
Abstract
Encounters between marine animals and humans can result in critical injury and fatal complications. We highlight a 20-y-old male who sustained a penetrating injury to the neck as a result of impalement by needlefish (Tylosurus sp) while snorkeling. He sustained a penetrating injury in the posterior triangle of the neck. On presentation, he was stabilized and received empirical antibiotics, analgesia, and antitetanus toxoid injection before being transferred to a tertiary center. On presentation to the tertiary hospital, the patient was hemodynamically stable with no clinical evidence of injury to surrounding neck structures, and this was confirmed using computed tomography. The patient underwent local wound exploration and retrieval of the needlefish beak under general anesthesia. The wound was left open to heal by secondary intention. The patient was discharged with oral antibiotics and went on to make a complete recovery.
Introduction
Injury caused by marine animals is usually unexpected. Despite the need for fishing or social activities among the local population and travelers, marine ventures can be life-threatening, especially in tropical and subtropical countries. Activities such as windsurfing, kite surfing, swimming, and diving can result in injury owing to contact with marine animals.1,2 Stingrays and stonefish can cause direct trauma and envenomation, but there are also infrequent cases of injury by needlefish and swordfish species. 3 Although infrequent, an encounter with these fish can result in critical injury and even fatal complications.4,5 We present a case of injury to the posterior triangle of the neck after needlefish impalement and discuss our management approach.
Case Report
A 20-y-old Maldivian male presented to a tertiary care center 4 h after being impaled by a needlefish while snorkeling in the evening. The patient had sustained a penetrating injury to the right side of the neck (Figure 1) with local swelling and ecchymosis. On presentation, he was hemodynamically stable with a pulse of 75 beats·min-1 and blood pressure of 120/70 mm Hg. There was no evidence of vascular injury, such as pulsatile bleeding, arterial thrill, or rapidly expanding hematoma. After initial assessment and hemodynamic stabilization by the local clinic, the patient was given ceftriaxone and metronidazole empirically, along with analgesia and antitetanus toxoid (ATT) injection. He was then referred to the tertiary center for definitive management. The results of laboratory investigations, especially renal profile and liver function tests, were unremarkable. Chest radiography (Figure 2) revealed an elongated hyperdense foreign body, which was confirmed using computed tomography (CT) scan. The CT imaging revealed a 3-cm foreign body (Figure 3A) that avoided vital neck structures (Figure 3B).

