
Abstract
Objective
General anaesthesia with tracheal intubation results in sore throat. We evaluated the influence of the two-handed jaw thrust on postoperative sore throat in patients who require tracheal intubation.
Methods
In this prospective, double-blind, single-centre, parallel-arm, and randomised trial, 92 patients who were scheduled for general anaesthesia for total hip arthroplasty were allocated to one of two groups. In the jaw thrust group (n = 46), the two-handed jaw thrust manoeuvre was applied at intubation. In the control group (n = 46), conventional intubation with sham jaw thrust was performed. Incidences of airway morbidities including sore throat, hoarseness, and cough at 2, 4, and 24 hours postoperatively were compared.
Results
During the postoperative 24 hours, the incidence of sore throat (8 [17%] vs. 20 [44%]) and hoarseness were lower in the jaw thrust group (8 [17%] vs. 18 [39%]) compared with the control group. The incidence of cough during the postoperative 24 hours was similar between the groups.
Conclusions
The jaw thrust manoeuvre significantly reduced sore throat and hoarseness in patients after general anaesthesia using tracheal intubation.
Clinical trial registration: NCT 03568279.
Introduction
Tracheal intubation causes airway damage, which results in sore throat after general anaesthesia1–3 and increases patients’ complaints. 4 Various pharmacologic or non-pharmacologic preventive modalities have been investigated to reduce postoperative sore throat. Interventions such as thermal softening, dexamethasone, ketamine gargle, and sevoflurane inhalation have been reported to prevent postoperative sore throat.3–6
The risk factors for postoperative sore throat are female sex, younger age, lung disease, duration of anaesthesia, and the presence of a blood-stained tracheal tube. 7 Traumatic injuries to the larynx and hypopharynx are associated with a sore throat. 8 A meticulous insertion technique for the endotracheal tube is important to prevent airway injury and sore throat.
Two-handed jaw thrust manipulation elevates the epiglottis and tongue base away from the posterior pharyngeal wall, enlarging the laryngeal aperture.9,10 A previous investigation demonstrated that jaw thrust that is applied during double-lumen endobronchial intubation decreased the incidence of sore throat and airway injuries. 11 Whether the jaw thrust manipulation prevents postoperative sore throat in patients undergoing conventional tracheal intubation using a laryngoscope has not yet been determined.
We hypothesised that tracheal intubation using a laryngoscope facilitated by two-handed jaw thrust manipulation may reduce airway morbidities including sore throat, hoarseness, and cough compared with conventional intubation using a laryngoscope. We aimed to evaluate the efficacy of jaw thrust that was applied by an assistant, on sore throat, hoarseness, and cough in patients following conventional tracheal intubation for general anaesthesia.
Methods
This study was a prospective, double-blind, single-centre, parallel-arm, and randomised trial. Ethics committee approval was obtained from the Ethics Committee at Keimyung University in Daegu, Korea (Document no.: 2018-06-004). This study was registered at ClinicalTrials.gov (NCT 03568279). Written informed consent was obtained before enrolment. Patients with American Society of Anaesthesiologists (ASA) physical status (ASA-PS) I to III and who were 19 to 80 years old and scheduled for orthopaedic hip arthroplasty were enrolled from October 2018 to February 2019. Patients with a recent history of sore throat, upper respiratory infection, fragile teeth, a Mallampati grade >2, anticipated difficult airway, previous head and neck surgery, cervical spine disorder, recent analgesic administration, and multiple intubation attempts were excluded from this investigation. Multiple intubation attempts were defined as two or more laryngoscopic attempts. Randomisation was accomplished using the Random Allocation Software (ver. 1.0.0; Isfahan University of Medical Sciences, Isfahan, Iran). Patients were assigned to either the jaw thrust group or the control group using the closed envelope technique.
