
Abstract
Introduction
Suspension syndrome describes a potentially life-threatening event during passive suspension on a rope. The pathophysiological mechanism is not fully understood; however, the most widespread hypothesis assumes blood pools in the lower extremities, prompting a reduction in cardiac preload and cardiac output and leading to tissue hypoperfusion, loss of consciousness, and death. The aim of this study was to assess venous pooling by ultrasound in simulated suspension syndrome using human subjects.
Methods
In this trial, 20 healthy volunteers were suspended in a sit harness for a maximum of 60 min with and without preceding exercise. Venous pooling was assessed by measuring the diameter of the superficial femoral vein (SFV) with ultrasound at baseline in supine and standing positions as well as during and after suspension.
Results
SFV diameter increased and blood flow became progressively sluggish. In 30% of the tests, near syncope occurred. However, SFV diameter did not differ between subjects with and without near syncope.
Conclusions
Free hanging in a harness leads to rapid venous pooling in the lower limbs. The most important measure to prevent suspension syndrome might be constant movement of the legs.
Introduction
Suspension syndrome (also called suspension trauma or harness hang syndrome) is a potentially life-threatening event induced by passive hanging on a rope in a vertical or near vertical position.1,2 The exact incidence of suspension syndrome is not known, but numerous case reports can be found in the literature.1,3–7 Suspension syndrome can be encountered during occupational and recreational activities in which harness systems are used (eg, work on high-rise buildings, large facades, pylons, bridges, dams, offshore platforms, and power plants; rock climbing; ice climbing; mountaineering; canyoning; and caving). 1 In 1972, the first case series of 23 climbers who were suspended in their harness systems after falls was reported. Ten of the 23 died after prolonged suspension in the harness, in spite of an absence of life-threatening trauma. 6 The pathophysiology of the suspension syndrome has been the subject of debate. The most widespread hypothesis assumes that blood pools in the lower extremities because of gravitational forces and reduced effectiveness of the muscle pump. This prompts a reduction in cardiac preload and leads to a decrease in cardiac output and critical hypoperfusion, followed by loss of consciousness and cardiac arrest. 8 However, venous pooling during suspension has never been proven. Veins of the lower extremities can easily be examined with ultrasound. However, no study has examined the effect of orthostatic stress on the venous system of the legs during suspension. In this study, we aimed to assess venous pooling by ultrasound in simulated suspension syndrome using human subjects.
Methods
We performed a study on a convenience sample of healthy male volunteers who were freely hanging on a rope using a climbing harness in an indoor climbing facility (Figure 1). Each performed the experiment on 2 different days, once with and once without climbing for 10 min before suspension (total of 40 tests). The study was approved by the institutional review board of the San Maurizio hospital of Bolzano, Italy (No. 68-2015) and registered in

Study setting: Participants were hanging freely on a rope in a sit harness. To monitor the cardiovascular response, the heart rate, blood pressure, and stroke volume were recorded continuously (Nexfin HD, BMEYE B.V, Amsterdam, Netherlands) and echocardiography was performed intermittently. To assess venous pooling, ultrasound of the superficial femoral vein was performed and tissue oxygen saturation of the calf muscle measured with near-infrared spectroscopy (O3 Regional Oximetry, Masimo Corporation, Irvine, USA). 9
Ultrasound was used to assess venous pooling. With a linear transducer (5–10 MHz, DP50; Mindray Bio-Medical Electronics Co., Ltd., Shenzhen, China), transverse and longitudinal views of the right superficial femoral vein (SFV) at the level of the mid-thigh were obtained. Diameter and blood flow were measured independently by 2 expert sonographers. Baseline measurements were obtained with the participants in a supine position and in a standing position (after 5 min of standing).
Participants then were suspended on a rope attached to a climbing harness (Rock M, Salewa, Oberalp SPA, Bolzano, Italy; appropriate size was selected according to the manufacturer’s recommendation). During the suspension phase, the ultrasound examination was repeated every 2.5 min during the first 15 min and in 5 min intervals thereafter. Intermittently, participants were asked to contract their leg muscles, and the effect of muscle contractions on venous flow was assessed with ultrasound. The suspension phase was stopped after a maximum of 60 min unless the participant wished to terminate the study earlier, the heart rate increased to over 150 beats·min-1 or decreased to less than 35 beats·min-1, systolic blood pressure increased to over 200 mm Hg or decreased to less than 90 mm Hg, the Glasgow coma scale decreased to less than 13, or symptoms of near syncope occurred (lightheadedness, pale skin, warmth, blurred vision, or nausea).