After impalement, the body of the fish separated from the beak, which was retained in the wound. The wound entry was noted at the posterior triangle and zone II of the neck.
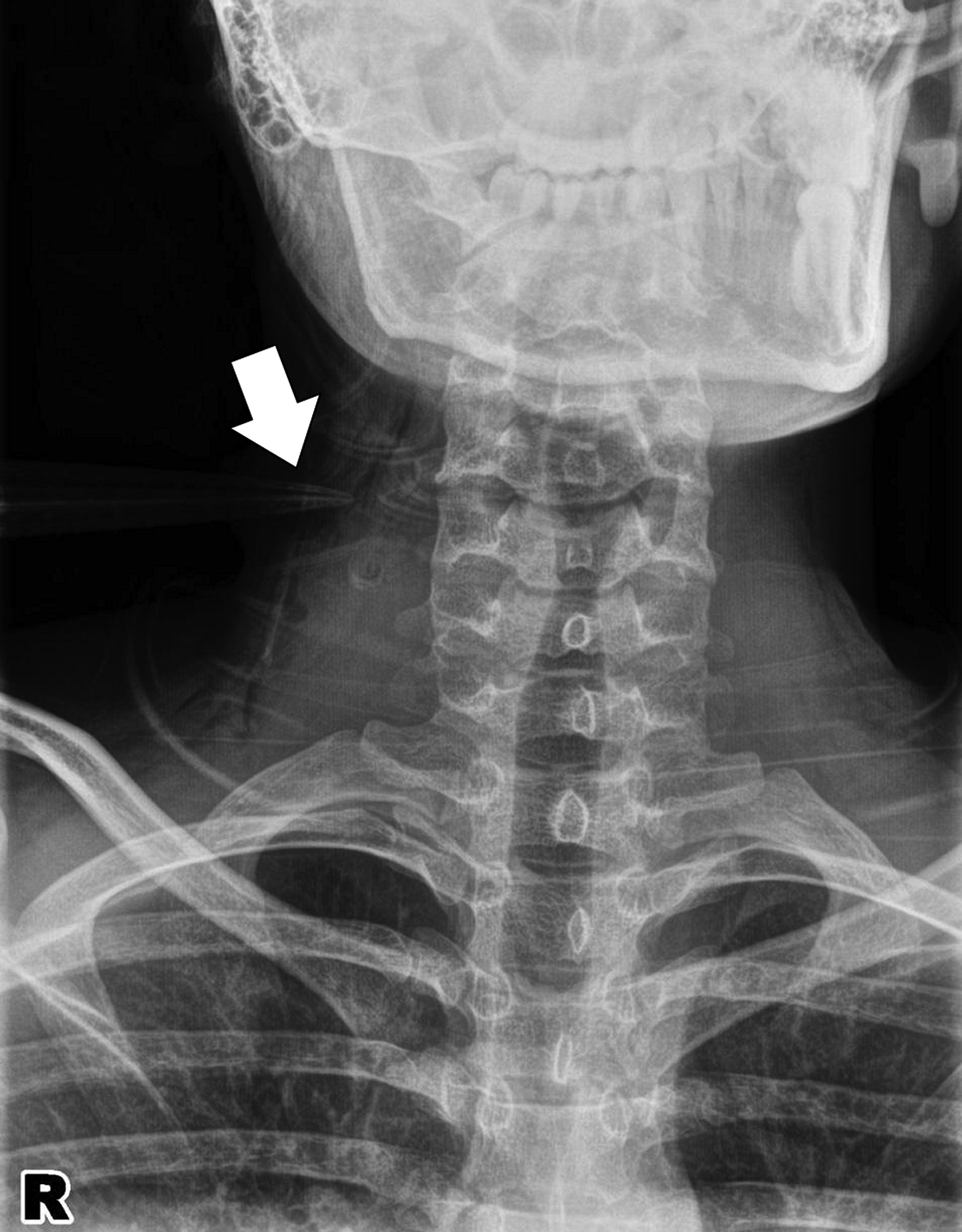
Chest radiograph revealed a sharp, elongated, radiopaque structure (white arrow) at the right lateral neck.
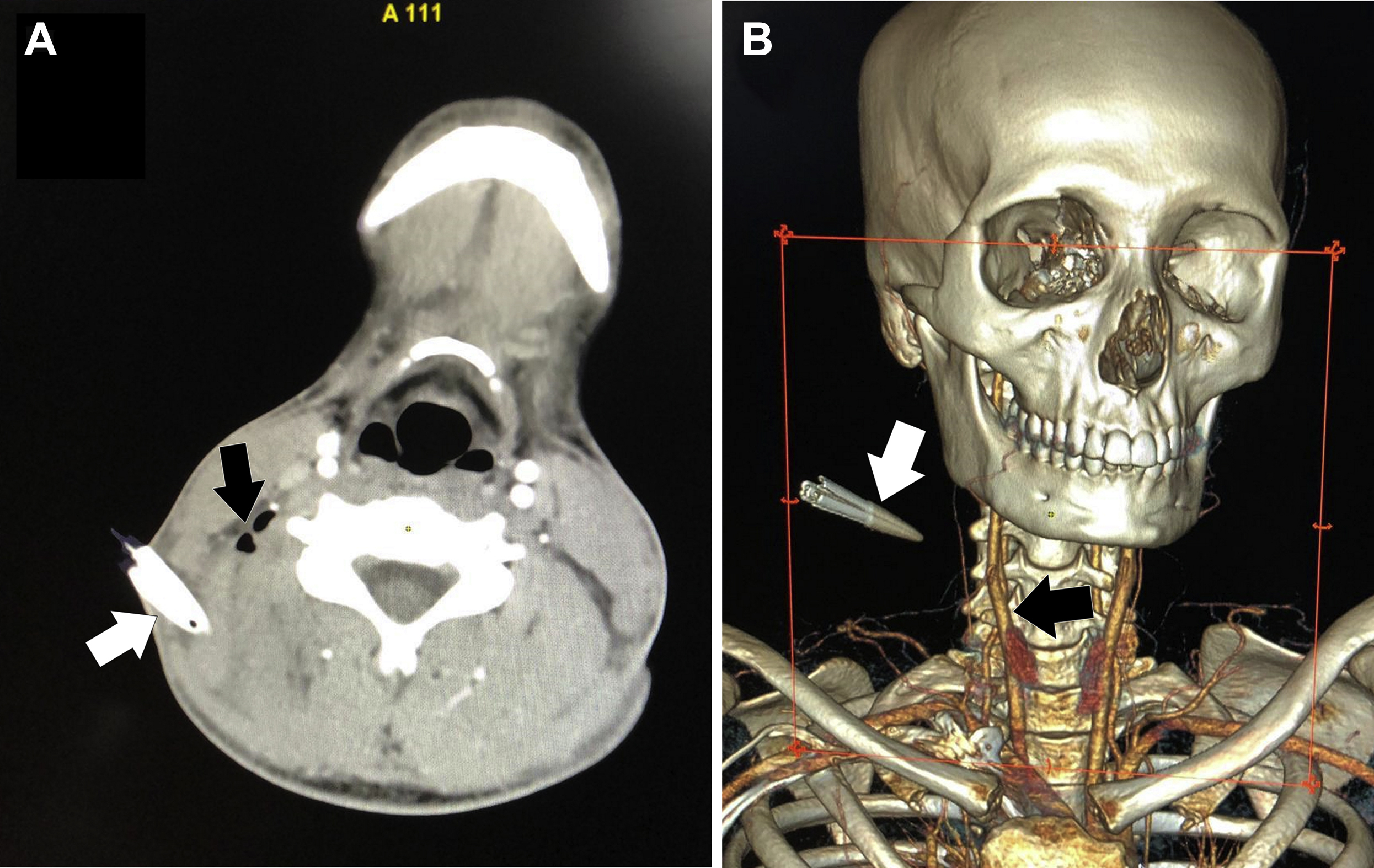
(A) An axial computed tomography angiogram image revealing a hypodense structure (white arrow) measuring 3 × 1 cm, representing the retained beak of the needlefish penetrating beyond the deep cervical fascia with the presence of air (black arrow). (B) A 3D reconstruction revealing the elongated foreign body (white arrow) 6 cm from the carotid vessels (black arrow).
Upon confirmation that no major structures were involved, the patient was taken to the operation theater for wound exploration under general anesthesia. Intraoperative findings (Figure 4A) revealed a 3-cm-long oblique penetrating wound tract on the lateral aspect of the right side of the neck. The intact needlefish jaw was extracted (Figure 4B), and the wound was copiously irrigated with saline. The surgery was completed without complication, and the wound was left open to allow healing by secondary intention given the possibility of retained foreign body and infection. The recovery period was uneventful, as expected, and the patient was discharged home the next day with oral antibiotics (cefuroxime and metronidazole) and analgesia. He was prescribed Algicel Ag dressing changes every other day.
