
Abstract
Introduction
Cricothyroidotomy is an advanced and life-saving technique, but it is also a rare and a difficult procedure. The purpose of the present study was to produce a low-cost simulation model with realistic anatomic features to investigate its effectiveness in developing cricothyroidotomy skills.
Methods
This study was performed at a university simulation center with 57 second-year student paramedics and a cricothyroidotomy simulation model. Total scores were assessed using a checklist. This consisted of 13 steps and was scored as misapplication/omission=0, correct performance and timing with hesitation=1, and correct performance and timing without hesitation=2. One of these steps, local anesthesia of the area if time is available, was not performed owing to time limitations. The highest possible score was 24. Data are presented as mean±SD with range, as appropriate. Normal distribution was evaluated using the Kolmogorov-Smirnov test, Student
Results
Students completed the cricothyroidotomy procedure steps in 116±46 (55–238) s. At performance assessment, the score achieved was 12±5 (2–24). The highest total score of 24 was achieved by 3 students (5%). Total scores exhibited negative and significant correlation with procedure time (r=−0.403,
Conclusions
The model developed in this study is an inexpensive and effective method that can be used in cricothyroidotomy training for student paramedics. We think that repeating the cricothyroidotomy procedure on the model will increase success levels.
Introduction
Airway management represents a prime component of resuscitation. Paramedics and other advanced medical providers use either basic or advanced airway techniques to provide ventilatory support. However, these airway procedures may not always be employed successfully. Supraglottic or fiber optic devices may be employed in some critical cases; if these fail to effectively ventilate and oxygenate the patient, surgical cricothyroidotomy may need to be considered. 1 Cricothyroidotomy is an invasive surgical technique involving an incision through the cricothyroid membrane. 2 This is a life-saving technique that permits ventilation, particularly in patients who cannot be ventilated with endotracheal intubation, which is the clinical standard airway procedure.2,3 Wilderness medicine shares many common topics and procedures with emergency medicine, especially in prehospital emergency care. 4 Wilderness medicine doctors’ cricothyroidotomy skills are very important to patient survival in cases in which there is no equipment to provide airway clearance in austere conditions. Improving cricothyroidotomy skill is of vital importance in wilderness medicine and in emergency medicine.
Devices developed to establish an airway have reduced the frequency of cricothyroidotomy procedures.5,6 Although the reported prevalence of surgical airway opening ranges between 0 and 19%, the true rate is unclear. 7 Additionally, the incidence of cricothyroidotomy in prehospital emergency interventions is approximately 10 times higher than that in emergency departments. 8 The majority of situations requiring prehospital cricothyroidotomy are trauma related, although cricothyroidotomy may also be required in some nontraumatic situations such as fascial muscle spasm, laryngospasm, upper airway narrowing, laryngeal and oral edema, and lack of visibility due to blood and vomit despite suctioning. 3
Cricothyroidotomy generally has a high success rate, ranging between 89 and 100%, 8 –10 although this can be lower in prehospital emergency situations as a result of light and background noise or situations in which patients are trapped. 11 The incidence of short-term postcricothyroidotomy complications (bleeding, laceration of cartilage tissues, perforation of the trachea, creation of a false tract, or infection) is 32% and that of long-term complications (eg, subglottic stenosis, voice changes) is approximately 8%. 2 It is therefore highly important for health workers providing emergency services to be able to perform the procedure.
Simulation is a method with proven effectiveness in the acquisition and development of clinical application skills by health workers. 12 Many commercial airway simulators with either low- or high-fidelity simulation nevertheless exhibit inferior airway anatomy. The use of a sheep trachea may therefore be superior to many commercial airway simulators because sheep anatomy closely resembles the human anatomy. The purpose of this study was to develop a low-cost simulation model intended for the acquisition of cricothyroidotomy application skills and to assess the effectiveness of that model.
Methods
The study was performed in April 2019 at the Acibadem Mehmet Ali Aydinlar University simulation center, Turkey. Inclusion criteria were willingness to participate in the study, no prior education on cricothyroidotomy, and no previous experience with performing cricothyroidotomy. The study included 57 student paramedics who met the inclusion criteria and were studying at the Acibadem Mehmet Ali Aydinlar University vocational school of health services. The study protocol was approved by the Acibadem Mehmet Ali Aydinlar University medical research ethical committee (ATADEK-2019/3).
