
Abstract
Introduction
We aimed to describe the epidemiology and injury patterns of aviation sports crashes in the Austrian mountains and identify risk factors.
Methods
In this retrospective cohort study, out-of-hospital data on patients who sustained crashes when participating in aviation sports from January 1, 2006 through December 31, 2015 were assessed. The out-of-hospital data were merged with in-hospital data obtained from Innsbruck Medical University Hospital.
Results
A total of 2037 persons were involved in 1856 aviation sports crashes. Data on 126 in-hospital patients were available. Wind and pilot error were the most common causes. Most injuries occurred in paragliders (n=111, 88%). Most commonly, paragliders sustained injuries to the lumbar spine and hang gliders to the thoracic spine. Rescue operations were undertaken mainly by helicopter emergency medical services (n=87, 69%) or combined rescue forces (ground and helicopter, n=100, 79%.). The Injury Severity Score was 15±15, with a peak in patients with isolated injuries of the lower extremities (n=38, 32%) and a second peak in patients with multiple trauma (n=44, 35%).
Conclusions
In the Austrian mountains, wind and pilot errors are the most common causes of aviation crashes. Aviation sports crashes frequently resulted in severe injuries and multiple trauma. The lumbar spine is particularly at risk in paragliders, whereas the thoracic spine is commonly affected in hang gliders. Injuries frequently caused long-term paralysis and limitations in quality of life. To minimize long-term consequences and save lives, skilled and well-equipped teams may be beneficial to provide effective on-site care and safe transportation to a trauma center.
Keywords
Introduction
During the last 4 decades, aviation sports (paragliding, hang gliding, glider flight, powered fixed-wing aircraft, helicopter flight) have gained in popularity. 1 In their early days, these sports were considered extreme sports, mainly because of a lack of adequate safety precautions and safety equipment. 2 In the 1970s and 1980s, paragliding was counted as one of the most extreme sports. Critical phases of the flight such as takeoff and landing were poorly understood; they were performed by trial and error and often resulted in crashes. Safety equipment was almost nonexistent. Currently, paragliding is considered to be no more dangerous than most other sports. 1 The Swiss Accident Insurance company classifies paragliding as a regular sport, with the exception of acro-paragliding and speed gliding, which are viewed as an extreme kind of paragliding. Supporting this classification, a previous study showed that the actual risk of injury and the risk for deadly crashes in paragliding is not greater than in other aviation sports or motorcycling. 3 Aviation sports safety has improved with helmets, protective footwear, and emergency parachutes.
In Austria, 65% of the land area is mountain terrain. Mountains are attractive for aviation sports enthusiasts. However, terrain and weather can make aviation conditions unpredictable and dangerous. The Austrian Alpine police record all accidents occurring in the mountains, which are reported to medical emergency dispatch centers. There is a lack of data on aviation sports crashes in mountain regions. The aim of this study was to assess the epidemiology and injury patterns of mountain aviation crashes and to provide advice on preventive measures.
Methods
This was a retrospective cohort study. We collected data on aviation sports crashes occurring in the Austrian mountains between January 1, 2006 and December 31, 2015. A crash was enrolled in the study if it involved a paraglider, hang glider, glider, motor glider, parachute, helicopter, or any other aviation sports device (eg, speed flyer) and occurred in a mountain environment. In Austria, all emergency calls from mountain areas received by any medical dispatch center are digitally recorded by the Austrian Alpine police.
The Austrian Alpine police record out-of-hospital data (demographics, crash circumstances, injuries, and vital signs of casualties) on site and by questioning the team after the rescue mission for every emergency in which a dispatch center is notified and a professional rescue triggered. A digital accident registry for these data was started on January 1, 2006. We searched the Austrian Alpine police database for aviation sports crashes (see online Supplemental Figure 1). We matched out-of-hospital data with in-hospital data on patients treated at Innsbruck Medical University hospital (Figure 1). The patient data system of Innsbruck Medical University hospital was searched for: 1) keywords (paraglider, paragliding, paraglider and crash, hang glider, hang gliding, hang glider and crash, glider, gliding, glider and crash, aviation accident) and 2) trauma department codes for aviation crashes. We also manually scanned for patients who had experienced an aviation crash and were admitted to the emergency department or trauma department.
