
Abstract
The objective of this case series was to describe 2 patients presenting with subarachnoid hemorrhage with hydrocephalus and hemoventricle after a snakebite caused by presumed Bothrops ssp. Both cases occurred in the municipality of Guajará (Amazonas state), Western Brazilian Amazon. Both cases featured delay in administration of serum therapy, which may have contributed to the emergence of complications such as stroke. Patient 1 was admitted to hospital 16 h after the snakebite occurred. Before receiving antivenom, testing showed the patient as having unclottable blood. She developed hemorrhagic stroke (a subarachnoid hemorrhage with hydrocephalus and hemoventricle). On the seventh day, she was discharged from hospital. Patient 2 arrived at the hospital 3 d after the snakebite occurred and presented with unclottable blood. He had a stroke (right frontoparietal hemorrhage, intraparenchymal hemorrhage already open to the ventricle) and died on the eighth day after the snakebite. Delay in seeking health care after snake envenomation can result in worse outcome.
Introduction
In Brazil, on average, 26,000 medically important snakebites occur per year, and the lethality rate is around 0.4%. 1 Snakebites caused by Bothrops spp. are the most commonly reported in Brazil. 2 Victims of envenomation caused by these snakes present local signs and symptoms such as pain, edema, ecchymosis, blisters, and necrosis, as well as systemic symptoms such as alterations in blood coagulation, spontaneous bleeding, and renal failure. 3 –6
Bleeding occurs due to the action of antithrombotic properties of some components of the venom, such as metalloproteases, serinoproteinases, and phospholipases A2. 7 These components lead to the consumption of platelets, fibrinogen, and other coagulation factors. 8 When coagulopathy results in systemic bleeding, the central nervous system can be affected. 9 Cerebrovascular complications caused by Bothrops envenomations are estimated to occur in around 3% of patients, of whom 63% die and the remaining develop irreversible sequelae. 10 In the Amazon, a fatal case of hemorrhagic stroke was reported after Bothrops envenomation. 11
In this case series, we report on 2 cases of subarachnoid hemorrhage with hydrocephalus and hemoventricle after snakebite caused by presumed Bothrops spp. in the municipality of Guajará (Amazonas state), Western Brazilian Amazon.
Case Report 1
Patient 1 was a 65-y-old female illiterate agricultural worker and a resident in the Badejo de Cima community in the municipality of Guajará, Amazonas state. The snakebite occurred at 0600; despite killing the snake, she did not bring it to the hospital or take a photograph of it. At the time of the bite, she was in the yard wearing sandals and believes that she walked past the snake, which was around 40 cm long, had a tail with a white end, and was described as being a presumed jararaca (popular name for Bothrops atrox). No first aid was given, although she reported having drunk bitter black coffee to “reduce the effects of the venom,” which is a common practice in the region.
She was bitten on the lower left leg (heel). Initially, she experienced no symptoms; however, after a short period of being asymptomatic, she reported dizziness, vomiting, and pain at the bite site. From 0800 onward, vomiting intensified and headache began in the nape of neck area. At this point, she decided to seek medical care. The same day, she went to the Juruá Regional Hospital, Cruzeiro do Sul, in the state of Acre, and was admitted at 2220, 16 h after the bite occurred.