Study procedures
Upon arrival in the operating room, patients were monitored using non-invasive blood pressure measurement, electrocardiography, and pulse oximetry. Quantification of the neuromuscular blockade was performed using acceleromyography (TOF-watch SX; MSD BV, Oss, the Netherlands) and the depth of anaesthesia was assessed using a bispectral index monitor (A-2000 XP; Aspect Medical Systems, Newton, MA, USA). After pre-oxygenation, anaesthesia was induced by injection of propofol (2 mg/kg) and remifentanil (1 μg/kg). Rocuronium (0.8 mg/kg) was administered to support tracheal intubation while monitoring train-of-four (TOF) counts at the ulnar nerve. Before endotracheal intubation, we ensured the TOF count was ‘0’ to confirm that muscle relaxation was sufficient.
In the jaw thrust group or the control group, jaw thrust manipulation or sham jaw thrust manipulation, respectively, was executed from the insertion of the laryngoscope blade into the patients’ mouth until the vocal cords were in position between two depth marker indicators on the endotracheal tubes. 3
The anaesthesiologist who performed intubations was blinded to both the sham jaw thrust and the jaw thrust manoeuvre by placing a cover behind the patient’s mandible and bottom lip. On the basis of previous reports,12,13 the jaw thrust manoeuvre was performed by an anaesthetist other than an intubator. We decided to add an assistant to execute the jaw thrust manoeuvre while intubation was being performed. When the intubator was ready, she first turned around with her back to the patient while an assistant either applied sham jaw thrust or jaw thrust manoeuvre to blind the intubator.
The assistant applied the jaw thrust manipulation as follows: 12 the assistant stood by the left side of the patient’s body facing the anaesthesiologist who performed tracheal intubation; the assistant placed her fingers at the posterior aspects of the mandible and thrusted upwards; and the assistant then opened the patient’s mouth using her thumbs. The sham jaw thrust was performed as follows: the assistant placed her fingers behind the patient’s mandible angle without thrusting the mandible upward and opened the mouth using her thumb.
A single anaesthesiologist intubated all tracheas via a direct laryngoscope in both groups. Macintosh 3 or 4 blades (Minneapolis, MN, USA) were used. When the glottic view was poor, the anaesthesiologist who performed intubation requested backward, upward, and rightward pressure (BURP). The assistant nurse standing by the right side applied BURP to facilitate the intubation. A soft, seal cuff sterile polyvinyl chloride endotracheal tube with a standard cuff (Unomedical, Kedah, Malaysia) with an internal diameter of 7.0 for women and 7.5 mm for men was inserted and the tracheal tube cuff was inflated with air. An endotracheal tube was lubricated with sterile normal saline. End-tidal capnography confirmed the tracheal placement. The cuff pressure was maintained at 20 mmHg intraoperatively using a cuff pressure manometer (VBM Medizintechnik, Sulz, Germany). A bite block was not applied. After the patient’s position (left or right lateral decubitus position) was changed for surgery, auscultation, capnography, and cuff pressure were rechecked to confirm the location of the endotracheal tube. Anaesthesia was maintained using sevoflurane inhalation and continuous infusion of remifentanil. Remifentanil was started at a rate of 0.05 μg/kg/minute and increased or decreased by 0.05 μg/kg/minute based on clinical demands. The depth of anaesthesia was controlled to adjust the bispectral index to within 40 to 60 and the mean blood pressure within ±20% of the baseline values. The average concentration of intraoperative remifentanil was checked and compared. After skin closure and wound dressing, pyridostigmine (0.3 mg/kg) and glycopyrrolate (0.01 mg/kg) were infused to reverse residual neuromuscular relaxation while monitoring the TOF count. Ramosetron (0.3 mg) was injected to prevent postoperative vomiting and nausea. Gentle suction was applied at the oropharynx to prevent aspiration and tissue trauma. The trachea was extubated after adequate reaction to verbal commands, and spontaneous breathing and the TOF ratios were confirmed. Perioperative steroids were not infused to prevent postoperative infection.