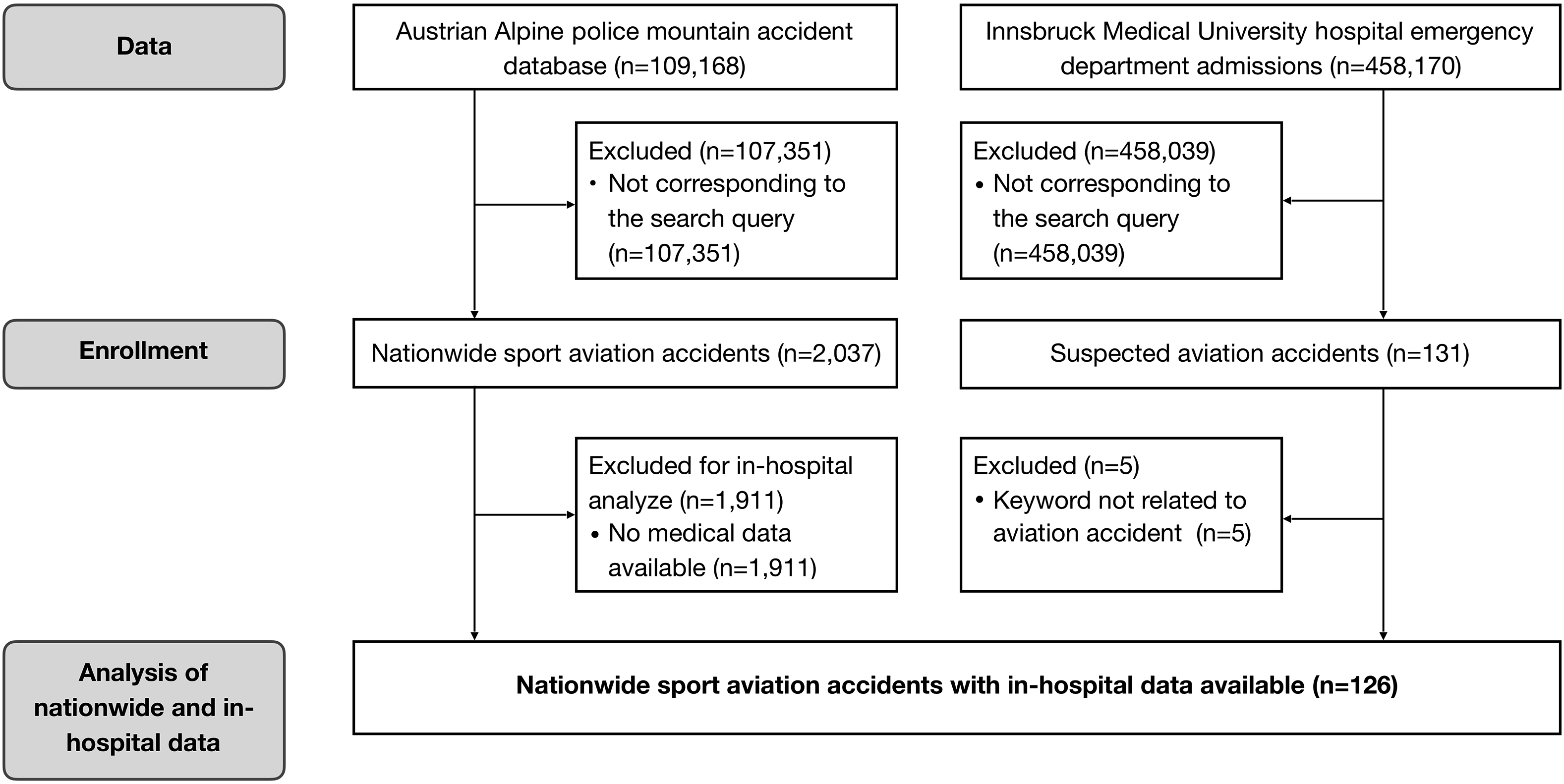
Patient inclusion algorithm with results.
Advanced trauma life support guidelines were used in patient treatment. All in-hospital patients were assessed with a full-body computed tomography scan.4,5 The abbreviated injury scale (AIS), ranging from 1 to 6, was used to calculate the Injury Severity Score (ISS). Multiple trauma was defined as ISS≥16. 6 Outcome was measured at discharge from Innsbruck Medical University hospital. The characteristics of all mountain aviation crashes in Austria were compared with the data kept by Innsbruck Medical University hospital to determine whether the Innsbruck sample was representative for Austria (Tables 1 and 2).
