
Abstract
Infants and toddlers can sustain grievous craniofacial injuries after dog bites, some of which may be life-threatening. An 18-mo-old male child presented to our emergency department with complex panfacial wounds after being bitten by an unvaccinated wild dog 6 h earlier. Primary management, hemostasis, and rabies postexposure prophylaxis were performed near his home. Initially, he was resuscitated from severe hemorrhagic shock and anemia in a pediatric intensive care unit. After stabilization, early primary repair of all facial injuries was performed. Surgical exploration revealed multiple full-thickness avulsions, lacerations, nasal bone fractures, facial muscle injuries, and right ear necrosis. Gentle tissue-handling and meticulous reconstruction satisfactorily restored his facial soft-tissue contours about 64 h after the bite injury. Postoperatively, recovery was uneventful except for localized soft-tissue infection caused by multidrug-resistant Pseudomonas, which resolved with appropriate antibiotics. Nine months later, his face and ear appeared almost symmetrical with well-settled scars. Psychological recovery progressed smoothly, excepting few incidences of panic attacks that were triggered by loud noises. Here, we observed that early primary reconstruction of severely mauled soft tissues after wild dog bites, performed within 72 h with adequate precautions, safely produced satisfying long-term outcomes.
Introduction
With numerous unvaccinated wild, stray, and mixed-breed dogs roaming in the city streets and village neighborhoods of developing countries, a sizeable world population remains at risk of bites by unvaccinated dogs. 1 Age-wise, children constitute the largest segment of victims. Among children, 0- to 1-y-olds are the minority at 5%, and 6- to 12-y-olds constitute the majority (51%). 2 Although infants and toddlers are affected the least numerically, they are maximally vulnerable to craniofacial injuries owing to their short stature, disproportionately large head, tendency to crawl on the ground, extreme curiosity, subdued danger awareness, and inability to defend themselves. 3
Wound closure after bites by wild, unvaccinated, or unknown dogs remains controversial. Immediate primary suturing of such bites is not recommended. 4 Many surgeons prefer not suturing unvaccinated-dog bite injuries at all, to prevent additional trauma that may increase the risk of rabies. Some surgeons perform delayed primary repair after 5 d, while irrigating the wounds daily to decrease viral load. Another attractive alternative is to loosely appose soft tissues with gentle tissue-handling 48 to 72 h afterward, under cover of antirabies vaccine and rabies immunoglobulin, to control viral spread. This last approach was performed in this case report, and long-term results were observed.
The child’s parents provided written, informed consent for the case to be reported in the literature, including all of the content shared.
Case Report
An 18-mo-old male child presented to our emergency department unconscious and severely pale, with several avulsions and lacerations throughout his face. About 6 h earlier, he was reportedly attacked by an unknown wild dog just outside his home. His parents were out of town on an emergency and his babysitter was distracted on a phone call when he crawled outside his home unnoticed. Profusely bleeding and in severe pain, the injured child was rushed to the nearest health facility. Later, this same wild dog went on to attack 2 more children in the same village, which bordered a forest. The villagers stoned this dog to death 2 d after this incident. Forensic examination performed thereafter did not reveal Negri bodies in the brain, which are indicative of rabies infection. The recommended surveillance of the dog in a registered facility for 10 d after this incident was not possible, however.
A general physician managed the child initially, controlled the bleeding, and administered antibiotics, analgesics, and sedatives. Over the wounds, rigorous irrigation with copious amounts of normal saline for 15 min, disinfection with povidone-iodine while protecting the eyes, and light coverage with sterile dressings (without any wound suturing) were performed. Passive immunization with human rabies immunoglobulin at a dose of 20 IU·kg-1 body weight was administered deep inside of and all around the facial wounds. The recommended dose was diluted to 3 times the original volume with sterile normal saline because the extensive nature of the wounds necessitated administration of significant volumes of the immunoglobulin. Active immunization was performed with cell-cultured antirabies vaccine. After primary treatment, the child was referred to our hospital and reached us after a 4-h journey in a private vehicle.
