
Abstract
Bear attacks, although rare, can inflict life-threatening injuries. We present the case of a 50-y-old woman from rural Pennsylvania who was attacked by a North American black bear, Ursus americanus. She sustained multiple complex injuries including near-complete scalp avulsion, bilateral ear avulsions, and fractures of the face, ribs, and pelvis. These injuries are similar to those sustained in other bear maulings reported in the literature and required both acute intervention and a multidisciplinary approach to recovery.
Introduction
The black bear, Ursus americanus, has both the largest population and largest range of North American bears. They are found across the United States and in all Canadian provinces and territories. Black bears are the smallest of North American bears, with weights typically ranging from 64 to 295 kg. They are omnivores, and approximately 5% of their diet consists of live prey. 1 North American black bears are considered less aggressive toward humans compared to other bear species, such as the brown bear (Ursus arctos, including its subspecies the grizzly bear, Ursus arctos horribilis), the polar bear (Ursus maritimus), or the Asian black bear (Ursus thibetanus). 1 -3 Encounters with black bears do not usually result in attacks or injuries, and most end with a defensive retreat by the bear.1,4 However, given the proximity of their habitat to populated areas, human–bear encounters are becoming increasingly common.1,4
Although reporting remains inexact, a review of data from all North American state and national parks between 1960 and 1980 reveals that 500 people were injured by black bears. 5 Ninety percent of these encounters resulted in only minor injuries. 5 This is lower than both the attack and injury rates from North American brown bears.6,7 When a black bear feels threatened, it may paw at the ground, make blowing noises, or make mock charges. 8 Attacks are generally classified into 1 of 3 categories: sudden (93% of reported cases), human provoked (7%), or predation (<1%). 1 Most bear attacks across species are associated with a sudden encounter with a female bear and her cubs.1,2 Although more frequent, these attacks are less often fatal compared to provoked or predatory attacks, which are usually committed by solitary males.1,2
The expansion of urban and suburban communities into black bear habitats has been an important variable in the increasing frequency of human-bear encounters. 4 Habituation to human food and the presence of domestic dogs have been factors in many bear attacks.1,7-10 Fatalities are infrequent; from 1900 to 2009, 63 deaths from North American black bears were reported, the majority of which were the result of predation by adult males. 8 According to Pennsylvania game commission records, there have been no known fatalities from wild black bear attacks in Pennsylvania and only 3 other nonlethal attacks since 2011. 11
Case report