Demographics of patients involved in aviation sports crashes in the Austrian Alps from January 1, 2006 through December 31, 2015
ns, not significant.
Characteristics of aviation sports crashes in the Austrian Alps from January 1, 2006 to December 31, 2015
ns, not significant.
Data are presented as mean±SD or count and percentage, as appropriate. Normal distribution of sample values was checked using Shapiro-Wilk test. Differences between the national and Innsbruck groups were determined by the Kruskal-Wallis test. Differences were considered significant at a P value <0.05. Data were transcribed with Excel 2016 (Microsoft, Redmond, WA) and analyzed with SPSS Statistics 22.0 (IBM, Armonk, NY). This study was approved by the ethics committee of the Medical University of Innsbruck (AN4757 315/4.4) and registered with Clinical Trials under
Results
National Data
In 1856 aviation crashes in the Austrian Alps, 2037 persons were involved (Figure 1). The vast majority of casualties were male (Table 1). To estimate the relative risk of a female pilot experiencing a crash, we compared the number of members in the German Paragliding and Hang Glider Association (DHV) and the Austrian aviation sports organization (Austrian Aero-Club) and found a relative risk of 1.4 and 2.4 for female members. When comparing the practicing members and the crash victims, the relative risk of crashing was seen to be 1.4 higher for paragliding. Age was 41±13 y. Most victims were from Austria or Germany (86%), and 30 different nationalities were recorded. Most crashes involved paragliding and occurred during the flight phase (Table 1). Of the crashes, 57% happened in the summer months (n=266 in June, n=351 in July, n=349 in August, n=186 in September). Mean time of crash was 1400, with an SD of 158 min. Seventy-seven percent of all crashes (n=1558) occurred between 1100 and 1700. Most of the crashes occurred in sunny (n=1683, 83%) or cloudy (n=246, 12%) weather conditions. Fog, heavy rain, snowfall, strong winds, and thunderstorms were rare. Wind and pilot error were the leading causes of crashes (Table 2). Most crashes took place in the state of Tyrol (n=827, 41%), followed by Carinthia (n=331, 16%) and Salzburg (n=239, 12%). Falls from >10 m were the most common crash mechanism and occurred mostly during the flight phase, whereas crashes of <5 m occurred mainly during takeoff and landing. The altitude of the crash sites was 1250±560 m. Of the patients, 863 (42%) were rescued by helicopter. In Tyrol, 56% of the patients were rescued with a helicopter or combined rescue mission (ie, helicopter and ground forces). Injury severity was estimated on scene by the out-of-hospital emergency physician and reported to an Alpine police officer (Table 2). A subspecialty of an out-of-hospital emergency medicine exists in several European countries.
The nationwide results are comparable to those for Tyrol. Tyrolean statistics counted 266 uninjured (35%) persons, 92 minor injuries (12%), 347 major injuries (45%), 32 fatalities (4%), and 32 unknown (4%). In our results, there were no crashes caused by equipment failure. In victims who were not wearing helmets, nationwide mortality increased by up to 20%. Even in sports in which helmets are mandatory, some pilots did not wear helmets (paraglider [n=18, 1%]; hang glider [n=1]). Eighty-one (4%) crashes occurred while flying tandem; 77 were paragliders and 4 were hang gliders, with severity of injury and mortality being lower than in the overall cohort. Most patients were initially treated on-site by an out-of-hospital emergency physician from a rescue helicopter (53%). 7 The initial assessment of injuries correctly reflected the injuries later diagnosed in the hospital. In Austria, the majority of patients were rescued by helicopter emergency medical services (HEMS) (53%), and most patients at Innsbruck Medical University hospital were rescued by HEMS (79%).