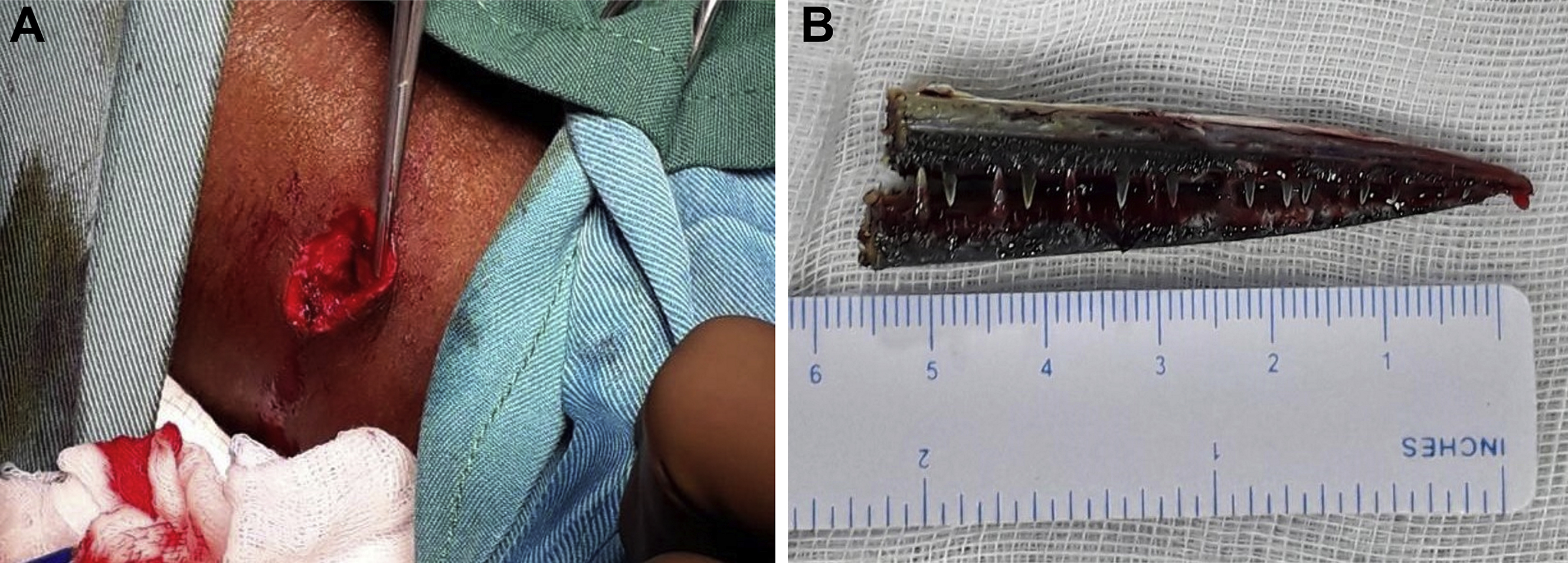
(A) Wound exploration and irrigation. The entry wound measured 1 × 0.5 cm and 3 cm in depth. (B) The needlefish beak was retrieved in a complete form measuring 6 cm in length.
Discussion
Needlefish are silver in color with an elongated body and are tubular in shape, ranging from small to medium size; most needlefish are usually between 3 and 95 cm. 6 Needlefish have a characteristic narrow, pointed jaw with numerous sharp teeth. They belong to the family Belonidae and order Beloniformes. 6 Usually, needlefish swim near the surface; however, if they are startled, frightened, or attracted to bright light, especially at night, they may leap from the water or skip on the surface. They are capable of making short jumps out of the water at up to 65 km·h-1 (40 mph). 6 With high velocity, their sharp beaks can spear swimmers, divers, or fishermen, inflicting deep puncture wounds.4,5 In our case, the type of fish was identified based on visual confirmation by the patient and local bystanders who brought him to the hospital. We did not send for DNA testing because it was unnecessary at the time and a biologist was not available for visual identification.
Injury severity depends on the organs involved. Given the nature of penetrating wounds, the entry point may appear deceptive compared to the underlying injuries it has caused. Injuries from needlefish to the limb, abdomen, and even face have been commonly reported within the literature.1,2,4,5,7,8 However, there are infrequently reported cases involving the neck.9,10 To date, there are only 2 other reported cases involving the neck; however, this type of injury has the potential to be fatal. This case is important because it highlights the management of a marine penetrating injury to the neck and key considerations to be made (Table 1).
Traumatic neck injury caused by needlefish
ATT, antitoxoid therapy; CT, computed tomography.