On admission, she had high blood pressure (170/100 mm Hg), bradycardia (58 beats·min-1), and tachypnea (24 breaths·min-1) but no fever (36°C). She reported vomiting and a severe, persistent, holocranial headache, which were the reasons for which her family brought her to the hospital. At the site of the bite, on the left heel, puncture wounds could be seen, as well as edema 2+/4+ in 2 segments (foot and leg) and ecchymosis. Furthermore, her level of consciousness was decreased; she was lethargic, sleepy, and had mydriatric but responsive pupils. Before receiving antivenom at 2250, a Lee-White clotting time test was carried out, which showed her as having unclottable blood. Laboratory results are presented in Table 1. Thirty minutes after premedication with intravenous (IV) promethazine, IV dipyrone, and IV hydrocortizone, 6 vials of Bothrops-Lachesis antivenom (Butantan Institute, São Paulo, Brazil, acquired by the Ministry of Health for national distribution) were administered by IV (1 vial neutralizing 5 mg·mL-1 of reference Bothrops jararaca venom in mice). Bothrops atrox envenomation was confirmed through enzyme-linked immunosorbent assay. 12
Case report 1—laboratory parameters during hospitalization
Reference values: hemoglobin: 13.0–16.0 g·dL-1; hematocrit: 40–54%; platelets: 130,000-400,000/mm3; leukocyte: 4,000–10,000/mm3; glucose: 70–99 mg·dL-1; urea: 10–45 mg·dL-1; creatinine: 0.5–1.2 mg·dL-1 for adults; sodium: 140–148 mmol·L-1; potassium: 3.6–5.2 mmol·L-1; chlorine: 98–108 mmol·L-1; alanine transaminase: 2–44 UI·L-1; aspartate transaminase: 2-38 IU·L-1; international normalized ratio: 1.00.