The postoperative pain management protocol included infiltration of ropivacaine HCl and morphine as well as additional rescue medications. 3 Morphine (5 mg) was infiltrated at the muscular layer and ropivacaine HCl (150 mg; total volume, 100 mL) was infiltrated at the wound. Pethidine (25 mg) was injected at the start of skin closure. Postoperative wound pain at rest was evaluated using an 11-point verbal numerical rated score (0 [no pain] to 10 [worst possible pain]). We infused additional analgesics including diclofenac, pethidine, or tramadol for moderate-to-severe pain (pain scores, 4–10). When patients complained of moderate-to-severe pain, diclofenac (75 mg) was injected. When the pain did not acceptably subside (pain score, 4–10) and patients requested supplemental analgesics, pethidine (25 mg) was also infused. Tramadol (50 mg) was infused when the pain did not decrease after application of diclofenac and pethidine (pain score, 4–10).
Measurement of variables
The blinded anaesthesiologist assessed the Mallampati grade before surgery. The anaesthesiologist who intubated patients evaluated the glottis view using the Cormack–Lehane grade and percentage of glottic opening score, which corresponds to the percentage of the glottis that was visualised. 14 The percentage of glottic opening score ranges from 0% to 100%. 14 The time from the insertion of the laryngoscope blade into the mouth until the end-tidal CO2 was >30 mmHg was defined as the time-to-intubation. The hemodynamic variables including heart rate and mean arterial blood pressure were checked immediately before tracheal intubation and at 2 minutes afterwards. The blinded investigator assessed incidences of airway morbidities including sore throat, hoarseness, and cough at postoperative 2, 4, and 24 hours. Sore throat was evaluated while resting using a four-point system (severe, moderate, mild, or none), which was defined as follows: severe sore throat (hoarseness or change in voice that was considered to be throat distress); moderate sore throat (patient-volunteered complaints of sore throat); mild sore throat (complaints of sore throat reported only after enquiring); and none. If a patient presented with mild to severe sore throat (at any postoperative hour), the patient was considered to be positive for experiencing postoperative sore throat symptoms. The overall incidence of postoperative sore throat was defined as the number of patients who presented with any range of sore throat symptoms during any investigational postoperative time period. Sore throat severity was also assessed using a numerical rated score (0, no throat discomfort; 100, worst possible throat discomfort) at postoperative 2, 4, and 24 hours. 3 Hoarseness was recorded on a four-point system (severe, moderate, mild, or none), which was defined as follows: severe hoarseness (severe change in the quality of voice as assessed by the examiner); moderate hoarseness (moderate change in quality of speech of which the patient also complained spontaneously); minimal hoarseness (minimal change in quality of speech of which the patient complained only on enquiry); and none. Postoperative cough was assessed on a four-point system (severe, moderate, mild, or none), which was defined as follows: 3, severe cough (more severe than noted with a cold); 2, moderate cough (similar to that noted with a cold); 1, mild cough (less than that noted with a cold); and none. Jaw discomfort was evaluated using the following two-point system: yes or no. Postoperative pain scores were evaluated using a visual analogue scale (0, no pain; 100, worst conceivable pain).
The primary endpoint was the incidence of sore throat during the postoperative 24 hours. Secondary endpoints were hoarseness, cough, and jaw discomfort during the postoperative 24 hours and wound pain at postoperative 2, 4, and 24 hours.
Statistical analysis
A previous study showed that the incidence of sore throat was 44% during the postoperative 24 hours following tracheal intubation for general anaesthesia. 3 The jaw thrust manoeuvre was presumed to reduce the incidence of sore throat to 14%, and this was regarded as clinically significant. Thirty-five patients were needed in each group to achieve 80% power, and an alpha of 5% in a two-sided test. Forty-six patients per group were needed to compensate for a possible dropout rate of 10%, and a compliance rate of 95%.
Categorical variables including sore throat, hoarseness, cough, and jaw discomfort were analysed using the Chi-squared test or Fisher’s exact test when necessary. Continuous data were checked for a normal distribution using the Kolmogorov–Smirnov test. The Student’s t-test or Mann–Whitney U test was applied depending on the distribution of the variables. We used IBM SPSS Statistics software (ver. 22.0; IBM Corp., Armonk, NY, USA) to conduct statistical analyses. A p value of less than 0.05 was considered to be a statistically significant difference.
