most reported cause of accidents (33%). Although the rigid wing of hang gliders protects them from collapse, they are more at risk during the take-off phase. Owing to their size and weight, or rather the principle of inertia, a take-off abort is usually not possible, with take-off failure being potentially fatal.
It has been said that a long flight can be compared with a long car drive 16 and can cause mental exhaustion. 17 The duration of the flights (only 1 case >1 h) did not suggest that long flights led to fatalities. Thus, mental exhaustion is unlikely to have played a role.
Equipment failure was not blamed for any fatalities in our study. Other studies also reported that equipment failure was a rare cause of accidents (1%, n=405; 3%, n=2037).6,18 However, quality, approved, and presumably safe equipment was reported to be important for paragliding pilots.
19
The rates of helmet use and the installation of rescue parachutes (both 100% considering only the cases with known status) among the fatalities in this study show their importance for pilots in Switzerland. In comparison, the SCAP reported that only 16% of skiers and snowboarders wore helmets in the 2002 to 2003 winter season in Switzerland. This, however, increased consistently to 92% in the winter season of 2015 to 2016 (
Although the rescue parachute installation rate was 100%, the pilots rarely used the parachute. Of 24 cases, only 5 pilots pulled their parachutes, and only 1 succeeded in fully deploying the parachute. The low percentage of use could be due to a lack of emergency training, in which the practice of pulling the rescue parachute becomes a reflex action. The low altitude aggravated the situation. In 12 cases, the event that led to the accident happened at <100 m above the ground, which is usually not sufficient to use a rescue parachute. A free fall of 100 m with g=9.81 m·s-1 takes 4.5 s. After deciding to use the rescue parachute, it takes 4 s to find the handle, grab it, pull it, throw it, and let the parachute fully deploy. 20 The isolated opening time of a new rescue parachute is approximately 1 s (from throw to full deployment). 20 The low altitude and the rare use of the rescue parachute led us to make 2 recommendations: repeating safety courses and ensuring a sufficient distance from the ground and the slope.
The increasing proportion of glider-associated accidents, with an increase in glider difficulty (Figure 3), supports the warnings of the SHV, flight schools, and manufacturers that high-end gliders can become out of control more easily. 9 -15 Experienced pilots have fewer accidents during the take-off phase compared with beginners; however, a large number of accidents resulting from collapse occurred among experienced pilots. 18 A potential explanation for the discrepancy between the take-off and the mid-flight phase events might be equipment choice, if experienced pilots tend to choose more demanding gliders. It has also been suggested that experienced pilots take more risks. 21
Data regarding pilot experience were rarely reported. Focusing on experience among speedflyer pilots, 5 of 7 died within the first 2 y after receiving their license. The first 2 y after gaining a license are the most accident prone, irrespective of the number of completed flights. 18 This is despite speedflyers already requiring a paragliding license before speedflying training. Experience appeared to decrease the risk of some types of mishaps5,7 while increasing the risks of others.7,21 To reduce accidents, all pilots should strictly maintain use of the recommended checklists to avoid preventable mistakes and should take care in glider selection. 20
Bad weather conditions or weather changes are often described as risk factors6,7,18,22 and play a contributing role in up to 33% of all accidents, 23 becoming risk factors for deadly accidents. For base jumping, the environmental factors linked to fatal accidents were mostly a result of poor decision making. 24 Although 5 of 6 fatalities in bad weather conditions were thought to have been provoked by these conditions, most of the fatalities (59%) occurred in unproblematic weather conditions.
The famous Lauterbrunnen Valley attracts speedflyer pilots, and a similar aggregation is seen in base jumping. The base jumping fatality list compiled by BLiNC magazine, a community base jumping website, reported that 51 (56%) of 91 fatalities in Switzerland between 1994 and 2019 occurred in the Lauterbrunnen Valley. The popular region allows up to 10 base jumps per day, leading to a multiplication of the absolute risk. 24 The circumstances of speedflying fatalities in this challenging region show that these pilots tend to expose themselves to high-risk situations, either through the use of demanding and dangerous launch sites or through proximity flying.
The elevation exposure during the accident in 8 cases was between 2500 and 4100 m above mean sea level, referred to as moderate altitude.
25
These altitudes are potentially sufficient for some degree of hypoxia or even high altitude illness.