By 1220 the next day, the patient’s clinical condition had worsened, and she was admitted to the intensive care unit (ICU) for endotracheal intubation and respiratory support. A computed tomography (CT) brain scan revealed a subarachnoid hemorrhage with hydrocephalus and hemoventricle (Figure 1). Diffuse cerebral edema and subcortical hypodensity of nonspecific appearance in the left parietal lobe were also noted. The patient was prescribed hydration, mannitol, metoclopramide, midazolam, and furosemide. Because her blood was still unclottable, an additional 6 vials of Bothrops-Lachesis antivenom were administered, after the premedication previously used. Blood pressure was 120/70 mm Hg, respiratory rate was 15 breaths·min-1, and axillary temperature was 33.5°C.
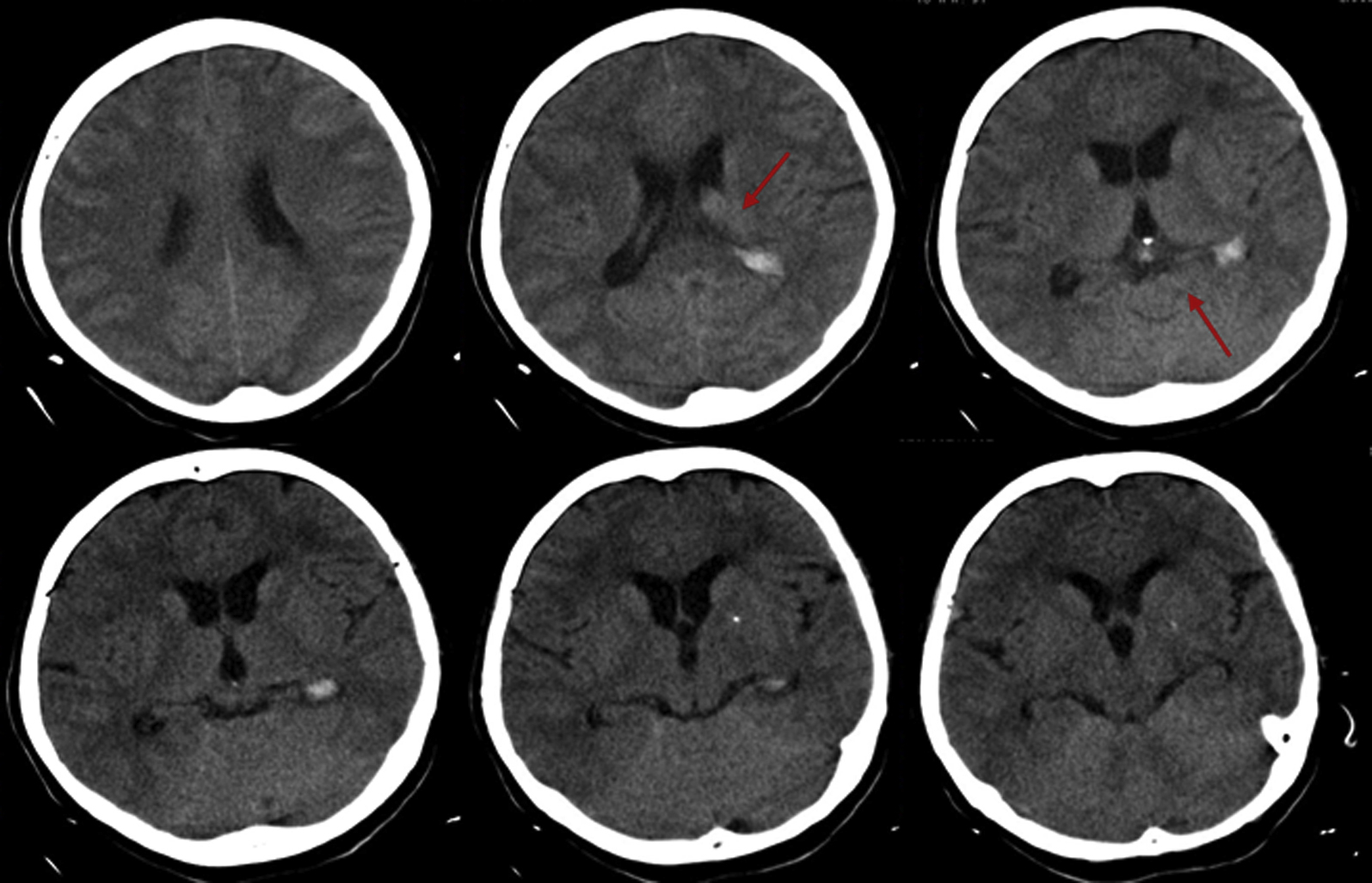
Patient 1. Cranial computed tomography scan.
The patient had clinical improvement by the third day of hospitalization. With these parameters, the patient was discharged from the ICU and transferred to the clinical ward. On the fourth day of hospitalization, she continued on an oral diet, was aware of time and space, and was calm, stable, and afebrile. She had upper and lower limb ecchymosis on the side of the body where the bite had occurred (left side). During the fifth to the seventh day of hospitalization, the patient remained stable with improvement in levels of pain and lower limb mobility. On the seventh day, she was discharged from the hospital.
Case Report 2
Patient 2, a 22-y-old male teacher, was admitted to the Juruá Regional Hospital in the municipality of Cruzeiro do Sul, Acre, having come from the Bom Jesus community in the municipality of Guajará, Amazonas state. According to information from companions, the patient had been bitten 3 d previously by the snake popularly known as jararaca. His companions reported that he was wearing sandals at the time of the bite and stepped on the snake while it was in movement. The snake bit his foot twice. The first bite affected the back of the right foot, and the second bite affected the plantar region and part of the back of the foot (Figure 2A–2C).