Our aim was to produce an effective and low-cost simulation model. This was done using Styrofoam, a sheep trachea, and a double-layer of chicken skin. Sterile gloves, a scalpel, a scalpel handle, a hook, an endotracheal tube, sponge, syringe, and antiseptic solution were used in carrying out the procedure. The first step involved producing the simulation model using Styrofoam, a modeling knife, glue, pencils, several nails, chicken skin, and a sheep trachea. The profile of a human head and neck was first drawn on 2 cm Styrofoam and cut out with a modeling knife for use as a template. Four separate templates were produced in this way and then combined. A central incision was made in 2 of the templates where the sheep trachea was to be inserted. Styrofoam supports were placed on the sides of this model and affixed with glue. The sheep trachea was installed in the cavity made in the Styrofoam, and 2 layers of preprepared chicken skin were then placed over the trachea. The chicken skins were then attached with nails. The skins were used in a double layer to simulate cutaneous tissues (Figure 1) and were replaced after every 3 or 4 cricothyroidotomy applications. The preparation of the model lasted approximately 60 min, and cost US $10.
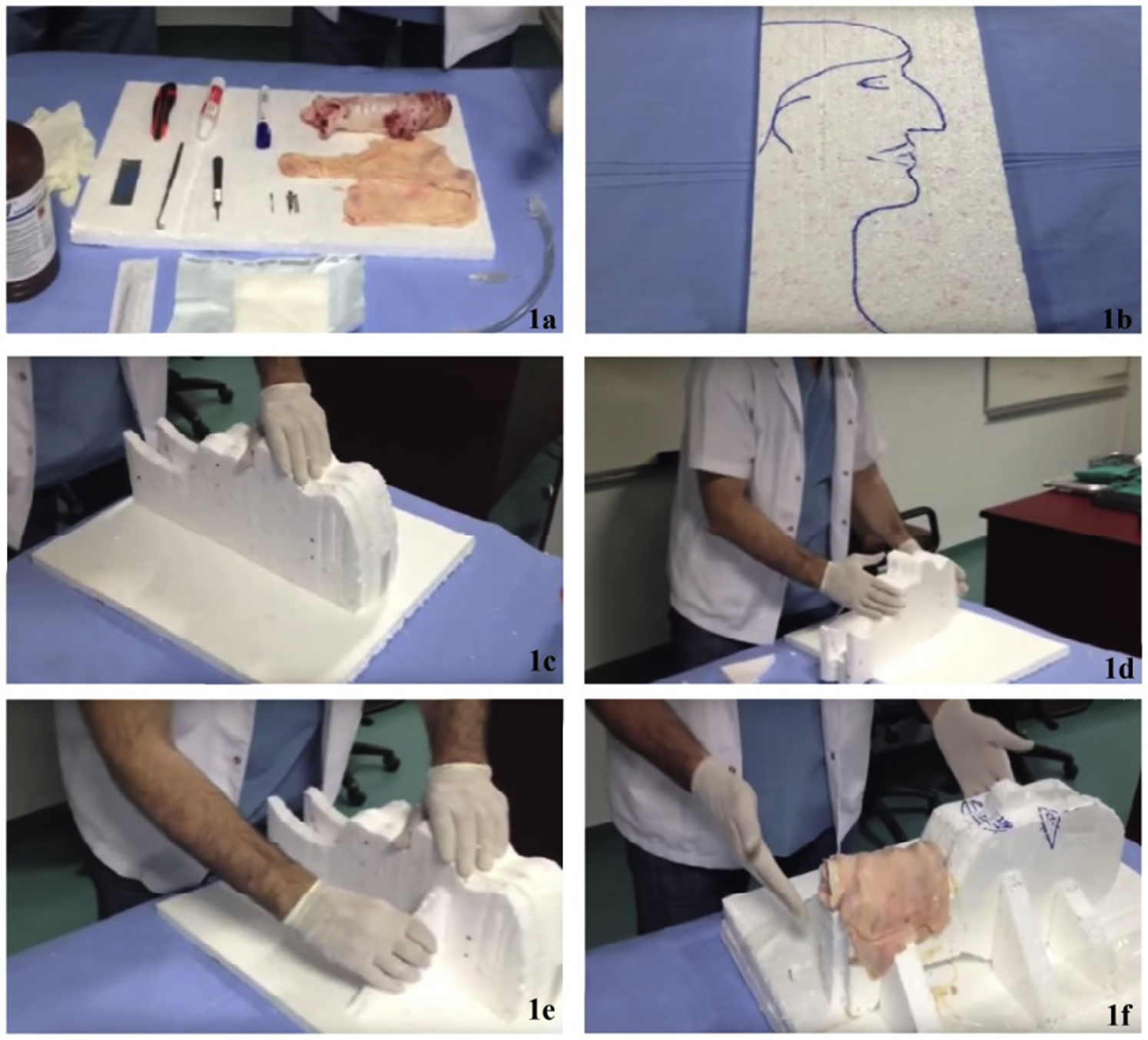
Preparation of biomaterial-covered simulation model.
