
Abstract
Snakebites are a neglected and underestimated global health hazard. In the Brazilian Amazon, Bothrops snakebites are the most prevalent and may lead to severe complications. Here we describe a severe case of Bothrops atrox snakebite that, owing to delayed medical assistance, presented with renal and respiratory failure, compartment syndrome, and tissue necrosis. After several fasciotomy surgeries, the patient survived; however, he showed significant functional disability. Prompt management of snake envenomation would aid in the early diagnosis of local and systemic complications and, consequently, would result in a better functional outcome with improved quality of life.
Introduction
Snakebite is a neglected global health problem with more than 6 billion people at risk of envenomation. 1 It causes considerable morbidity and mortality rates and is responsible for more than 100,000 deaths annually. 2 The greatest burdens are among the poor and isolated rural communities where interaction between snakes and humans is high and access to adequate healthcare is scarce. 3 Latin America is considered a hotspot of venomous snakes. 1 A recent study showed that the Bothrops genus was responsible for 81% of the snakebites in the Brazilian Amazon between 2010 and 2015 (57,374 of 70,816 cases). 4 Bothrops atrox, also known as the Amazonian lancehead, belongs to a clade of Neotropical pit vipers, which inhabit rainforests, drylands, and other ecosystems. 5 Complications can be localized and manifest as pain, swelling, ecchymosis, blistering, and necrosis, or they can be systemic and characterized by disseminated hemorrhage, stroke, and acute renal failure. 6 –8
Compartment syndrome (CS) is a serious and uncommon complication of Bothrops snakebites. 9 –11 Delay in diagnosis and treatment can increase the associated ischemic nerve damage and muscle necrosis. 12 In this report, we describe a case of a man who survived Bothrops atrox envenomation but developed CS and tissue necrosis that required fasciotomy, grafting, and intensive care, with resultant chronic disability.
Case report
A 27-y-old male with higher education residing in the municipality of Sena Madureira in the State of Acre in the Western Brazilian Amazon was bitten by a snake described as a presumed Bothrops atrox. The incident occurred in the morning as he was returning home from leisure activities (fishing). The bite was on his lower right limb. Immediately after the accident, the patient felt acute pain at the site of the bite but continued on his way home. During the walk home, he started to feel dizzy and nauseated and had blurred vision. Upon arriving home, soap and water were used to clean the wound, and family members offered him específico pessoa, an oral admixture of plant extracts with variable composition, which led to several vomiting episodes. The exact composition of the específico pessoa used in this case is unavailable. After an hour, the patient developed confusion but decided to stay at home. No other medicines were used locally.
After 2 d of progressive symptoms, he was taken to a local health facility for medical consultation, from which he was quickly transferred to a specialized hospital in the municipality of Rio Branco (141 km away). He arrived on the same day in the early morning. An initial clinical examination revealed a blood pressure of 100/60 mm Hg and confusion. Twelve vials (total of 120 mL) of Bothrops antivenom (AV) were administered. The patient lost consciousness, and endotracheal intubation was required. He was admitted to the intensive care unit.
Laboratory test parameters at admission revealed leukopenia (which later evolved to leukocytosis), thrombocytopenia, and elevation of creatinine, urea, and creatine kinase, the latter possibly indicating rhabdomyolysis (Table 1). According to acute kidney injury network guidelines, 13 the patient presented a stage 3 renal injury; venous hydration was optimized, and no renal replacement therapy was necessary according to attending physician discretion (Table 1).
Laboratory parameters during hospitalization
ALT, alanine transaminase enzyme; AST, aspartate transaminase enzyme; Cl-, chlorine; Cr, creatinine; CK, creatine kinase; CK-MB, creatine kinase muscle-brain; INR, international normalized ratio; K+, potassium; LDH, Lactate dehydrogenase; Na+, sodium; PTT, partial thromboplastin time; TAP, prothrombin time; WBC, white blood cells.
The patient’s health status continued to decline. The attending physicians clinically diagnosed CS and conducted an extensive fasciotomy on the affected limb (Figure 1). Intramuscular pressure measurement was not performed. Antibiotics (vancomycin 1 g every 3 d, imipenem 500 mg + fluconazole 200 mg every 12 h) were administered; blood pressure decreased, and vasoactive drugs for shock (3 ampoules of noradrenaline, 8 mg/ampoule, 4 mg/4 mL, and 1 ampoule of dobutamine, or 20 mL/250 mg) were prescribed.