Management of all penetrating injuries should begin with advanced trauma life support. 11 It may be challenging in a remote area and may require transfer to a higher center of care capable of advanced imaging and surgical intervention, as happened in our case. 12 Penetrating wounds to the neck may injure the vital structures such as the vessels, nerves, trachea, and esophagus, depending on the zone of injury (Figure 5).13,14 In this case, the patient sustained an injury in zone II, which lies between the angle of the mandible and the border of the cricoid cartilage, in which injury to the carotid arteries and its branches, as well as the jugular veins, can be life-threatening. 13 The cartilaginous laryngeal skeleton and tracheal injury are difficult to repair but can induce rapidly developed subcutaneous emphysema, which sometimes can lead to fatal outcomes. 15 Injury to the abdomen and thorax can lead to the involvement of visceral organs and their blood supply.
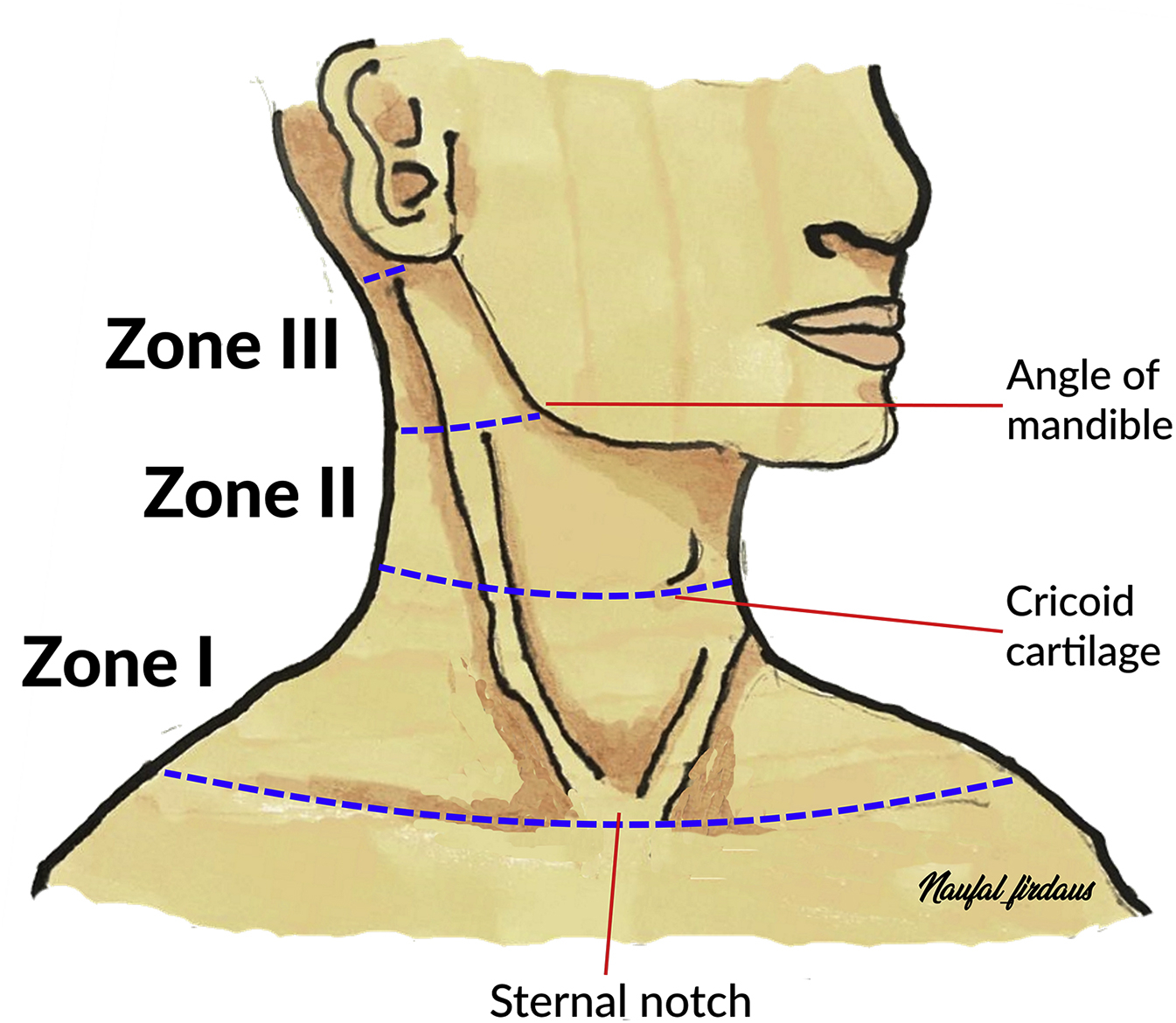
Illustration showing the level of penetrating injury to the neck according to 3 zones. Zone I: the area between the clavicles and the cricoid cartilage. Zone II: the area between the cricoid cartilage and the angle of the mandible. Zone III: the area between the angle of the mandible and the base of the skull.