An emergency medicine resident and 2 emergency medicine assistant professors prepared a video showing the cricothyroidotomy procedure step by step as part of the training program. 13 Because 1 of the physicians involved in the training also had video production experience, no costs were incurred for the video recording. The video was shown to students after an interactive presentation regarding airway and cricothyroidotomy. During the interactive presentation, students were informed about cricothyroidotomy indications, potential complications, and how the procedure should be performed.
Students subsequently performed the cricothyroidotomy procedure on the model. All performances were video recorded without the students’ faces being visible. An emergency medicine assistant professor was blinded to names and personal data and evaluated performances. Cricothyroidotomy skills were assessed on the basis of the criteria in the cricothyroidotomy skills checklist (Table 1). Each item on the checklist was scored separately. Any step that was missed or performed incorrectly was scored as zero. Procedural steps performed at the correct time and in the correct manner, but involving a pause after the previous step, received a score of 1; those performed at the correct time and in the correct manner, without hesitation, received a score of 2. Total scores were calculated by adding the scores awarded for all the procedural steps. The second skin in the simulator was intended to simulate the cricothyroid membrane. Both skins were changed to allow each student to have the same experience. We have used methods different from the simulation model for this purpose in previous studies. 14 However, owing to the inexperience of the students, the procedure steps were detailed in a step by step manner based on the standard surgical method.
Cricothyroidotomy skill checklist used in the study
Participants’ age, sex, cricothyroidotomy skills checklist scores, and data concerning procedure application times were recorded. The study data were analyzed using IBM SPSS (Armonk, NY) for Windows v23.0 software. Descriptive statistics were expressed as number and percentage. Compatibility with normal distribution was assessed using the Kolmogorov-Smirnov test. Correlation between total scores obtained and procedural times were analyzed with Spearman correlation test. When comparing the total score by sex, the Mann-Whitney U test was used; the Kruskal-Wallis test was used to compare total scores by type of high school attended. Data are presented as mean±SD with range, as appropriate.
Results
The study was performed with 57 student paramedics. Student age was 20±1 (19–25) y. Thirty-one students (5%) were men and 26 (46%) were women. No students were currently working or previously worked in an emergency department or ambulance service. Participant demographic data are shown in Table 2.
Demographic characteristics of the study population
Time to completion of the procedure was 116±46 (55–238) s. A significant negative correlation was observed between total score and procedural times (r=−0.403,
The procedural step performed correctly by all students was “equipment preparation,” the first step in the checklist. The procedure successfully performed by the next largest number of students (n=48) was the cuff inflation stage. The step with the lowest success rate was the insertion and rotation of the scalpel handle (Table 3).
Procedural step skills (n=57)
Discussion
Cricothyroidotomy is a technique generally applied as the final option in individuals at severe risk of mortality in whom endotracheal tube placement cannot be achieved or is contraindicated. It is therefore less commonly used in the clinical setting than other airway management techniques. 7 Simulation models are produced and used to allow health workers to acquire rapid and correct cricothyroidotomy skills.15,16 This study evaluated paramedics’ cricothyroidotomy skills using a low-cost simulation model and video instruction.
Cricothyroidotomy models can be created using various materials, including organic tissue, fully synthetic materials, and technological products. The most important features of the simulation models produced for this purpose is that they should be easy to prepare and affordable. 7 We think that our model is both cost effective and time efficient. Another study developed a synthetic model capable of bleeding. The authors reported that this model exhibited a high degree of structural and functional applicability and that it was more realistic than the porcine and cadaver models they had previously employed. 17 Another study compared a model made from simple inorganic materials with a synthetic model possessing anatomic features closer to reality. Those authors reported that their participants observed no difference between the models in terms of realism and practicability. 18 Other researchers compared a model developed out of edible products such as chocolate and fruit with synthetic and organic models. They concluded that the procedure took longer to perform with the edible model and reported that the most popular model among their participants was the organic model, followed by the edible model. 19 In the present study, we used a sheep trachea to create a model resembling human tissues and anatomy. Our model was produced from low-cost materials and can be prepared in 60 min. It was also designed to permit repetition of the procedure.