Physical examination at our hospital emergency department revealed multiple avulsions and lacerations all over the child’s face, but more so on the right (Figure 1A). Underlying facial muscles appeared mauled, covered with thick clots, and associated with nasal bone fractures (Figure 1B and C). The right ear was severely avulsed, with the helix torn off from the rest of the ear, hanging on a small base (Figure 1D). The child was pale, drowsy, tachycardic, and tachypneic at presentation. Even after receiving adequate oxygen through a face mask, his oxygen saturation levels gradually fell below normal. Arterial blood gas analysis on admission revealed low hemoglobin of 5.2 g·dL-1 (normal 12–17 g·dL-1) and high lactate of 13 mmol·L-1 (normal 2 mmol·L-1), signifying severe anemia and hemorrhagic shock. The child was intubated to prevent desaturation and was successfully resuscitated at our pediatric intensive care unit. All of his wounds were irrigated at the bedside once every day, and prophylactic broad-spectrum antibiotic combinations of intravenous amoxycillin-clavulanate and amikacin were started empirically. Bedside facial radiograms did not reveal any gross bony injuries, excepting the nasal bone fracture. The patient’s parents were counselled extensively about different treatment options. After diligent deliberation, considering risks, benefits, and costs, they chose an early primary repair. Accordingly, after hemodynamic stabilization, surgical exploration was performed with the patient under general anesthesia about 64 h after the bite injury.

An 18-mo-old child after being bitten by a wild dog. (A) Frontal view showing facial avulsions, lacerations, and nasal fracture. (B) Right oblique view showing mauled lips, ear, and face with clots over frontalis. (C) Nasal trauma showing fractured nasal bones. (D) Torn and ripped portions of the right ear.
Multiple full-thickness avulsions with extensive tissue loss and lacerations throughout the face, with fractured nasal bones, were found on intraoperative examination (Figure 2A). Facial muscles were ripped off the underlying bones in several areas, creating interconnected pockets (Figure 2B and C). Avulsion of the right ear ripped the helix off the concha, necrosing the antihelix and crura in the middle, with demarcation forming between healthy and necrotic tissues (Figure 2D). The injury was classified as a World Health Organization Category III animal bite. 5 According to Lackmann’s classification for pediatric dog bites, it was Type IV B. 6

Intraoperative findings. (A) Nasal bone fracture fragments after alignment. (B) Interconnected deep soft-tissue pockets observed over the right midface. (C) Frontalis muscle seen to be ripped off the bone, but the underlying nerves are preserved. (D) Zones of demarcation (black arrows) gradually forming between necrosing and healthy tissues over the right ear.
All wounds were rigorously irrigated under high pressure for approximately 30 min with 0.9% saline-filled 50-mL syringes fitted with an 18G needle. After protecting the patient’s eyes, substantial amounts of 10% povidone-iodine were smeared throughout all wounds for 5 min and flushed with normal saline before repair. Fractured nasal bones were carefully aligned. Soft tissues were meticulously apposed following the principles of wound closure with triple-plane dissection over the forehead and deep-plane augmented facial flaps over the mid and lower face.7,8 To preserve facial symmetry and harmony, reconstruction of the face progressed from central to peripheral with several tension-free synthetic sutures that were loose enough to allow free drainage from deep tissues, while avoiding excessive soft-tissue dissection (Figure 3A and B). Necrosed areas over the right ear were debrided, and remaining ear flaps were satisfactorily juxtaposed to remold the mutilated ear (Figure 3C).