After the suspension phase, participants were brought to a supine position, and ultrasound measurements continued for 15 min in 2.5 min intervals. Increase in SFV diameter from supine to standing position and comparisons between cases with and without near syncope at 4 time points of the suspension test (start, min 5 in suspension, last measure of the suspension phase, and 5 min into the postsuspension phase) were analyzed by means of general linear models with participant as a random factor and climbing and near syncope as fixed factors. SPSS version 24.0 (IBM Corp., Armonk, NY) was used for the statistical analysis. Values are reported as mean±SD, and P<0.05 was considered statistically significant. Unless stated otherwise, values obtained in the 40 trials are reported.
Results
The study was performed with 20 healthy male participants aged 31±7 y. Near syncope occurred in 12 of 40 trials (30%) after a suspension time of 44.7±13.3 min (range 13.4 to 59.7). Seven near syncopal episodes occurred in trials with climbing before suspension with a time until near syncope of 47.0±10.5 min; 5 participants experienced near syncope in the trial without prior climbing after 41.5±17.2 min. Four participants experienced near syncope in both trials. Of the 28 trials without near syncope, 12 were interrupted after the preset maximal duration of 60 min and 16 because of pain and numbness at the lower extremities.
The mean diameter of the right SFV at different time points (baseline supine, baseline standing, beginning and end of the suspension phase, start and 5 min of the postsuspension phase) in trials with and without near syncope is reported in Table 1. A change of body position from supine to standing led to a significant (P<0.001) increase in the diameter of the SFV (from 6.4±1.6 to 9.9±1.8 mm), whereas during the suspension phase the diameter did not further increase. Once participants were positioned supine in the postsuspension phase, there was a decrease in diameter to values comparable to the baseline supine diameter. Participants with and without near syncope showed no difference in SFV diameter at start (P=0.387), min 5 (P=0.478), and last measure (P=0.414) of the suspension phase and 5 min (P=0.417) into the postsuspension phase.
Diameter (mean±SD) of the superficial femoral vein at different time points, subdivided between cases with and without near syncope
In Figure 2, the longitudinal view of the SFV of a study participant is shown, with images taken at baseline in a supine position (A) and after 2.5 (B), 5 (C), and 7.5 (D) min of suspension, respectively. In addition to the increase in diameter of the SFV, over this short time course (7.5 min), the blood flow became progressively more sluggish; at the base of the venous valve, stagnant blood is imaged. Corresponding video clips (see online Supplemental Videos 1–4), in which the difference in blood flow between the different time points can be better appreciated, can be found in the online supplement of this article. Supplemental Video Clip 5 shows how venous stasis can be resolved by muscle contraction but reoccurs very rapidly after movement is stopped.
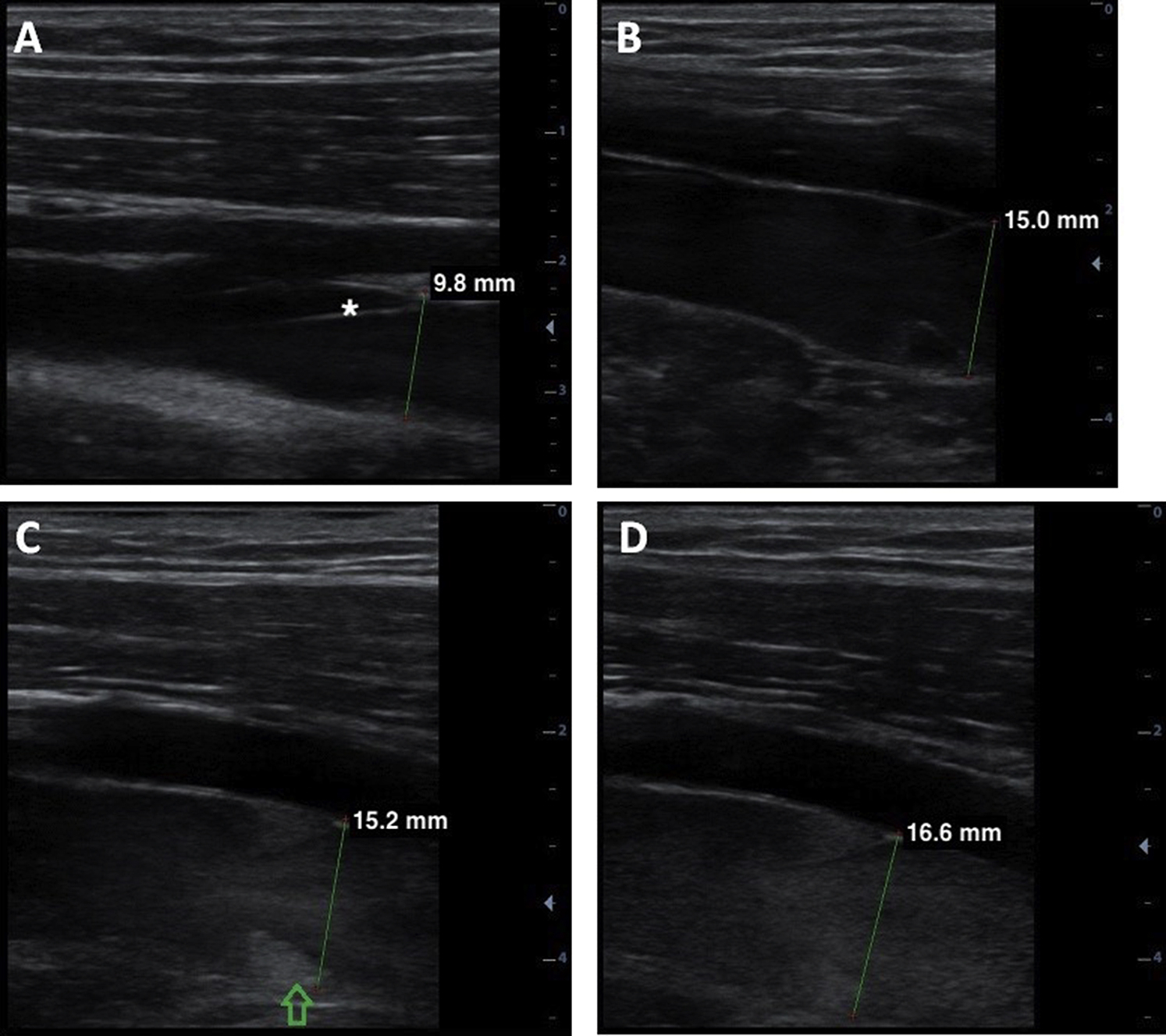