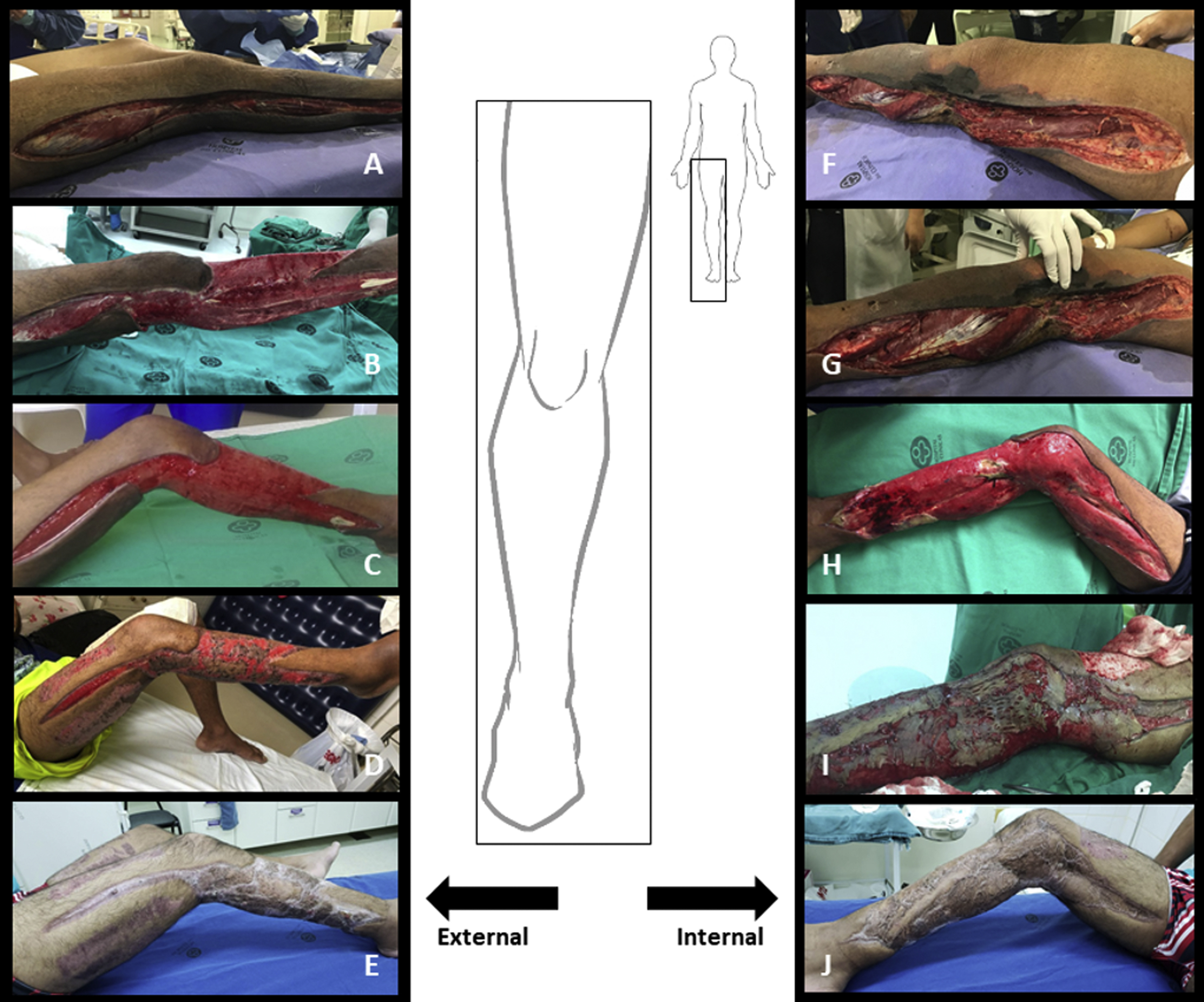
Initial and healed aspects of the wound (used with permission of the patient). Fasciotomy of the right leg on D13 after snakebite (A, F). External and internal region of the right leg after surgical removal of the necrotic tissue (B, C; G, H). Skin grafting procedure on D42 after snakebite (I). Healing phase on D47 after snakebite (D). Complete healing 4 mo after the accident (E, J).
On D13 after the bite, a surgical debridement procedure was performed for extensive necrosis at the fasciotomy site. The antibiotics regimen was adjusted (vancomycin 1 g every 12 h, imipenem 1 g every 6 h + fluconazole 200 mg every 12 h). Blood (from the central venous catheter) and urine cultures were negative on D20 postbite. There were no signs of infection at the snakebite site; therefore, no cultures from the bite site were performed.