The rate at which cricothyroidotomy is performed for airway management in hospitals is less than 1%. 20 Prehospital cricothyroidotomy is more common. One previous study examined the ambulance and hospital records for trauma patients undergoing emergency cricothyroidotomy by paramedics in the ambulance and determined that surgical cricothyroidotomy was performed on 10% of patients requiring intubation. 14 Another study examining the records for 78 medical teams transporting patients by air reported that 4800 patients were intubated and that cricothyroidotomy was performed in only 0.7% of these. 21 The incidence of cricothyroidotomy has been decreasing in recent years. The gradual decrease in the application of cricothyroidotomy is associated with the dissemination of advanced airway management training, rapid application of consecutive intubation programs, and technological advances in airway devices. 3 However, this decrease in the rate of cricothyroidotomy performed by paramedics does not mean that there is no need to acquire the skill. Health workers with the lowest use of surgical airway skills in fact have the greatest need for frequent training.3,20
Because cricothyroidotomy is a lifesaving intervention, the duration of the procedure is of considerable importance. In their study involving medical and dental students and individuals who had only heard about cricothyroidotomy through the media, Braun et al reported that 80% of participants performed the procedure successfully in a mean time of 243 s. 22 A study involving shop window manikins with different anatomic characteristics reported a mean application time of 74 s. 23 Another study investigated the effect of the traditional model and of the 4-step simulation method developed by Peyton on cricothyroidotomy skills. 16 Procedure times were 114±40 s in the traditional method group and 105±41 s in the 4-step method group. 16 The procedure time in the present study was 116±46 s. This shows that our training method yields results similar to the traditional simulation method. The study results also show that the procedure time depends on the knowledge of the performer, the method used, and the patient’s anatomic characteristics.
One previous study determined that medical students scored 2±1 out of 5 after simulation manikin training. 24 The score out of a possible 24 in the present study was 12±5 (2–24). The different characteristics of the models used in previous studies may account for the variation in findings. We attribute the higher scores achieved by our students to the educational material being supported by video recordings.
Another study indicated that repetition (at least 5 times) is essential to successfully perform a cricothyroidotomy in an acceptable length of time. However, in the current study, each student only performed the procedure on the model once. In addition, students had no previous experience in cricothyroidotomy. The scores achieved in this study might be improved further if each student were to perform the procedure several times. 25
Sixty-three percent of medical students in a study exhibited the ability to open an incision, but none successfully managed to widen the incision with a clamp. Thirty-six percent of medical students in that study managed to insert the endotracheal tube. 24 In the present study, 60% of students displayed the ability to make the incision, and 30% managed to widen the incision with a clamp. In addition, 81% of students managed to insert the endotracheal tube. That study simulated the larynx, trachea, and cricoid cartilage using materials such as cardboard and Styrofoam. 24 In the present study, however, the simulation model was created using organic tissues. The differences in success rates between the 2 studies may be due to differences between the models in terms of genuine tissues and realism levels. In addition, that study also included health workers with previous training on the subject, and their success rates for the same steps were significantly higher than the success rates achieved by the students. 24 In our study, students were prepared for the procedure through theoretical instruction and video presentations before application. These results show that in addition to its resemblance to actual anatomic structures, the model used in simulation training can also have a positive effect on the participant’s knowledge of the procedure and training outcomes.
Limitations
The study shows that the simulation model described is well designed and that all 13 steps can be successfully performed using it, although greater skills preparation is needed to achieve a much higher level of skill in this invasive surgical procedure. The fourth of the 13 procedural steps was defined as “application of local anesthesia to the area if sufficient time is available.” The students remembered this step but skipped it owing to lack of time. This step was therefore excluded from the evaluation. Another limitation of this study was that students’ knowledge levels before and after training was not measured and compared. In addition, potential complications that may develop in association with the cricothyroidotomy procedure cannot be simulated using this model. Another limitation of the present study was that students performed the procedure only once. The literature indicates that at least 5 trials must be done to successfully perform the procedure; we attribute the low scores achieved by some students to this factor. The lack of power analysis to determine the sample size and the lack of objective assessment tools are other limitations of this study.
Conclusions
Developing an easy-to-apply model for training in cricothyroidotomy will both increase the effectiveness of training and enable students who cannot access advanced simulation practices to undertake this training. The simulation model—which uses Styrofoam, a sheep trachea, and a double layer of chicken skin—employed in this study is inexpensive and simple to apply. The designed simulation model is unique, and our findings show that it can be usefully employed in the training of student paramedics. We concluded that the 13 steps can be performed and learned using this novel simulation. However, it seems that the teaching procedure used in this study among inexperienced paramedics does not prepare them well for achieving a high success rate in such a surgical airway procedure. In this study, students were allowed only 1 attempt on the simulation model. We think that the success level could be increased significantly by repeating the cricothyroidotomy procedure on the model. This study should now be repeated using the same model with a larger student sample, and participants’ opinions regarding the positive and negative aspects of the model should also be investigated.
Footnotes
Acknowledgements
Author Contributions: Study concept and design (OSC); acquisition of the data (YS, KK); analysis of the data (SP); drafting of the manuscript (OSC, SP, TO); critical revision of the manuscript (TS); final approval of manuscript (COS, SY, KK, HA, CG, PS, OT, ST).
Financial/Material Support: None.
Disclosures: None.