Innsbruck Medical University Hospital Data
Innsbruck Medical University hospital treated 11% of all patients who needed treatment after an aviation sports crash in Austria. For 126 patients, out-of-hospital and in-hospital data were available; this accounted for 15% of all crashes reported in Tyrol. In most respects, data from Innsbruck match the nationwide results (Tables 1 and 2). Most patients were male and the age was 37±13 y. (Table 1). Most persons were Austrian or German (89%), 4 (3%) persons were from the Netherlands. Swiss, Italian, Czech, Chilean, and Danish persons were among the injured (Table 1). Most crashes (61%) occurred in summer (n=17 in June, n=22 in July, n=19 in August, n=19 in September) at 1300, with a SD of 140 min. The majority occurred in sunny conditions (n=96 of 126, 76%). Altitude of crash site was 1460±460 m. Paragliders made up by far the largest group. Fifty-one persons fell from a height of more than 10 m (n=44 paragliders, n=6 hang gliders, and 1 victim of a helicopter crash). The causes of crash were most commonly unfavorable wind conditions and pilot error. Almost all victims were wearing helmets (Table 2). Ten crashes involved 2 or 3 people. Four crashes involved tandem partners. In 79% of the crashes, rescue operations were performed by helicopter or by combined rescue (ie, helicopter and ground forces). In approximately 10% of the crashes, patients were rescued by ground forces. Many patients (41%) were severely injured. We report 4 (3%) casualties, with 3 fatal crashes occurring in sunny and 1 in cloudy conditions. In 3 cases, a pilot error was reported. In the fourth case the cause was unknown. All patients suffered multiple trauma. One patient died of a traumatic brain injury (TBI) and combined trauma of the chest, abdomen, and pelvis. The second patient died of TBI, pneumothorax, and a pelvis fracture. The third patient’s causes of death include a rupture of the pulmonary artery and hemorrhagic shock. The fourth patient experienced traumatic brain and liver injury. Three of the deceased patients had an ISS of 75. The fourth had an initial ISS of 57.
ISS was 15±15. Forty-four individuals (35%) sustained multiple trauma. 8 Two peaks in ISS were found: a lower peak in 40 (32%) less-injured patients with ISS 6 to 10, mostly owing to complex limb injuries such as ankle and lower leg fractures, and a higher peak in 21 patients (17%), who had multiple trauma and an ISS of 16 to 20 (Figure 2). The chest, abdomen, and extremities were the most commonly injured areas (Table 3). Most moderate (AIS 2) and serious (AIS 3) injuries at the level of the chest and abdomen were spinal injuries, whereas severe (AIS 4) and critical (AIS 5) injuries in those regions were mostly related to internal injuries.
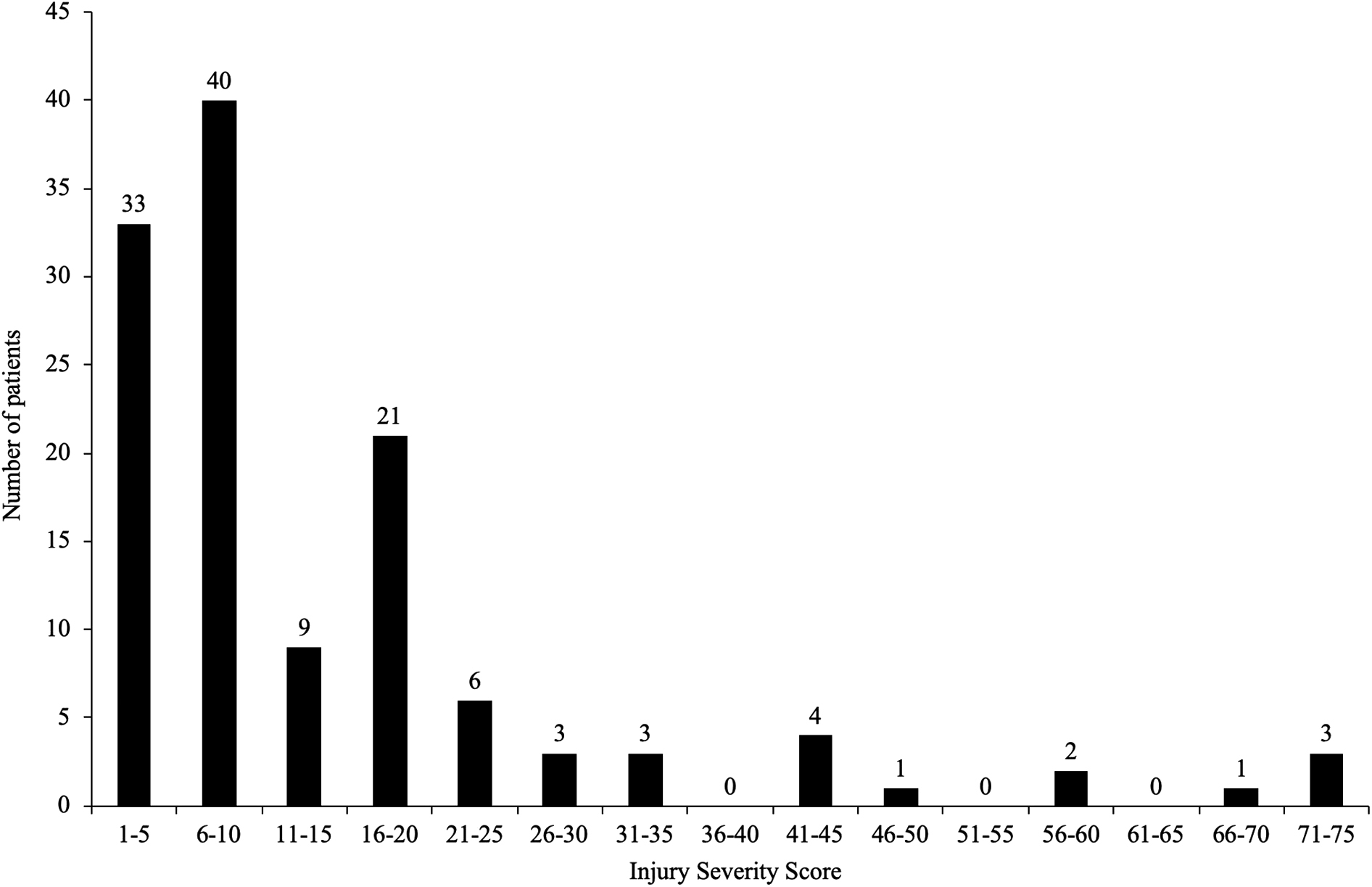
Injury Severity Scores for all patients treated at Innsbruck Medical University hospital (n=126).