Results
One hundred patients were screened from October 2018 to February 2019. Among them, eight patients were excluded, including two patients for previous head and neck procedures, three patients for Mallampati grades >2, and three patients for recent sore throat. Ninety-two patients were randomised and included in the final analysis (Figure 1). The baseline characteristics of patients were comparable in both the jaw thrust and control group (Table 1). The average age of patients in the jaw thrust group was 63 ± 12 years, and 22 were women while 24 were men. The average age of patients in the control group was 61 ± 10 years, and 26 were women while 20 were men. All intubation attempts were successful the first time in both groups. A gum-elastic bougie or stylet was not used in every patient.
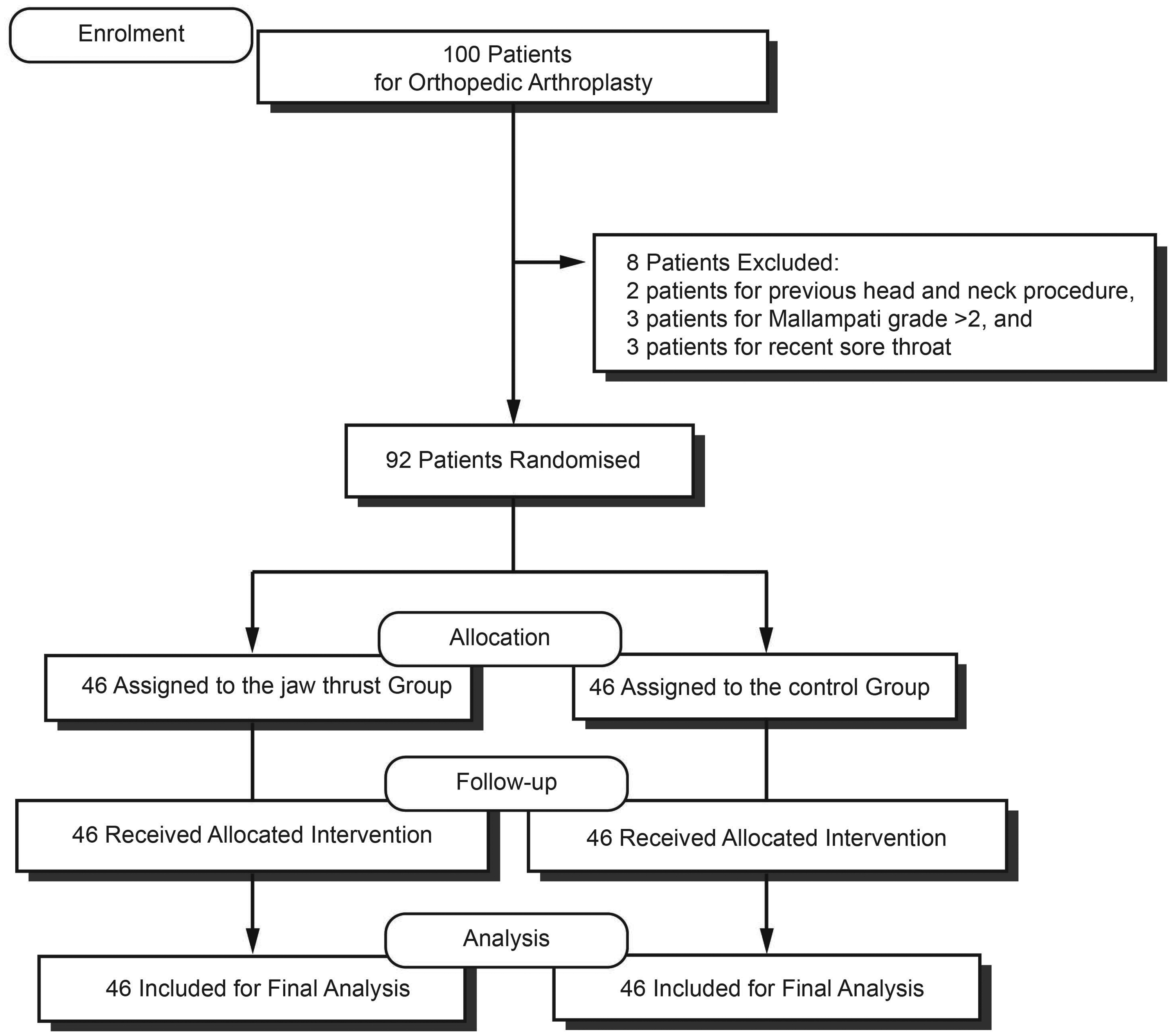
CONSORT diagram.