25
-27 A systematic review suggested that hypobaric hypoxia at moderate altitudes may lead to cognitive and psychomotor deficits in learning, reaction times, decision-making, and certain types of memory.
25
However, the results at moderate altitude were inconsistent,
25
with reported thresholds for cognitive deficits ranging from 1525 m when exercising to 4572 m at rest.28,29 There has been shown to be an increase in reaction time during exercise (80% peak oxygen consumption, 

The medical and forensic data showed a high proportion of cases (54%) without any medical interventions. This suggests that the victims sustained from severe injuries from the accident. The causes of death listed in Table 5 underline this suggestion on the basis of a high proportion of multiple trauma (54%). The literature is consistent about the fact that foot-launched flying sports accidents are often severe.7,22 Hang gliding pilots seem to be more prone to head and neck injuries and tend to die from cerebrocranial trauma. Other studies have shown that hang gliding pilots are more likely to experience head and neck injuries than pilots in the other categories.5,6 The high proportion of external-only inspections (74%) without autopsy did not reveal the exact cause of death, as would be expected from autopsies. Therefore, we are not able to discuss the importance of traumatic aortic rupture as a hidden and missed injury, as described in the literature.13,31,32
In comparison with a case of suicide, in which a skydiver manipulated his rescue system, 33 suicidal intentions were suggested in only 1 case with an unclosed harness. The suicide suggestion was ruled out later by witness testimony. In 1 case in which an autopsy was done, the accident mechanism showed the involvement of pre-existing medical conditions (coronary heart disease and pulmonary emphysema). In this case, the 64-y-old pilot flew without any steering impulses into a cliff. A case series also suggested that 1 of 6 skydivers who were autopsied could have lost consciousness owing the presence of coronary heart disease, outflow obstruction, and myocardial hypertrophy and may therefore have not opened the parachute. 34 However, there was no evidence of the influence of pre-existing medical conditions on the accidents. Therefore, because there is seldom danger to others, we do not recommend compulsory medical certificates, as is done in general aviation. An increased number of autopsies could help to give better-founded recommendations, in this regard.
To fully understand the causes and dynamics of foot-launched flying fatalities, a detailed examination of these cases is required.
Limitations
Data were gathered for nonresearch purposes by rescue teams, the police, and forensic doctors, and mostly without specific knowledge of foot-launched flying sports. Most of the causes of death were determined only by external inspection. Therefore, the medical results must be evaluated with caution and are only listed as the most probable cause of death. Records of pre-existing medical conditions and prescribed drugs were rare. Consequently, the data were incomplete, contained obvious assumptions, and included witness testimony. Nonpilot observations need to be assessed critically owing to possible misinterpretations.
The low number of accidents involving fatalities between 2000 and 2018, missing files, and the retrospective method used limited the value of the general statements about foot-launched flying sport fatalities.
The accidents occurred within a period of 20 y. The temporal dynamics, technical developments, adaptations of the education system, and other new security measures were not taken into consideration and may therefore have created a bias. Because the literature was sparse and not up to date, it was difficult to make comparisons with the results of this study.
Conclusions
The categories of foot-launched flying sports differed in the causes of accidents and causes of death. The causes of death appeared to be traumatic in nature, and all incidents were categorized as accidents. The deceased speedflying pilots were on average 18 to 23 y younger than the paraglider/hang glider pilots and often died in high-risk situations. High altitude take-off sites, incomplete or missing preflight checks, flying close to the slope, and use of demanding gliders were identified as potential risk factors. We see prevention possibilities in education and training, the implementation of preflight checklists, and familiarizing pilots with the technique of throwing the rescue parachute. We recommend that all pilots fly and choose their glider cautiously, considering their experience and their flying skills.
Footnotes
Acknowledgements
Acknowledgments: We thank the public prosecutors’ offices of the canton of Berne, Switzerland, for providing the investigation reports and the Swiss Hang Gliding Association for providing the data.
Author Contributions: Design of the study (FS, CS); acquisition of the data (FS, CS); analysis of the data (FS); interpretation of the data (FS, CS); drafting of the manuscript (FS); critical revision of the article; approval of the final manuscript (FS, CS, CJ).
Financial/Material Support: None.
Disclosures: None.