A 50-y-old woman presented to the emergency department of a rural, quaternary care hospital via ambulance approximately 2 h after being attacked by a black bear. The patient had left her rural home to check on her dog in her backyard when she noticed it had been barking at an adult black bear. While attempting to fight off the bear, the 55 kg patient was dragged an estimated 60 m into the woods. The bear left her alone for several minutes, and despite her injuries the patient was able to return to her home and call emergency medical services. The prehospital team bandaged her nearly avulsed scalp, placed her in a cervical collar, established intravenous access, and transported her to the hospital.
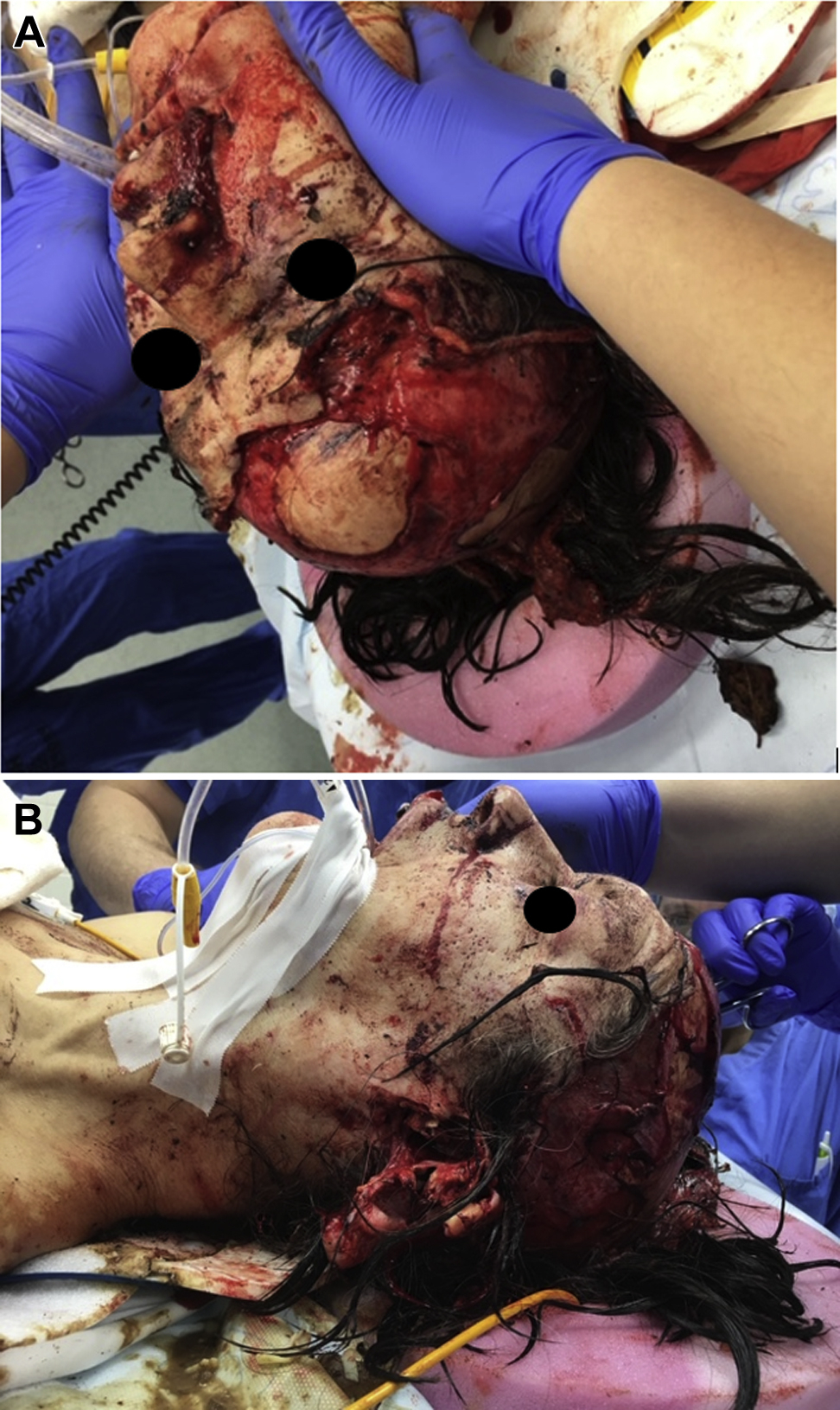
On arrival to the emergency department, the primary survey revealed significant craniofacial injuries, although there was no active bleeding or respiratory distress. The patient was alert, awake, and speaking in full sentences. She had normal oxygen saturation without supplemental oxygen. The secondary survey revealed a large anterior scalp avulsion with exposed cranium, bilateral ear avulsions, a complex lip laceration involving the vermillion border, and many lacerations and puncture wounds of various lengths and depths over the torso and extremities. The scalp wound was grossly contaminated with dirt. The periosteum was exposed, and there were multiple puncture and scratch wounds to the skull without associated fractures. Computed tomography imaging of her head, cervical spine, chest, abdomen, and pelvis and angiography of her neck vasculature revealed additional injuries (Table 1). The patient was given broad-spectrum antibiotics, tetanus vaccine, rabies vaccine, and immunoglobulin and was taken to the operating room that night. She was intubated fiber optically in the operating room, given the extent of her facial injuries. She underwent washout of her many wounds and initial closure of the scalp avulsion (Figure 1A and B).
Injury complex of patient
During the course of her hospitalization, she required 8 operations, including repair of complex lacerations to the lip, eyebrows, and ears, along with serial scalp debridements and skin grafting. Washout and closure of a thumb avulsion and operative reduction of a displaced clavicle fracture were also performed. The patient’s mandible, rib, and pelvic fractures were managed non-operatively. She was treated with 6 wk of intravenous vancomycin and cefepime for suspected cranial osteomyelitis secondary to the puncture wounds. Intraoperative and subsequent wound cultures were not collected. She also received the rabies vaccine series. The patient received evaluation and treatment from a critical care psychologist owing to concerns for acute stress disorder. She required extensive rehabilitation, including speech therapy, occupational therapy, and physical therapy. She was discharged home after being hospitalized for 55 d.
At 3-mo follow-up, the scalp graft and other facial injuries were healing well (Figure 2). The patient reported persistent lower extremity neuropathies that limited walking long distances, but otherwise she was back to her functional baseline. She did not report symptoms of posttraumatic stress disorder. The patient’s dog survived the attack after sustaining several rib fractures and superficial wounds. Local wildlife agents suspected the bear was an adult female that had been seen in the area with several cubs; attempts to locate and trap the offending bear with tracking dogs and traps were unsuccessful.

Patient at 3-mo follow-up with plastic surgery with healing scalp with graft.