Patient and anaesthetic characteristics.
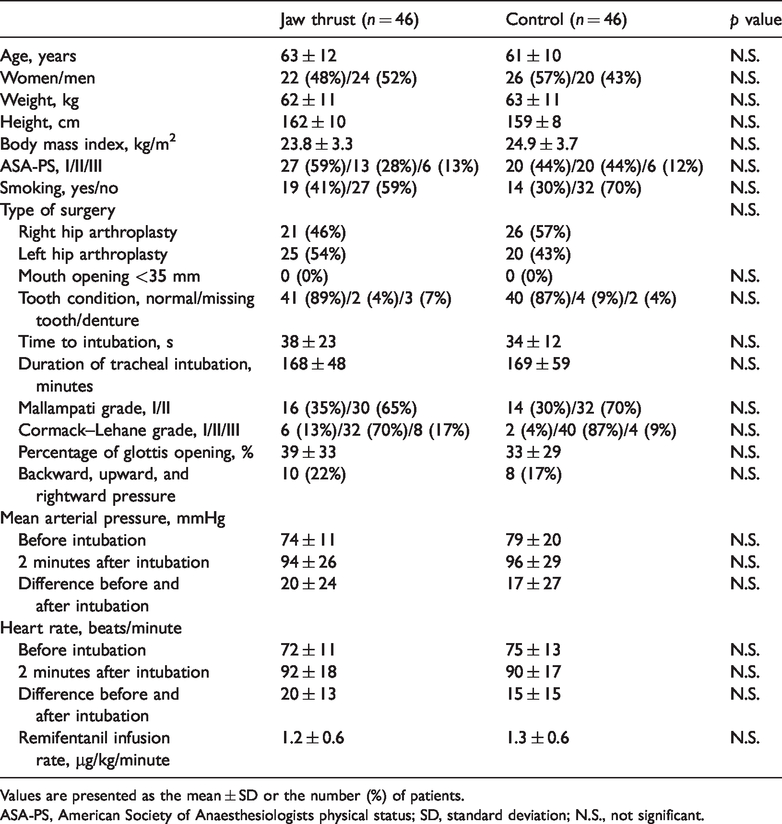
Values are presented as the mean ± SD or the number (%) of patients.
ASA-PS, American Society of Anaesthesiologists physical status; SD, standard deviation; N.S., not significant.
Overall postoperative sore throat occurred less during the postoperative 24 hours in the jaw thrust group compared with the control group (p = 0.007, Table 2). The incidence of moderate-to-severe sore throat was significantly lower during the postoperative 24 hours in the jaw thrust group compared with the control group (p = 0.026). The severity score for sore throat after surgery at postoperative 2 and 4 hours was comparable between the groups. The severity score for sore throat at postoperative 24 hours was significantly lower in the jaw thrust group compared with the control group (p = 0.013). Overall postoperative hoarseness was significantly lower during the postoperative 24 hours in the jaw thrust group compared with the control group (p = 0.021). The incidence of postoperative cough was similar in both groups.
Variables of postoperative airway complications.

Values are presented as the number (%) or mean (standard deviation) of patients.
CI, Confidence interval; N.S., not significant.
The incidence of overall postoperative sore throat was similar between patients who were undergoing left lateral decubitus and those undergoing right lateral decubitus (15 [33%] vs. 10 [22%], risk difference 11%, 95% confidence interval −9 to 30). The incidence of overall hoarseness was comparable between patients who were undergoing left lateral decubitus and those undergoing right lateral decubitus (10 [22%] vs. 11 [24%], risk difference 2%, 95% confidence interval −16 to 21). The incidence of overall cough was similar between patients undergoing left lateral decubitus and those undergoing right lateral decubitus (5 [11%] vs. 4 [9%], risk difference 2%, 95% confidence interval −12 to 17).