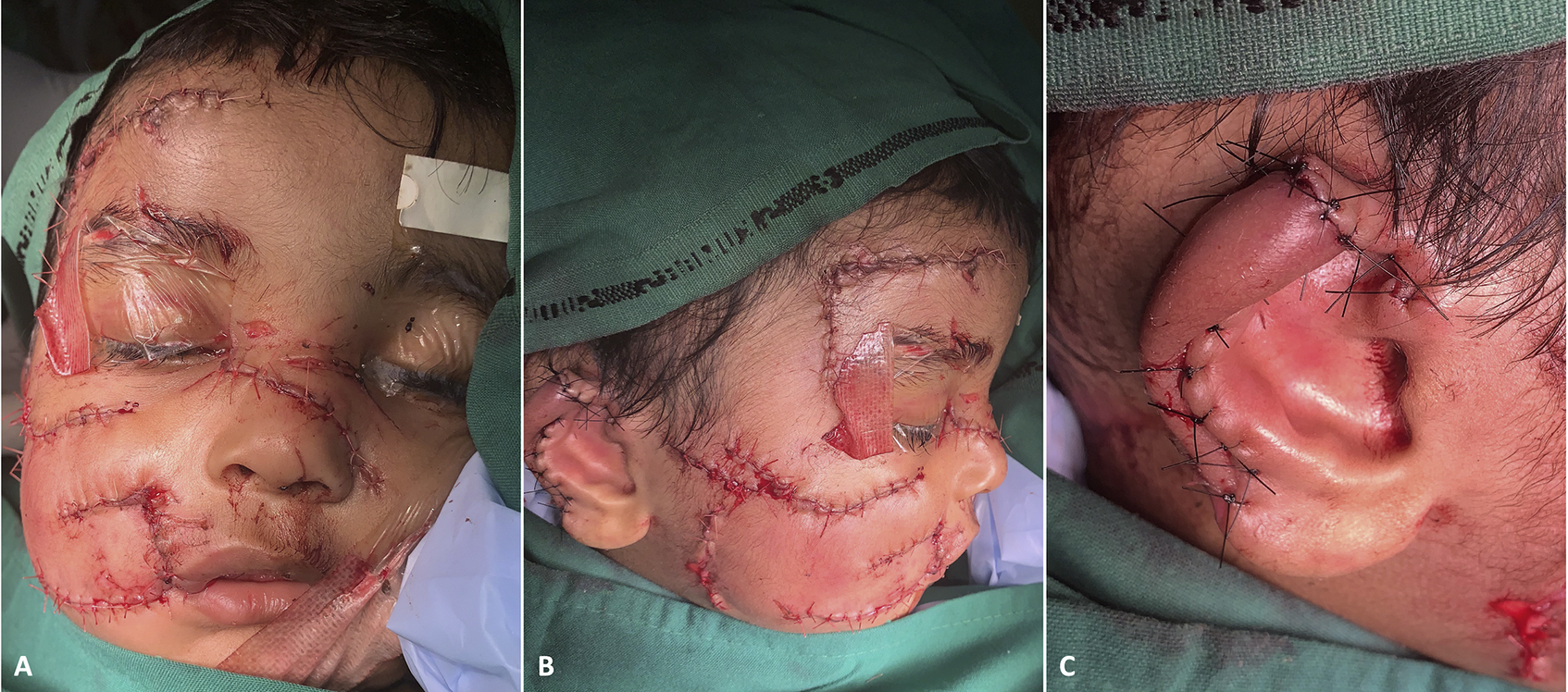
Immediate postoperative results after tension-free apposition of soft tissues. (A) Frontal view. (B) Right lateral view. (C) Right ear.
After discharge, about 1 wk postoperatively, scanty purulent discharge was noticed over a corner of 1 of the midface wounds, with redness and swelling of 2 × 2 cm adjacent areas. Wound swab was culture-positive for multidrug-resistant Pseudomonas aeruginosa, resistant to the antibiotics started earlier. After the results of a sensitivity profile, intravenous meropenem was combined with tigecycline for the next few days to control this infection. Antirabies vaccination was completed as scheduled on days 0, 3, 7, and 28. 5 Initially, the involved areas were considerably edematous, but this subsided appreciably within the next 2 wk. Swelling and redness were still visible at the infected area, with about 1 mm of marginal skin necrosis (Figure 4A). Movements over the affected areas were restricted during the first postoperative month and improved gradually afterward. Scars, including the cross-hatches, were reddish and overtly visible during the first 2 mo (Figure 4A and B). The remolded right ear appeared well shaped (Figure 4C). The child was withdrawn, afraid, and extremely irritable during the early months, requiring psychological counseling and constant parental care. Otherwise, his recovery was mostly uncomplicated and uneventful.

Postoperative results after 2 wk. (A) Frontal view showing residual redness, swelling, and marginal wound necrosis over right lower midface (this area was infected secondarily). (B) Right lateral view of the healing wounds and scars. (C) Remolded right ear.
Nine months postoperatively, his facial appearance and expressions were well balanced and pleasing. Complete reanimation of all avulsed facial muscles resulted in coordinated and harmonious facial movements. Scars settled well and were barely noticeable from afar. Some amount of scar stretching was noticeable in some areas, however (Figure 5A and B). His right ear, although a bit smaller and floppier, appeared nearly symmetrical (Figure 5C). Psychologically, for the first 6 mo, he experienced severe bouts of panic attacks from loud noises, especially the noises of lightning during storms. He improved thereafter, and after 9 mo, while still avoiding all dogs, he would sometimes be fearful after hearing the noise of leaves rustling during high winds. Otherwise, he recovered well under the supervision of a psychologist and a pediatrician. Both of the child’s parents expressed deep satisfaction with the entire treatment process, with the final outcome and recovery far exceeding their expectations.