After 26 d of hospitalization (29 d after the bite), the patient was discharged from the intensive care unit. In total, he was hospitalized for 74 d. During this period, he underwent 3 other surgical procedures (partial skin grafting and debridement of necrotized tissue; Figure 1), which occurred on D42, D49, and D63 postsnakebite. After discharge from the hospital, postsurgery assessments were conducted through follow-up visits at the outpatient clinic. No physical rehabilitation took place as there was no multidisciplinary care facility available in the city.
The patient’s disability was assessed after 4 mo, using the World Health Organization disability assessment schedule (WHODAS 2.0). 14 The questionnaire was administered by phone interview and yielded the following results regarding the patient’s extent of disability: 33% impairment in the cognition domain; 55% impairment in the mobility domain; 38% in the self-care domain; 10% in the getting along domain; 88% in impact in life activities; and 63% in participating in society. The patient gave consent to reporting of this case.
Discussion
The patient in this case report fits the profile of the majority of snakebite victims in the Amazon region: male, of productive age, rural resident, and affected in the lower limbs. 15 –22 The patient was walking in lowlands after fishing activities. This type of animal encounter is not unusual in the lowlands; riverine communities settle there near rivers because of their economic productivity potential. 4
The vast majority of snakebite envenomations have low to moderate severity.15,18,19,23,24 Uncoagulable blood and spontaneous systemic bleeding, tissue necrosis, hemodynamic instability, shock, and respiratory and renal failure are common complications in severe cases.7,12,16,25–27
CS originates from an acute and intense local inflammatory response confined to anatomical spaces surrounded by noncompliant tissues such as muscle fascia, ligaments, and bone. The resulting edema leads to an intracompartmental pressure increase, which disrupts adequate blood flow to distal tissue, subsequently leading to neurovascular ischemia and necrosis if not diagnosed and treated quickly. 26 In snake envenomation, this process may be initiated by hemotoxic/cytotoxic effects of venom at the envenomation site. Of note, pain, swelling, hemodynamic instability, and hemorrhage are also common clinical features of snake envenomation. Therefore, clinical signs and symptoms of snake envenomation may mimic clinical features of CS, which may not be solely explained by the presence of snake fang injuries at the injection site. To complicate matters, evidence of snakebite is not always distinguishable on the initial examination, which could be misleading. As an example, distal pulselessness and pallor may be explained by circulatory shock and local edema owing to toxic effects at the injection site and not necessarily by the development of CS. Finally, unnecessary and debilitating surgical treatment, such as fasciotomy and amputation, may occur.
The diagnosis and management of CS secondary to snakebites have been a matter of great debate among researchers, clinicians, and surgeons for decades. It is important to mention that the clinical presentation of CS secondary to high-impact trauma (eg, vehicle collisions), despite having the same underlying pathologic causes, is in most cases very clear and distinguishable from CS secondary to snake envenomation, as mentioned. To decide whether to proceed with aggressive and immediate surgical procedures such as fasciotomy and amputation after envenomation or when to manage under conservative approaches with comprehensive examinations, repeated AV administration associated with serial pressure measurements and even decompressive fasciotomies is challenging, especially in low-resource settings.
According to a panel of US surgeons, 28 the advent of safe antivenom and its widespread availability in the United States has drastically decreased the need for urgent and aggressive surgical interventions in crotaline snake envenomation, the most prevalent cause of snake envenomation in the United States. 29 The authors developed and discussed the best practice guidelines for surgical interventions for acute management of crotaline snake envenomation, which takes into consideration the previously published optimal management algorithm for such cases. 30 It is suggested that after standard treatment and detailed neurovascular examination, compartment pressure serial measurements should be done. Thus, the decision to proceed with surgical approaches should be made to occur after serial pressure measurements and evidence of neurovascular compromise are consistent with tissue damage. 28 The exact pressure cut-off point remains debatable. 31 Imaging techniques as Doppler ultrasound, 31 or even magnetic resonance imaging, could help to properly manage vascular emergencies. 11
Few studies have reported CS in Bothrops snakebites. 9 -11,32,33 The frequency may vary according to geographic region. For instance, a study in Korea reported that 33 of 59 (56%) patients presenting to hospitals with snakebites were suspected to have CS, of whom 17 (51%) had elevated compartmental pressure and were managed with fasciotomy. In the current case, compartmental pressure was not measured; however, the clinical features were consistent with CS, according to attending physicians.