Wound pain score after surgery was similar in both the groups at postoperative 2, 4, and 24 hours (Table 3, Figure 2). The number of patients who required supplemental analgesic medication was comparable, and the requirements for diclofenac sodium, pethidine, and tramadol were not different between the two groups.
Postoperative wound pain score and analgesic requirements.
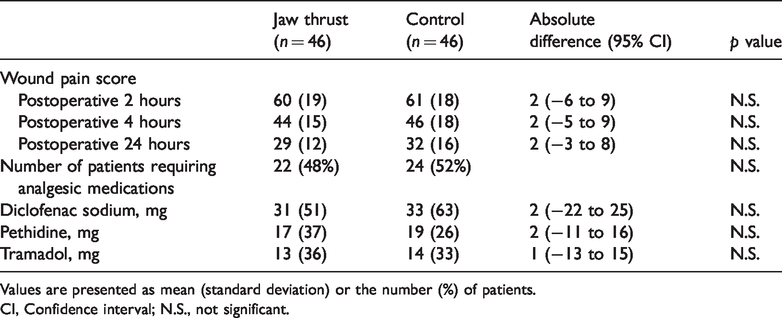
Values are presented as mean (standard deviation) or the number (%) of patients.
CI, Confidence interval; N.S., not significant.

Mean scores for wound pain score (0, no pain; 100, worst imaginable). Wound pain score after surgery was similar in both the groups at postoperative 2, 4, and 24 hours. Error bars show 95% confidence interval for the mean
Discussion
This trial demonstrated that intubation with a laryngoscope that is facilitated by a two-handed jaw thrust reduced the incidence of sore throat after surgery in patients after orthopaedic hip arthroplasty that was conducted under general anaesthesia. The jaw thrust manoeuvre also reduced the incidence of moderate-to-severe sore throat, the severity score of postoperative sore throat, and hoarseness. Jaw thrust did not result in any morbidity, such as jaw discomfort.
Sore throat is a frequent and distressing complication after general anaesthesia using tracheal intubation. 1 Postoperative sore throat may decrease a patient’s quality of life. 5 In this investigation, jaw thrust by an assistant prevented postoperative sore throat and decreased sore throat severity. Sore throat after surgery is associated with mucosal damage with inflammation that is caused by airway manipulation or the irritation that is caused by an endotracheal tube. 15 A jaw-thrust manoeuvre increases the first-time success rate and reduces the time required for tube advancement in fibreoptic oral tracheal intubation by increasing the pharyngeal cavity and laryngeal inlet size.9,13 The Cormack–Lehane grade, percentage of glottis opening, and rate of backward, upward, and rightward pressure showed no difference between the two groups, which may conflict with the decreased incidence of sore throat in the study group in this investigation. A previous report regarding double-lumen endobronchial intubation and sore throat showed fewer laryngeal injuries and a lower sore throat incidence in intubations that were facilitated by the jaw thrust manoeuvre. 11 Although the laryngeal and pharyngeal injuries were not evaluated, increased pharyngeal cavity and laryngeal inlet size that was induced by the jaw thrust manoeuvre may have decreased the physical trauma to the airway mucosa and reduced the incidence of sore throat in our study. The jaw thrust manoeuvre decreased double-lumen endobronchial tube advancement resistance during double-lumen endobronchial intubation. 11 Although double-lumen endobronchial tube advancement resistance during endotracheal intubation was not assessed, the decreased resistance by the jaw thrust manoeuvre may reduce the damage to the airway, and consequently decrease airway complications. A previous report showed that the jaw thrust manoeuvre decreased airway obstruction at the soft palate and epiglottic level. 10 Reduced obstruction may contribute to less contact between the upper airway and the endotracheal tube during intubation. Jaw thrust manipulation improves the glottis view in patients who are undergoing video laryngoscope intubation.16,17 There was a slight improvement in the percentage of the glottic opening score in the jaw thrust group, although it was not statistically significant. Glottis view improvement by jaw thrust manipulation may also contribute to the reduced incidence of sore throat in this investigation.