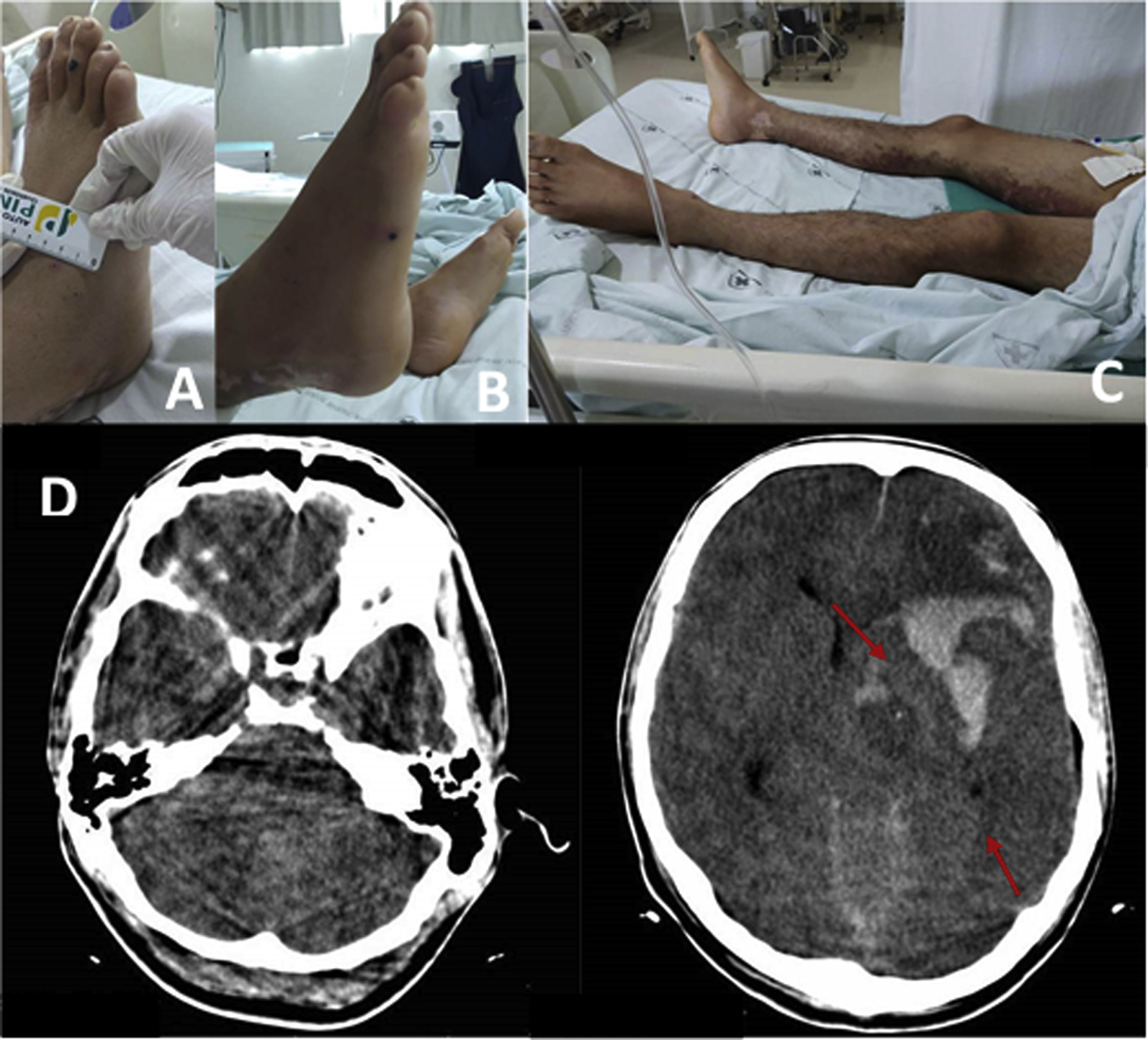
Patient 2. (A) Bite affected the back of the right foot and (B) the plantar region and part of the back of the foot. (C) General view of the patient bitten by snake. (D) Cranial computed tomography scan and images of the snakebite.
According to family members, the patient initially reported that the affected limb had mild edema up to the medial third of the leg, so he decided to treat himself at home and not seek medical attention. They adopted the use of Específico Pessoa, which is a traditional medicine used to treat snakebites in the Brazilian Amazon. No water was given to the victim for at least the following 24 h. On the third day after being bitten, the patient began to report a severe headache, tachycardia, and eye pain. His mother gave him anti-inflammatory and analgesic drugs, and the symptoms became more intense with aphasia and, later, a lack of consciousness.
After the administration of 8 vials of Bothrops-Lachesis antivenom in Guajará city, the patient was referred to the Juruá Regional Hospital, 36 h after the bite occurred. On admission, he was unconscious, eupneic, and tachycardic. His Glasgow Coma Scale score was 8, blood pressure was 160/130 mm Hg, heart rate was 117 beats·min-1, temperature was 39°C, oxygen saturation was 93%, and pupils were mydriatic. The patient was prescribed 30 mL of midazolam. Thirty minutes after premedication with IV promethazine, IV dipyrone, and IV hydrocortizone, an additional 4 vials of Bothrops-Lachesis antivenom were prescribed. Laboratory results are presented in Table 2. The patient was admitted to the ICU for endotracheal intubation. A CT scan revealed that the patient had experienced a stroke with right frontoparietal hemorrhage, intraparenchymal hemorrhage already open to the ventricle (Figure 2D), very visible significant edema that deviated from the midline, and subarachnoid hemorrhage.
