
Abstract
Introduction
Climate change is an increasingly relevant public health issue attracting increasing amounts of attention. Despite family medicine being at the front line for public health, no recent studies have assessed the opinions of physicians and patients regarding climate change and health in the family medicine setting.
Methods
Surveys were distributed to adult patients in the waiting rooms of 4 University of Wisconsin Department of Family Medicine and Community Health clinics. Four hundred three patient surveys were collected, for an 86% response rate. An online survey was distributed to all University of Wisconsin Department of Family Medicine and Community Health physicians. Fifty-eight surveys were collected for a 32% response rate.
Results
Forty-four percent of patients believe climate change is currently affecting their community’s health. Patients have high trust in their physician regarding environmental issues (median=4 out of 5), and 6% of patients ranked their physician as a top source of information on this topic. Sixty-four percent of physicians believe climate change is affecting their patients’ health, and 17% are comfortable counseling patients about climate change and health. Although 71% of physicians believe climate change is relevant to primary care, 31% believe that physicians should have an active role in discussing climate change with patients.
Conclusions
Patients and physicians are concerned about climate change and its health implications. Patient data reveals that physicians are highly trusted but underutilized sources. However, physicians are unsure of their role in addressing this topic. Thus, a large opportunity exists for family physicians to educate patients on the emerging issue of climate change and health.
Introduction
Climate change is an emerging public health threat, with Americans becoming increasingly worried about climate change. 1 A nationwide survey in 2017 revealed 4 out of the top 10 fears of Americans are related to climate change and the environment; environmental fears had never previously entered the top 10. 2 The World Health Organization predicts there will be an additional 250,000 deaths per year between 2030 and 2050 as a result of various effects of climate change, such as heat-related disease, infectious disease, and malnutrition. 3 In addition, several recent studies have revealed unexpected associations between rising temperatures and insufficient sleep, violent crime, and chronic diseases, such as type 2 diabetes mellitus. 4 –7 Despite growing public concern about climate change and an increasing body of research on its health implications, very few studies have assessed patients’ or physicians’ opinions on the health impact of climate change. 8 –10 Although primary care is the foundation for public health, none of the studies assessing physician opinions have been conducted in the primary care setting.9,10 Furthermore, no studies have surveyed both patients and physicians within the same practice setting to compare medical and nonmedical perspectives of the impact of climate change on health.
A 1998 survey of primary care patients in Dane County, WI, revealed that patients were concerned about environmental health but did not use their physicians as sources of information, despite having a high level of trust in them. 11 This same geographic population was chosen for this study to compare environmental health perceptions nearly 20 y after this initial survey. This study primarily aims to determine patients’ and physicians’ perceived impact of climate change on patient health in the family medicine setting and has the advantage of tracking the changes in these opinions over time.
Methods
A cross-sectional survey was used for data collection. Questions for this survey were modified from the Temte and McCall study, and several questions were added and modified from 2 recent specialty-specific physician surveys. 9 –11 Each question was formatted in a dichotomous yes or no formulation, free text, or on a 5-point Likert scale, depending on the nature of the question. The protocol was evaluated as minimal risk by the University of Wisconsin Health Sciences institutional review board and received exempt status.
Patients
A 15-item paper survey was administered to a convenience sample of adult (aged ≥18 y), English-speaking patients at 4 University of Wisconsin Department of Family Medicine and Community Health (UW DFMCH) clinics in Madison, WI, and the surrounding region. Prior environmental health research has been conducted at these clinics. 11 Rural (Belleville), suburban (Verona), and urban (Wingra, Northeast) patient populations were represented at these clinical sites. All patients present in the waiting room during the days of data collection were approached by a researcher (TMB) before their appointment and given a cover letter that explained the research project, described potential risks, and provided researcher contact information. Completed surveys were returned anonymously to a collection receptacle before the patient left the clinic. The patient survey can be found in online Supplemental Materials (Figure 1).