Postoperative results after 9 mo show a near-normal facial appearance and function with scars bettering over time. (A) Frontal view. (B) Right lateral view. (C) Right ear.
Discussion
Dog bites are preventable injuries and yet pose a significant public health problem globally. In children, facial dog bites usually occur after prolonged eye contact with the dog, while bending over the dog, after overt familiarity, or when remaining indoors together for a long time without going out for walks. 2 Close supervision of all child–dog interactions, not leaving any child unattended around any dog, proper vaccination of all dogs, and prompt reporting of all dog bites help to protect children. Dog bites are more common in children than in adults, with 76% occurring in the head/neck region. Cheeks, lips, and nose are commonly affected as the “central target region” in children younger than 18 mo. 9 In comparison, older children usually sustain dog bites to their extremities because they are taller.
Soft-tissue dog bite injuries are classified into 3 major types: laceration, avulsion, and puncture. Typically, a combination of all 3 are present. A biting dog’s jaw usually produces a powerful force of 1380 to 3100 kPa (200–450 pounds per square inch), which is strong enough to perforate metal sheets. Frequently, the ripping-and-tearing motion associated with a dog bite devitalizes the wounded soft tissues and damages underlying vessels and nerves. 10 During admission, alerting patients about the chances of wound necrosis, infections, scars, foreign bodies, and rabies helps in overall management. 9 Facial bone fractures after dog bites in children are rare, occurring in about 1 to 2%. The compressive force of dog bites is sufficient to fracture thin facial bones in children, especially over the orbit, nose, and skull. Facial bones in growing children are spongy, have high regenerative potential, and possess osteogenic capabilities. When correctly aligned, these properties frequently result in proper fracture healing. 11
Soft-tissue infections after dog bites occur in around 10%, with Pasteurella canis being the most commonly (50%) isolated organism. Other bacteria such as Fusobacterium, Bacteroides, Prevotella, and Pseudomonas may also be present. 12 Capnocytophaga canimorus is an uncommon but fearsome slowly growing organism with a prolonged incubation period of 1 to 7 d that causes septic shock and purpura fulminans in susceptible patients, with 25% mortality. 13 Short courses of preemptive antimicrobials are recommended for moderate-to-severe bite injuries over the face and upper limbs. Longer courses are preferred for severe injuries with bony fractures and joint penetration.4,6 Amoxicillin-clavulanate is effective against most pathogens, including Pasteurella and Capnocytophaga, and amikacin is effective against gram-negative bacteria including Pseudomonas. 4 Thus, combining these 2 antibiotics empirically provides good protection.
From an aesthetic perspective, open wounds allowed to heal secondarily often form unacceptable disfiguring lifelong scars. When compared to nonsuturing, wounds closed within the first 24 h achieve better aesthesis and function with similar secondary infection rates. Wound management started early also results in decreased infection rates and improved aesthetic outcomes, regardless of suturing status. 14 Scalp and forehead are relatively tough tissues, and a limited triple-plane dissection helps in meticulous repair of injuries over these areas. 7 Over the cheeks and lower face, a deep-plane cervicofacial flap-like approach is helpful. 15 Mobilizing the mauled and avulsed segments of facial soft tissues as a large and thick augmented facial flap ensures adequate vascularity to the wound edges while avoiding undue dissection of the adjacent healthy areas. 8 Because facial reconstruction of the central target area is more complicated, the lip vermilion and commissure, nose margins, and nasal columella are reconstructed first. Substantial tissue loss after avulsions may require reconstructive flaps or grafts. If initial surgery is delayed for any reason, delayed primary closure up to 5 d later, with daily wound irrigation, remains a good option. 16
Conclusions
Major dog bite injuries persist as a global public health problem. Psychological issues are equally significant in affected patients. Here, an early primary meticulous reconstruction of the severely mauled panfacial soft tissues, after taking comprehensive precautions, produced pleasing long-term surgical results in an 18-mo-old child. Vigilance during the postoperative period and a prolonged medical and psychological supervision helped in good patient recovery, yielding excellent patient-reported outcomes.
Footnotes
Acknowledgements
Acknowledgments: The author thanks Dr. Tamal Laha, MD, and Dr. Abhishek Poddar, MD for their contribution to the successful clinical management of this patient.
Financial/Material Support: None.
Disclosures: None.