Case report 2—laboratory parameters during hospitalization
Reference values: hemoglobin: 13.0–16.0 g·dL-1; hematocrit: 40–54%; platelets: 130,000–400,000/mm3; leukocyte: 4,000–10,000/mm3; glucose: 70–99 mg·dL-1; urea: 10–45 mg·dL-1; creatinine: 0.5–1.2 mg·dL-1 for adults; sodium: 140–148 mmol·L-1; potassium: 3.6–5.2 mmol·L-1; chlorine: 98–108 mmol·L-1; alanine transaminase: 2–44 UI·L-1; aspartate transaminase: 2–38 IU·L-1; international normalized ratio: 1.00.
On the fifth day of hospitalization, he presented bradycardia, was hypotensive and hypothermic, and did not respond to pain stimuli. Signs were suggestive of brain death and lack of respiratory drive, with reflex cough absent and mydriatic pupils. Glasgow coma scale score was 3. The next day, the patient developed gingival bleeding, blood pressure was 76/43 mm Hg, temperature was 38.7°C, heart rate was 119 beats·min-1, and oxygen saturation was 64%. The patient died later that day.
Discussion
Hemorrhagic stroke is characterized by bleeding in the brain tissue, cerebellum, or brain stem. This leakage can lead to clinical manifestations that are related to the volume of blood transported to the extravascular space and to the location of the hemorrhage.13,14 The signs and symptoms observed in our study, such as lower levels of consciousness, were compatible with brain damage and indicated a suspected stroke. These manifestations appear in patients with persistently depressed sensorium and focal neurological deficits that begin early and then develop into cerebrovascular lesions after snakebite envenomation, as was observed in our 2 cases. 15
The diagnoses were confirmed by clinical findings associated with CT examination. Imaging is the method of choice for immediate detection of cerebrovascular hemorrhage. 13 Some cases of Bothrops snakebites that have caused cerebrovascular hemorrhage have been reported previously. In Colombia, for example, a 48-y-old woman had a magnetic resonance imaging-confirmed ischemic stroke on the fourth day after admission. 16 In Brazil, two 65-y-old women in the state of Bahia 17 and a 62-y-old woman in the state of Pará also had hemorrhagic stroke due to snakebite by Bothrops. 18 In the cases that occurred in Bahia, there was confirmation by CT scan within the first 24 h after the bite. In the case reported in Pará, the condition began with edema, local erythema, and severe pain, although without blisters. Laboratory tests were performed; however, the results showed the patient to be within the normal parameters. An axial tomography scan of the skull was performed 24 h after the incident and revealed carotid atheromatous calcifications, hemorrhagic lesions with perilesional edema measuring 20 to 30 mm in the left frontal and right parietal lobe, and partially erased brain grooves.