Longitudinal view of the right superficial femoral vein (SFV) with a venous valve (* in A) at the level of the mid-thigh at baseline in a supine position (A) and after 2.5 (B), 5 (C), and 7.5 (D) min of suspension is shown. The diameter of the SFV increased during the first 2.5 min of suspension (from 9.8 to 15.0 mm). From min 2.5 to min 7.5, the diameter increased much less (from 15.0 to 16.6 mm), while the blood flow became progressively sluggish. (C) The arrow marks stagnant blood flow behind the cusp of the venous valve. Anterior to the SFV, the superficial femoral artery can be seen.
Discussion
In our study, we showed a rapid orthostatic shift of blood to the lower extremities in all participants. The reason for blood pooling in the veins of the legs is likely a combination of gravitational force and a lack of muscle contraction/movement. There was an approximately 50% increase in the mean SFV diameter after the transition from a supine to a standing position. During the course of the suspension phase, the mean SFV diameter did not further increase, probably because the vessel was maximally distended. Reduced effectiveness of the muscle pump might contribute to the progressive reduction in venous flow noted during suspension. Venous compression due to the harness straps is not the likely cause of blood pooling based on anatomy: The SFV runs in the anteromedial compartment of the thigh, whereas the straps, which support the body weight, are located posteriorly. With ultrasound, we confirmed the patency of the SFV and excluded an obstructive effect of the harness straps.
Blood accumulation in the lower extremities did not differ between trials with and without near syncope. This indicates that blood pooling in the veins of the lower extremities is not the main mechanism leading to loss of consciousness in suspension syndrome. This was supported by the trends in heart rate, blood pressure, and stroke volume during the suspension phase. 9 A significant reduction in cardiac preload due to blood pooling in the lower extremities would be expected to lower stroke volume and elicit compensatory mechanisms, particularly tachycardia, to maintain cardiac output. However, in our study, there was neither a relevant decrease in stroke volume nor a compensatory increase in heart rate. The near syncopal events, observed in 30% of the trials, were characterized by a sudden decrease in heart rate and blood pressure combined with the occurrence of lightheadedness, pale skin, warmth, blurred vision, and nausea. 9 These findings resemble a neurocardiogenic event. However, the cause of neurocardiogenic syncope is unclear. Although still the subject of considerable debate, it is presently believed that the pathophysiology of neurocardiogenic syncope often is related to prolonged orthostatic stress. 10 –13 Reduced venous return is thought to activate mechanoreceptors in the left ventricle. The afferent signals from the heart to the brainstem would then override the baroreceptor responses, leading to an inappropriate decrease in sympathetic tone and an increase in parasympathetic (vagal) tone. 14 Although susceptibility to a neurocardiogenic response is probably present in all healthy persons, certain individuals appear to be more susceptible than others.15,16 This could explain why in our study only 7 of 20 participants experienced a neurocardiogenic event, although venous pooling was found in all participants.