AIS scoring for patients treated at Innsbruck Medical University Hospital after aviation sports crashes (n=126) from January 1, 2006 to December 31, 2015
AIS, abbreviated injury scale; ISS, Injury Severity Score; NACA, National Advisory Committee for Aeronautics.
Results are given in absolute numbers and percentages. Severity was calculated with the AIS (0 uninjured, 1 minor, 2 moderate, 3 serious, 4 severe, 5 critical, 6 maximum) for each body region to obtain ISS values. In the chest and abdomen regions, many injuries involved the spine.
Severe injuries of the face and TBI were diagnosed in 24 patients (19%). Fractures of the cervical spine were rare, found in 3 patients (2%), as compared to 31 patients with fractures of the thoracic spine (25%) and 48 patients (40%) with lumbar spine fractures. Four (13%) of the 31 thoracic spine fractures and 8 (16%) of the 50 lumbar spine fractures were associated with neurological deficits. There were 69 patients (55%) with fractures of the thoracic or lumbar spine; 12 patients (10%) had fractures of both. Paragliders commonly sustained injuries of the lumbar spine (n=46, 37%). Hang gliders commonly sustained injuries of the thoracic spine (n=4, 50%). Most spine injuries occurred in the thoraco-lumbar junction (thoracic vertebrae 11 to lumbar vertebrae 2) (47, 37%). Fractures of the pelvic ring, sacrum, and femur were present in 22 patients (18%). Two individuals experienced neurological deficits due to fractures of the pelvis. There were 58 patients (46%) who had injuries of the extremities. Twenty-four patients (19%) had upper extremity fractures. Forty crashes (32%) were associated with lower limb fractures, including knee injuries (n=7, 6%) and fractures of the ankle (n=17, 14%). The frequency of surgical and intensive care treatment is reported in Table 4.
In-hospital data on patients treated at Innsbruck Medical University Hospital after aviation sports crashes (n=126) from January 1, 2006 through December 31, 2015
ISS, Injury Severity Score; NACA, National Advisory Committee for Aeronautics Score.
Length of overall inpatient stay in hospital was 19±12 d. Typical stay in the intensive care unit (n=28) was 7±8 d. At discharge, 74 patients (59%) were in need of pain medication for continuing pain. Seventeen patients (14%) experienced paresis or paralysis ranging from lesions of the radial nerve to hemiparesis (8 lesions of peripheral nerves, 4 cauda equina syndrome, 1 hemiparesis, 1 Brown-Séquard syndrome, 1 paraplegia, 1 partial paraplegia). Five patients still experienced pain several months after the crash. Four patients had paraplegia due to complete spinal cord injury (American Spinal Injury Association ASIA A—complete injury). Sixty percent of patients were discharged home, 22 (17%) to other hospitals, and 5 (4%) directly to rehabilitation.