Discussion
Victims of bear attacks can present with multiple severe and complicated injuries requiring prolonged hospitalizations and multidisciplinary care. As with any major trauma, patients presenting after a bear attack should be assessed for their ability to protect their airway and for major sources of hemorrhage or vascular injury. A retrospective study of attacks by Ursus thibetanus indicated that of 21 patients, over half required some form of emergency airway management including intubation or surgical airway. 12 Hemorrhage control is critical during initial resuscitation.13,14 Although fatalities from bear attacks after presentation to the hospital are rare (2% in 1 retrospective review of 417 cases), 3 exsanguination is the most common cause of death. 7 In 1 case series, major vascular trauma occurred in 7% of Ursus thibetanus attacks, with injuries including femoral, popliteal, brachial, and carotid arteries. All of those injuries required surgical intervention. 15 Cervical spine injuries have only been reported in 2 cases14,16 and rates of cervical spine injuries in bear attacks are noted to be lower than in attacks by other large carnivores. 17 Bear attack victims presenting with multiple or complex traumatic injuries should be transferred to a trauma facility once they are stabilized. 2
Other injuries from bear attacks may include a combination of puncture, avulsion, and crush injuries from powerful jaws, sharp teeth, and long claws.1,2,18 Craniofacial injuries may include skull fractures and associated intracerebral hemorrhage, many of which are fatal. 19 Maxillofacial and scalp injuries are common, as seen in this case, and include damage to the ears, nose, mandible, and eyes. 14 -16,19-26 Injuries to the face and jaw occurred in 81% of cases and injuries to the scalp in 55% of cases in 1 retrospective review. 3 Complex surgical repairs, including reconstruction with skin flaps or skin grafts, are required in 25% of patients presenting with craniofacial injuries. 23
Bear attack victims may present with extremity fractures as well. Upper extremity injuries (notably humerus, clavicle, and forearm fractures) are more common than lower extremity injuries, 27 particularly when victims protect their face with their arms. 28 In 2 cases comparing attacks by North American black bears (Ursus americanus) and brown bears (Ursus arctos), there was a slightly higher incidence of lower extremity injuries in black bear attacks compared with attacks by Ursus arctos.6,29 Asian black bears (Ursus thibetanus) and Ursus arctos have longer claws, are more facile at walking on 2 feet, and are noted to be more aggressive, with a higher incidence of reported attacks compared to Ursus americanus.1,3,26,27 Despite these differences, the overall injury complex across all species appears to be similar, and further studies are needed to delineate any other possible differences due to each species’ behaviors or anatomy.
Wounds from bear attacks are considered contaminated at a minimum and dirty if an infection develops. 30 Skin and soft tissue infections14,24,27,29 and osteomyelitis 31 have been reported in patients hospitalized after bear attacks. Studies of microbes associated with infected wounds from bear injuries and oral flora found in bears have found organisms common to other bite injuries (cat, dog, human) with a predominance of aerobic bacteria. 32 -34 Thorough irrigation for all wounds and debridement of crushed or devitalized tissue is recommended on initial presentation.14,35 Wound cultures of new injuries without signs of active infection are not recommended because diagnostic yield is low.35,36 Injuries sustained in bear attacks are particularly prone to infection given extensive crush, puncture, and avulsion injuries and associated tissue necrosis.14,24,27,29
Guidelines recommend high-risk soft tissue wounds be treated prophylactically with amoxicillin-clavulanate as first line agent.35,37,38 High-risk wounds include deep puncture wounds, complex crush wounds, wounds over vital structures, wounds to the distal extremities, and wounds with exposed bone or over joints. 35 Soft tissue injuries in immunocompromised patients and patients at extremes of age and wounds with delayed evaluation are also considered high risk for infection. 35 These and other types of wounds may be considered poor candidates for primary closure and require surgical consultation.35,36 Providers should consider the possibility of underlying osteomyelitis when choosing the initial antibiotic regimen; however, data on treatment of osteomyelitis from animal bite wounds are limited.31,39,40
Although black bears are not the most common vector of rabies, cases have been reported in several US states and Canada. 41 -43 The US Centers for Disease Control and Prevention (CDC) recommend rabies immunization for victims of wild carnivore attacks. 44 The CDC also recommend tetanus vaccination for wounds if the patient is unvaccinated, is unsure about vaccination status, or has not completed the tetanus vaccination series; if the most recent tetanus immunization or booster was more than 5 y prior to the injury, another booster is indicated. 45 Tetanus immunoglobulin is reserved for those who have not completed the 3-vaccine series or are unvaccinated. 45
After initial stabilization and treatment of acute injuries, many bear attack victims face prolonged hospitalizations3,14,29 with chronic sequelae such as psychiatric illness or long-term disabilities. Although data are limited, several case reports of bear attack victims have shown patients develop symptoms consistent with acute stress disorder14,26,29 and may later develop posttraumatic stress disorder. 29 Chronic neuropathic pain and neuropraxias limiting daily function have also been reported in multiple case series, as was reported in follow-up with this patient.15,26,27
Prevention is key in avoiding bear attacks both in the wilderness and in developed environments.1,2,4,9 Many resources highlight specific practices to avoid bear encounters in the backcountry.1,2,46 Several retrospective field studies have shown that capsaicin spray is an effective deterrent in attacks.47,48 If the offending animal is captured, relocation and monitoring are common practices employed by many wildlife agencies, with variable success. 49
Conclusions
Our case highlights the life-threatening and complex injuries of an attack by Ursus americanus as consistent with those by other bear species reported in the literature. Bear attack victims may require early and aggressive resuscitation and stabilization as well as significant resources in both the acute and long-term care of their injuries. Further studies on these injuries will be key to improving the care of these patients and providing a better understanding of bear behavior and prevention of future attacks.
Footnotes
Acknowledgements
Acknowledgments: Appreciation is extended to Chadd Kraus, DO for insightful comments regarding the clinical case and report.
Author Contributions: Acquisition of case data and analysis of case data (MC, TDS); drafting of case and overall manuscript (MC, TDS); critical revision and approval of final manuscript (MC, TV, MF, TDS).
Financial/Material Support: None.
Disclosures: None.