Various methods were studied to decrease the incidence of sore throat.6,18 Pharmacological applications using intravenous dexamethasone, 5 combined usage of dexamethasone and paracetamol, 19 and topical application of benzydamine hydrochloride 20 prevented sore throat after surgery. Physical preventive methods, compared with pharmacological interventions, have been rarely investigated. Recently, thermal softening was investigated to reduce airway mucosal injury and postoperative sore throat in patients who were undergoing double-lumen endobronchial tube insertion. 6 The jaw thrust does not cause pharmacologic sequelae. Although jaw thrust manipulation took additional time, it did not increase the time-to-intubation significantly compared with the control group in this study. In this investigation, anaesthetic induction requires one additional person who performs the jaw thrust. It may be redundant that two or more persons assist with a routine anaesthetic induction. The cost-effectiveness of intubations that are facilitated by jaw thrust manipulation needs further investigation.
Jaw thrust manipulation caused a sore jaw in patients who were undergoing face mask ventilation in a previous investigation. 21 Bruising behind the jaw after the jaw thrust manipulation was reported in a patient who was taking warfarin. 22 In our investigation, jaw thrust manipulation was applied only at intubation, which may have contributed to the similar incidence in jaw discomfort in both groups. Manipulation of the laryngoscope and the lateral decubitus position might cause jaw distress in the control group. In this study, jaw thrust reduced postoperative sore throat without additional complications.
During the postoperative 24 hours in the control group, the incidence of sore throat and hoarseness in our investigation was 44% and 39%, respectively. The incidence of airway complications including sore throat and hoarseness was relatively high compared with other investigations.23–25 The positional change in intubated patients alters the pressure and position of the endotracheal tube cuff. 26 Patients in our trial were intubated in the supine position, but they underwent a positional change to the lateral decubitus position. The previous investigations regarding sore throat in patients who were undergoing orthopaedic lower extremity surgery showed the relatively higher incidence of postoperative sore throat compared with that in previous reports.3,27 Prolonged duration of intubation is also a risk factor for postoperative sore throat. 7 These risk factors may explain the higher incidence of sore throat in this trial. The jaw thrust technique prevented postoperative sore throat in patients with a high risk of airway complications in this investigation. The jaw thrust technique that was applied during intubation, however, may not be effective in preventing sore throat in other populations.
Previous investigations using physical preventive methods did not show a decrease in the incidence of hoarseness;6,28 jaw thrust manipulation, however, reduced the incidence of hoarseness in our study. The mechanism of hoarseness prevention by jaw thrust requires further investigation. Although there was no significant difference in the Cormack–Lehane grade, the incidence of Cormack–Lehane grade III was higher in the jaw thrust group. There were not enough patients enrolled to detect the correlation between sore throat incidence and the Cormack–Lehane grade in this investigation. The effect of the jaw thrust manoeuvre in patients with a difficult airway requires further evaluation.
The protective effect of jaw thrust on the severity of sore throat was observed mainly at postoperative 24 hours, which is consistent with the previous investigation regarding double-lumen endobronchial intubation. 11 This study showed no significant decrease in severity of sore throat in the early stage—postoperative 2 and 4 hours—of the postoperative period compared with the aforementioned investigation. 11 Sore throat may be influenced by either the different types of surgical procedure or postoperative pain control in the post anaesthesia care unit. More severe pain and additional rescue analgesics administered at the immediate postoperative period in the PACU may have blunted the protective effect of jaw thrust. The duration of the protective effect of the jaw thrust manoeuvre on sore throat requires further evaluation.