Remote places, such as the deep Amazon, have scarce access to snake AV and inadequate patient management, and the health facilities in some cases lack AV vials. Thus, strategies adopted by highly developed countries, such as the United States, may not be feasible in the remote areas of the Amazon. Accordingly, physicians and the multidisciplinary team use whatever modalities are available to save a limb, or a life, even if aggressive surgical procedures are the only option.
Furthermore, the risk of secondary infection caused by the bacteria flora present in the snake’s mouth 21 needs to be considered. Follow-up evaluation for potential worsening wound conditions should always be performed to ensure timely necrotic tissue debridement. Antibiotic treatment also needs to be updated to avoid a chronic functional loss to secondary motor disabilities. 34 In severe cases, amputation may be necessary if intensified and comprehensive approaches are not an option.24,27 Although amputation was not necessary in the present case, several motor sequelae persisted.
The majority of snakebite envenomation victims are generally involved in agricultural or pastoral activities. If they survive the envenomation, they experience great physical and psychological disabilities that hamper the sustainability and socioeconomic stability of their family and the local community. 2 Barriers to accessing rehabilitation services are commonly experienced after hospital discharge in snakebite endemic regions. This inaccessibility further diminishes recovery and return to previous socioeconomic activities, including work. The patient discussed here thus faces major limitations in several domains, according to the WHODAS 2.0 tool. Several months after the bite, the patient was not yet able to resume previous activities and relied on family for daily activities and financial support.
Time is a critical factor when treating snakebite envenomation. After the accident, access to proper medical attention was delayed for more than 48 h. In the Amazon region, the time between envenomation and medical assistance needs to be within 6 h; nonetheless, riverine topography and transportation in the area have become important factors that may affect clinical outcomes.15,18,21,27,35–38 In addition, the reduced number of hospitals, together with insufficient medical equipment and staff, contributes to reduced effectiveness of snakebite management in rural areas.15,21,27,35,36,39,40
Indigenous and riverine beliefs are important aspects to consider and may contribute to snakebite AV treatment delay and clinical outcome, as observed in this case. Medicinal plant extracts are widely used for such cases, especially where proper AV is scarce. 41 Despite not having proven efficacy against Bothrops atrox snakebite venom,42,43 específico pessoa as described here is still used by the population.21,27 Other common empirical practices are perforation and suction of the wound.40,44,45
Lastly, it is of the utmost importance to mention the sustainable development goals (SDG) developed by the United Nations. SDG-3 highlights the urgent need to achieve universal health coverage for good health and wellbeing. 46 It aims to ensure that all individuals and communities receive the full spectrum of essential healthcare services, including promotion, prevention, treatment, rehabilitation, and palliative care. The Brazilian government has been addressing the SDGs with multiannual plans and initiatives, 47 but more needs to be done. As a neglected condition, snakebite envenomation represents a major concern faced by poor and rural populations, with great economical prejudice to local communities. Proper access to AV, medical care, and rehabilitation services needs to be properly and urgently tackled by policymakers.
Conclusions
Snakebite can lead to extensive tissue loss and chronic disabilities. As a result, the overall quality of life and economic activities in the community is negatively affected. We emphasize that severe complications, such as CS, are possible outcomes of Bothrops snakebites and that shorter periods between snakebite and AV administration need to be pursued. Patient assessment should be serial and comprehensively performed, taking into account whatever treatment modalities are available in the healthcare facility. Aggressive surgical procedures should be avoided except as the last option. Nonetheless, differences between developed and underdeveloped countries exist and are reflected in the management of patients with snakebite. It should not be presumed that existing guidelines followed in developed countries, despite having high clinical evidence of efficacy, can be easily adopted in low-income areas. Postdischarge rehabilitation services, such as psychological, physical and occupational therapy, should be accessible to surviving snakebite victims for better and improved functional, psychological, and social outcomes.
In summary, prompt and effective treatment, rehabilitation availability, and proper access to education and prevention strategies regarding ways of approaching activities in rural areas without increased exposure to such risks are essential to tackle this worldwide problem and reduce disability rates.
Footnotes
Acknowledgements
Author Contributions: Study concept and design (JAGS, CSM, FFV, WMM); acquisition of the data (CSM, TGS); analysis of the data (JAGS, FFV, JAA, NCV); drafting of the manuscript (JAGS, FFV, JAA, NCV); critical revision of the manuscript (IMS, MFS, LCF, WMM); and approval of final manuscript (FGS, FFV, JAA, NCV, CSM, IMS, TGS, MFS, LCF, WMM).
Financial/Material Support: None.
Disclosures: None