Discussion
Demographics and Incidence of Crashes
Generally, in mountain accidents, female pilots may be more risk averse than males. 9 Interestingly, when comparing the sex ratio of registered pilots to injured pilots, female pilots were at greater risk of crashing. In the DHV and Austrian Aero-Club, only 10% (n=3500) and 6% (n=131), respectively, of all members are female. Of all pilots involved in aviation crashes 86% (n=1757) were male and 14% (n=280) were female. If the ratio of male to female pilots is the same as the ratio of male to female members of aviation organizations, women are at greater risk of crashing relative to men. Similar to our study, in other mountain accident scenarios more males than females were injured. For instance, studies from Austria and the United States reported a high percentage of injured males in rock climbing (78%), 10 lightning strike (84%), 11 and skiing (85%). 12 The ratio of male to female athletes has not been reported in these studies.
Paragliders were by far the largest group of victims in our study, followed by hang gliders. Of 39,000 DHV members, 90% (n=35,000) were paragliders and 10% (n=4000) were hang gliders. The risk of crashing seems to be 1.4-fold higher for paragliding than for hang gliding.
Crash Circumstances
Mountains cover 65% of Austria’s surface and offer a variety of good thermal and launch conditions for paragliders and hang gliders. In Austria, the tree line is located at 1800 to 2000 m. The crash altitude was 1480 m, which is higher than most settlements; therefore, most sites were difficult to access. Direct road access was limited. We suspect that early afternoon is the most likely time for accidents because it is the optimal time for soaring thermal winds, which are attractive for takeoff and flying. Similarly, a study conducted in Tyrol in the late 1970s reported that of 75 hang glider crashes, 65% occurred between May and September and 73% between 1300 and 1500. 13 Wind and pilot error were the most important crash causes. According to a survey made by the DHV, about 50% of paragliders use thermal conditions and 20% use constant winds. Both are common during summer and daytime. Even in good weather conditions, local wind and strong gusts are risk factors in paragliding crashes. The second major cause of crashes was pilot error, which is in line with other studies performed in the United States, Germany, Switzerland, and Austria.3,14-20 In the 75 hang glider crashes, human error was responsible for more than 90%, 13 as compared to 93% for paragliders. 3 Our group did not analyze pilot experience. A study interviewing German pilots who crashed concluded that the first 2 y after obtaining a pilot’s license were the most dangerous. This could also be attributed to selection bias because it is possible that most pilots quit flying within the first 2 y after obtaining their license. The proportion of pilot error was remarkably high in experienced and very experienced pilots (n=135, 33%) and often lead to a collapse of the paraglider.14,16,21
Almost all victims wore helmets. In some aviation sports (helicopter, glider, motor glider) protective gear is not compulsory, and this might be why helmets were not worn by some victims. In our results, no crashes were caused by equipment failure. Reasons for the rare cases of tandem paragliding crashes might include 1) tandem paragliders being larger and therefore more stable and 2) pilots potentially flying more safely on commercial flights.
Rescue and out-of-hospital Assessment
Rescue missions can be challenging in mountain terrain owing to the need for technical rescue and helicopters and because of special circumstances such as cold exposure, changing weather conditions, and limited equipment. The larger proportion of HEMS missions in Tyrol may reflect the distinct mountain character of Tyrol. It might also be explained by the existence of 11 year-round and 5 additional winter HEMS bases for about 750,000 inhabitants and 5.9 million annual visitors.22,23 These numbers are much higher than for other regions of Austria. The high frequency of HEMS missions could also reflect the importance of Innsbruck Medical University hospital as a referral center for critical trauma patients in western Austria, where most of the nation’s mountain accidents (74%) happen. 24 The onsite assessment correctly reflected the injuries later diagnosed in the hospital but not necessarily the severity of injury. In contrast, other studies reported thoracic and lumbar spine injuries as commonly missed diagnoses in the out-of-hospital phase. 25
Injury Severity and Survival
All patients scored had National Advisory Committee for Aeronautics (NACA) scores ≥3. In 20 (16%) of our multiple-trauma patients, the NACA score given was 3 or 4, causing us to suspect that injury severity was underestimated by the out-of-hospital emergency physician. A study analyzed hang-gliding accidents in Tyrol from 1973 to 1976 and reported up to 80% NACA 4 and 5 patients, which was twice as high as our results. 13 Another study analyzed fatal aviation accidents in the state of Lower Saxony, Germany, from 1979 to 1996 and reported that multiple trauma was the most common cause of death (56%), followed by TBI (27%). 26 It is remarkable that in our study of all patients admitted to the trauma department, only 4 (3%) died after hospital admission. One of the 4 patients who died was transferred in hemorrhagic shock with ongoing cardiopulmonary resuscitation. The other 3 patients had multiple trauma. Two multiple-trauma patients died from TBI and 1 from respiratory failure. We suspect that the low mortality rate was because most patients died on scene before they could be transported. Thus, they were not treated at Innsbruck Medical University hospital and not registered in the local patient data management system.