Antibiotic coverage via the parenteral route should be considered empirically to avoid superimposed infection in the dirty wound after blood and swab culture and sensitivity testing. For marine injury in the summer, the 3 most common isolates were Bacillus sp, Enterobacter cloacae, and Klebsiella pneumoniae, which are sensitive to a combination of penicillin or ampicillin with levofloxacin for empiric antibiotic coverage via the parenteral or oral route. 15 Clinicians should consider ATT and its appropriateness in penetrating injuries/foreign body retention. It should be given if the patient has not received a tetanus shot in the last 5 y and if the wound is determined to be dirty.
A comprehensive physical examination is necessary to determine the extent of injury, and imaging can help suggest the approach, technique, and instrument that need to be used to retrieve the foreign body. 16 The choice of imaging modality is crucial to evaluate the injury severity, including the depth and local effects, and to look for any retained foreign body. 17 Neck radiography can sometimes be helpful to detect such findings; however, in an inconclusive study, especially in certain types of non-opacity or with small, fragmented pieces of foreign bodies, CT scan will be diagnostic. CT angiogram is mandatory if an injury to the vascular organs is suspected. A sharp foreign body is known to traumatize the vulnerable structures not only at the point and moment of entering but also during the process of withdrawal. A sharp and jagged foreign body may cause more harm during retrieval than during entrance, which is an important consideration from a surgical perspective.
Penetrating wounds need to be explored irrespective of zone in the presence of severe active bleeding, unresponsive hypovolemic shock, a rapidly expanding hematoma, blowing wound, and major hemoptysis. 13 A surgical examination can be done either under local or general anesthesia depending on the injury severity, based on individualized case judgment by the attending clinician. In our case, surgical exploration was performed with the patient under general anesthesia, owing to violation of the platysma. In this case, deeper vital structure injuries were anticipated compared to the intact platysma wound. EAST Guidelines of 2008 stated as Level I evidence that selective operative management versus mandatory exploration of penetrating injuries to zone II of the neck is both justified and safe. 18 The wound should be copiously irrigated, debrided, and closed by primary or secondary intention. 13 The size and depth of the wound will influence the need for suturing.
Conclusion
Traumatic encounters with marine animals such as needlefish can result in morbidity and mortality. A comprehensive primary and a secondary survey should be used in all penetrating traumas to rapidly identify additional injuries. Patients with penetrating neck wounds who are stable may be considered for surgical exploration once the platysma is breached. Marine penetrating injuries should be left open for secondary healing with antibiotic coverage to minimize risk of infection.
Footnotes
Acknowledgements
Acknowledgment: We thank the hospital director for permitting us to publish this case.
Author Contributions: Study concept and design (AAA, RG); involvement of the patient management and data retrieval (AAA, RG); literature search (FH, ADZ, IM, FFC); drafting and writing the case report (AAA, FH); all authors reviewed and approved the final manuscript.
Financial/Material Support: None.
Disclosures: None.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.