An interesting, albeit fatal, case occurred in the Amazonas state, where a 59-y-old woman with Bothrops envenomation showed clinical signs of cerebrovascular hemorrhage on admission to the hospital, just 1.5 h after the snakebite. The confirmation of stroke occurred post mortem on the third day after the snakebite, and snake venom was noted as present in the brain tissue. 11 A review of 83 case reports of cerebrovascular accidents due to snake envenomation found that 77% had ischemic stroke, 21% had intracranial hemorrhage, and both infarction and hemorrhage occurred in 2%; mortality was reported in 17%. 19
Hemorrhage caused by Bothrops venom is mainly attributed to metalloproteases, which are potent and specific α-thrombin inhibitors that interact with plasma prothrombin and have an anticoagulant effect upon activation of the intrinsic pathway of blood coagulation.20,21 Other venom-activated coagulation factors are the XIII factors 22 and V. 23 Thus, the association of venom coagulant action with its activity on platelets and vascular endothelium could increase the risk of systemic bleeding, leading to serious hemodynamic complications 24 such as cerebrovascular hemorrhages. 25
Unclottable blood and thrombocytopenia upon admission of a patient with Bothrops envenomation have been independently associated with the development of systemic bleeding during hospitalization. 26 This fact corroborates the laboratory findings of the patient in this report who presented altered coagulation time (unclottable) during the first 48 h of admission and thrombocytopenia during 4 d. Platelets represent the first line of activation of hemostatic reactions through adhesion to the subendothelial surface when bleeding occurs. 27 However, intensity of coagulation dysfunction, bleeding, and local manifestations may differ in each patient because they are directly related to the composition and toxicity of snake venom, which varies between species and within the same species due to factors such as habitat, food, sex of the snake, and its ontogenetic stage. 28 –30
In both cases reported in our study, mild initial symptoms, as well as the use of traditional therapies, were the motivation for the delay in seeking care—an attitude that is frequent in many communities and often contributes to more adverse outcomes, including deaths or sequelae without notifications to the health system. 31 Delays in seeking hospital care and the subsequent occurrence of stroke was also observed in other reports regarding snakebites in the states of Amazonas in 2017 32 and Pará in 2013. 33
The action of the Bothrops antivenom begins upon its administration, neutralizing the toxins in the blood immediately and later in the tissues. Early serum therapy is a major factor in preventing complications such as bleeding, intense edema, kidney failure, and death. 34 However, even with early administration, irreversible and fatal situations may occur in relation to hemorrhagic complications; these complications may arise even if serum therapy is initiated only 2.5 h after a Bothrops snakebite in the Amazonas state. 11 It is imperative to reinforce the importance of administering the correct amount of antivenom according to the situation as quickly as possible; thus, severe cases, such as patients with evidence of shock, acute kidney injury, or severe bleeding, should be treated with 12 antivenom vials for effective neutralization of the effects of the venom.
The first case in our study was confirmed as being caused by Bothrops atrox via the antigenemia of the envenoming agent. This is the second known report of stroke related to this species in the literature. Due to the characteristics of the specimen (40 cm length and white tail tip), it was thought to be a juvenile, whose bites are more commonly associated with coagulopathy. 35 In the second case, as in most reports of stroke related to suspected Bothrops envenomations in the Amazon,11,32 identification was based on clinical and epidemiological characteristics; we can be reasonably certain that it was caused by Bothrops atrox, which is most commonly involved in snakebites in the Brazilian Amazon.3,30,35
As a limitation to the case study, there may have been a lack of data in the medical records that would better describe the clinical and laboratory evolution of the patient. However, communication with the professionals who attended the patient can minimize these gaps.
Conclusions
Two cases were described that presented with subarachnoid hemorrhage with hydrocephalus and hemoventricle after a snakebite caused by presumed Bothrops in a municipality of Amazonas state. Delay in seeking health care after snake envenomation can result in worse outcome because bites by Bothrops snakes can cause bleeding. Health campaigns that emphasize the importance of rapid hospital care in cases of snakebite are essential; delayed serum therapy may contribute to the emergence of complications, such as stroke, which may lead to death.
Footnotes
Acknowledgements
Author contributions: Study concept and design (JAGS, AMS, WMM, PSB); acquisition of the data (AMS, AWCBD, TRD); analysis of the data (JAGS, AMS, PSB, MC, AMMS); drafting of the manuscript (JAGS, AMS, AWCBD, TRD, WMM, PSB); critical revision of the manuscript (PSB, MC, AMMS, WMM); approval of final manuscript (JAGS, AMS, AWCBD, TRD, MC, AMMS, WMM, PSB).
Financial/Material Support: This work was supported by Fundação de Amparo à Pesquisa do Estado do Amazonas through PAPAC (Call number 005/2019). WMM is a research fellow of the Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq).
Disclosures: None.