Continuous leg movements while suspended on a rope and awaiting rescue may transiently reduce venous pooling (Video Clip 5). Continuous leg movements can be recommended as a measure to prevent blood pooling in the lower extremities and possibly to reduce or delay the occurrence of the neurocardiogenic event leading to suspension syndrome, although the clear causative link of the neurocardiogenic event has not been elucidated. However, exhaustion, injuries, hypoglycemia, hypothermia, or pain can prevent muscle activity during prolonged hanging.
Rescue death refers to cardiovascular collapse at the time of rescue. Cases of rescue death have been described in which victims were rescued from freely hanging and placed in a supine position. 17 The cause of rescue death is unclear. One hypothesis is that rescue death is due to cardiac arrhythmia. This is supported by findings of sinus arrhythmias and premature ventricular contractions noted on electrocardiogram after experimental subjects were placed in a supine position. 18 Another hypothesis assumes that there is a sudden volume overload of the right ventricle as a result of abrupt return flow of the blood accumulated in the legs when the patient is brought into a supine position. 19 Although this hypothesis has not been confirmed, it has led to a recommendation that a patient should initially be placed in a seated position so that blood can gradually return to the heart.
In our study, we found a rapid decrease in the diameter of the SFV after participants were brought into a horizontal position. However, the echocardiographic examination performed immediately afterward did not show any signs of ventricular volume overload: The left ventricular end-diastolic diameter did not even reach the dimensions measured at baseline in a supine position.
No signs of right ventricular volume overload, such as diastolic septal displacement, were found. 9 However, based on our venous ultrasound findings with marked hemostasis in the veins, rescue death could be due to pulmonary embolism (PE). In spite of its name, the SFV is a deep vein. Thrombosis of SFV is potentially life-threatening because it can embolize to the pulmonary arteries. In the literature, we found 2 cases of deep venous thrombosis in rope access workers after prolonged work in harness, in 1 case with PE. 20 Although these cases cannot be considered cases of suspension syndrome, they suggest that prolonged hanging on a rope may lead to venous stasis, which can result in venous thrombosis and PE. In the case series presented in 1972, there was no evidence for PE on autopsy. 6
Limitations
This was a simulation study. Conducting this study prospectively in a real-life environment was not feasible. During the suspension phase, participants were asked to move their legs as little as possible to facilitate the ultrasound measurements. The reduced leg movements could have influenced the degree of venous pooling. In real life, persons hanging freely on a rope would probably move their legs spontaneously, which might reduce or delay venous pooling. Exhaustion, injuries, hypoglycemia, hypothermia, pain, and so forth might preclude muscle activity.
Conclusions
Freely hanging in a harness leads to rapid venous pooling and hemostasis in the lower extremities. The most important measure to prevent venous pooling may be constant movement of the legs. By constant movement of the legs, the neurocardiogenic response might be prevented or delayed. In addition, leg movement might prevent formation of potentially lethal venous thromboembolism, which we hypothesize to be a possible cause of rescue death.
Footnotes
Acknowledgments
The authors thank the Mountain Rescue South Tyrol (Bergrettungsdienst im Alpenverein Südtirol) for use of their indoor climbing facility. Furthermore, the authors thank the companies Mindray Bio-Medical Electronics Co., Ltd., Masimo Corporation, and Salewa for the loan of equipment.
Author Contributions: Conception and design of the study (SR, PP, KS, GS, EM, HG, HB); conduct of the experiments (SR, KS, GS, EM, HB, LO, BB); data analysis (SR, KS, HG, TdC, GC); writing of the manuscript (SR, GS, PP). All authors read and approved the manuscript.
Disclosures: None.
Funding
Financial/Material Support: The study was funded by a research grant of the German Society for Mountain and Expedition Medicine (BexMed).
Supplementary materials
Supplementary material associated with this article can be found in the online version at
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.