In-Hospital Management
Hang glider pilots probably sustained severe head and neck trauma as a result of their horizontal head-first position. A Norwegian group reviewed several studies regarding paragliding and hang gliding. They reported that TBI and injuries to the upper extremities are more common in hang gliding, whereas injuries to the chest, abdomen, and spine are more common in paragliding. 27
The fact that most spinal injuries in our study occurred at the thoracolumbar junction is in line with prior reports.14,15,17,28 A Swiss study on aviation sports reported comparable frequencies of injuries of the spine and pelvis. 29 Ankle injuries were frequent, comparable to a Turkish study analyzing paragliders admitted to hospital and reporting 18% foot and ankle injuries. 30 In 1 study of paragliders with back injury, only 40% stated that they had landed on their legs and buttocks first. 19 Because of the seated position, the feet, pelvis, and spine are the body parts that hit the ground first and are therefore at greatest risk of being injured. Paragliders face a high risk of severe thoraco-lumbar spine injuries, including unstable fractures with and without neurological deficit.28,31,32 Thoraco-lumbar back injuries are particularly common when landing at high speed (50–100 km·h-1). 33
Advanced trauma life support guidelines were used in patient treatment. Surgery and intensive care unit admission were often required. Neurologic sequelae ranging from pain and weakness in the distribution of the radial nerve to hemiparesis, were reported. Two studies on sequelae of paragliding crashes reported that 4 out of 64 patients experienced paralysis. 15 The second study analyzed 127 accidents leading to 14 spinal lesions with persisting neurological deficit and 12 victims with chronic pain. 14 This is comparable with our results.
Limitations
This is a retrospective study, and some data are missing. Not all out-of-hospital cases could be matched to corresponding in-hospital cases. Because of restrictions imposed by the Austrian data protection authority, we assessed only in-hospital data from Innsbruck Medical University hospital, which has a Level 1 trauma center. This could result in increased rates of severely injured persons. It is known that ISS underestimates minor injuries because it considers only serious injuries. Multiple trauma is commonly defined as an ISS >15. The new Berlin criteria for defining multiple trauma might be a better option because they reflect clinical reality, enabling transparent evaluation of treatment results provided by different institutions. This is indispensable for adequate and reliable benchmarking of care and outcomes.34,35
Conclusions
In the Austrian mountains, wind and pilot errors are the most common causes of aviation crashes. Aviation sports crashes frequently resulted in severe injuries and multiple trauma. The lumbar spine is particularly at risk in paragliders, whereas the thoracic spine is commonly affected in hang gliders. Injuries frequently caused long-term paresis and limitations in quality of life. To minimize long-term consequences and save lives, a skilled and well-equipped team may be beneficial to provide effective onsite care and rapid and safe transportation to a trauma center.
Footnotes
Acknowledgements
Acknowledgments: We thank Mag. Andreas Würtele and Mag. Dagmar Walter of the Kuratorium für alpine Sicherheit (KURASI—Committee for Mountain Safety), which hosts the database of the Austrian Alpine police; Oberst Hans Ebner, BA of the Austrian Alpine police; and all contributing Alpine police officers for the provision of data and the KURASI for supporting us in this unique opportunity to analyze these cases. This study was presented as a poster at the national Anesthesia, Intensive Care and Resuscitation 2018 congress in Villach, Austria, and at the International Society of Mountain Medicine (ISMM) 2018 congress in Kathmandu, Nepal.
Author Contributions: Design of the study (MS, PP); data collection (MS, SW); analysis of the data (MS, SW); interpretation of the data (MS, SW, BW, PP); drafting of the article (MS, SW); revision of the article and contribution to the final manuscript (MS, SW, BW, MBM, HB, PP).
Financial/Material Support: None.
Disclosures: None.
Supplementary data
Supplementary material associated with this article can be found in the online version at