The current trial has some limitations. First, endpoints including sore throat, hoarseness, cough, jaw discomfort, and postoperative pain scores are subjective. Second, practices including oropharyngeal suction and extubation may cause airway morbidity. We reduced the bias by blinding the anaesthesiologist who was performing tracheal intubations and the investigator who evaluated the endpoints. Third, although a drape was covering the patients’ jaw, the anaesthesiologist who conducted intubation might recognise the jaw thrust pressure. Hawthorne effects might have influenced the performance and the postoperative outcomes. 29 Fourth, neuraxial anaesthesia was not applied. We preferred general anaesthesia because the risk of blood loss and hypovolemia is high in patients who are undergoing hip arthroplasty. The wound pain score in the immediate postoperative period was considerable, and this could increase the incidence of sore throat. We applied randomisation to reduce this bias. Fifth, the incidence of patients with Mallampati grade 3 or 4 in this trial was relatively low and the incidence of Cormack–Lehane grade III was relatively high. The incidence of patients with Mallampati grade 3 or 4 in previous investigations ranged 0% to 14%.12,13,30 The incidence of Cormack–Lehane grade III ranged from 4% to 18%. The Cormack–Lehane grade III incidence was higher in our investigation.31,32 Although we excluded patients with Mallampati grade >2 and Cormack–Lehane grade III, the incidence was comparable in both groups, and the population in our investigation may not represent the general population. Sixth, we did not evaluate jaw discomfort using a graded scale. Jaw thrust can cause complications such as hematoma and sympathetic responses.22,33 Although the jaw discomfort incidence was comparable in the study and control groups, a graded scale would have been better to describe the jaw discomfort. Negative effects of jaw thrust in the anaesthetic induction require further evaluation. Seventh, time-to-intubation was relatively longer in this study compared with the previous studies.4,31,34 Time-to-intubation was reported as 17 to 55 seconds in the previous reports. The different anaesthetic protocols, patient population, and term definition may affect the time-to-intubation. The time-to-intubation data in this trial might not represent that of the standard population. Eighth, all intubations were performed by an experienced female anaesthesiologist. The muscle power of a female anaesthesiologist may be less than that of a male anaesthesiologist. However, a previous report 35 showed that female intubators did not differ in their ability to intubate compared with male intubators. Whether the intubator’s gender affects the incidence of sore throat requires further investigation. Ninth, BURP may influence the effect of jaw thrust and the protocol because the vector of BURP may be different from that of the jaw thrust. BURP may affect the position and size of the larynx, which may affect the airway injury and the incidence of sore throat. The incidence of BURP, however, was comparable between the groups. The effect of BURP and jaw thrust on sore throat requires further investigation.
In conclusion, jaw thrust manipulation at tracheal intubation prevented postoperative sore throat and hoarseness. Jaw thrust also reduced the severity of sore throat after surgery. Therefore, we recommend the routine use of jaw thrust manipulation during tracheal intubation.
Supplemental Material
sj-pdf-1-imr-10.1177_0300060520961237 - Supplemental material for Influence of two-handed jaw thrust during tracheal intubation on postoperative sore throat: a prospective randomised study
Supplemental material, sj-pdf-1-imr-10.1177_0300060520961237 for Influence of two-handed jaw thrust during tracheal intubation on postoperative sore throat: a prospective randomised study by Hyub Huh, Doo Yeon Go, Jang Eun Cho, Jihoon Park, Jiwon Lee and Hyun-Chang Kim in Journal of International Medical Research
Footnotes
Author contributions
Conceptualisation: Hyun-Chang Kim, Jiwon Lee, Jihoon Park; Data curation: Hyub Huh, Jang Eun Cho; Formal analysis: Hyun-Chang Kim, Hyub Huh, Doo Yeon Go, Jang Eun Cho; Funding acquisition: Hyub Huh; Investigation: Jiwon Lee, Jihoon Park; Methodology: Hyun-Chang Kim, Hyub Huh, Doo Yeon Go, Jang Eun Cho; Resources: Jiwon Lee, Jihoon Park; Software: Jihoon Park, Hyun-Chang Kim; Supervision: Hyun-Chang Kim, Hyub Huh; Validation: Hyub Huh, Doo Yeon Go, Jang Eun Cho; Visualisation: Hyun-Chang Kim; Writing—original draft: Hyun-Chang Kim, Hyub Huh; Writing—review and editing: Hyub Huh, Doo Yeon Go, Jang Eun Cho.
Declaration of conflicting interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF), which is funded by the Ministry of Science, ICT & Future Planning (2018R1C1B6007539).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.