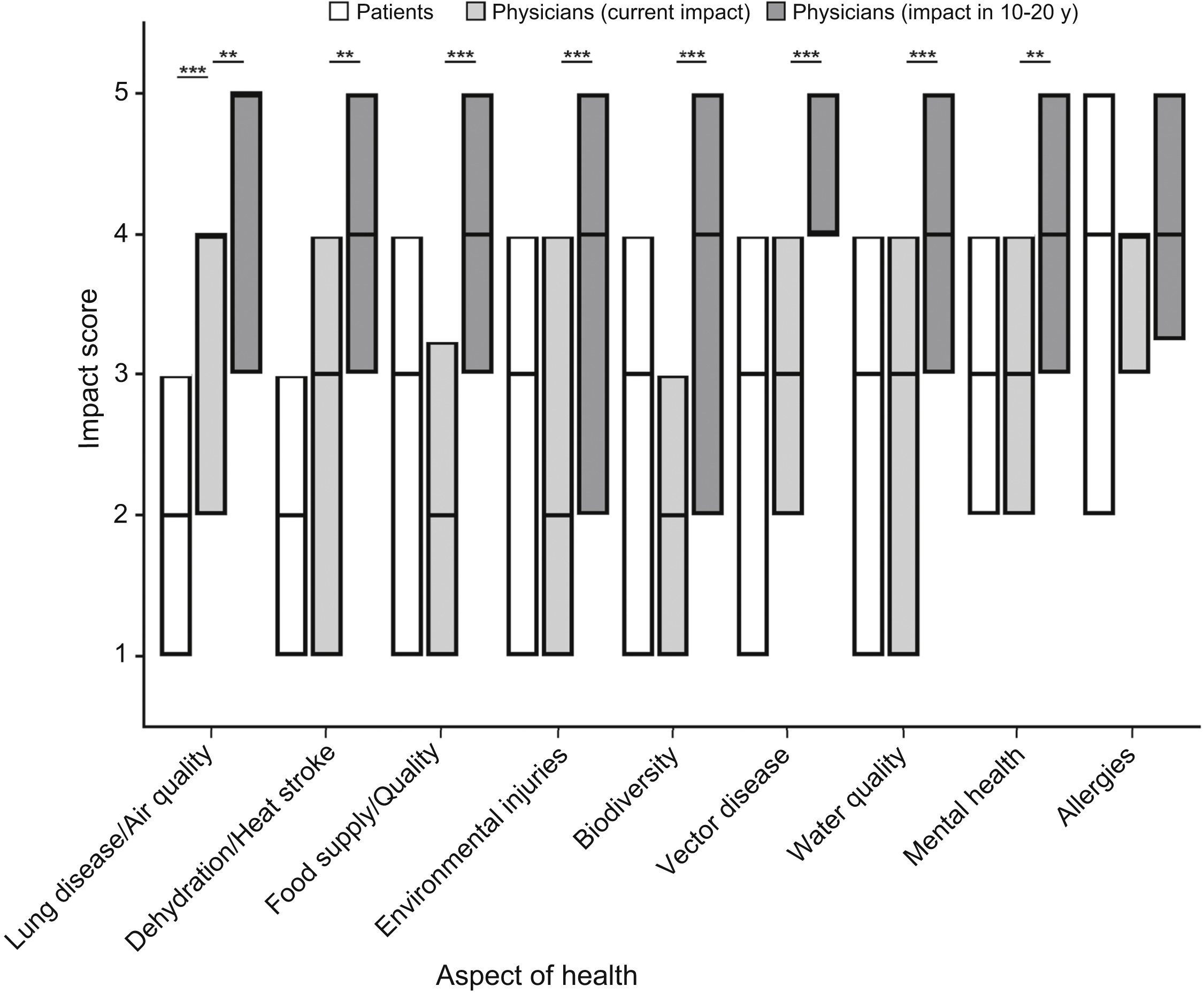
Patient and physician perception on the impact of climate change on patient health. Median level of respondents’ perceived impact of climate change on several patient health concerns was measured on a 5-point Likert scale, with 1=no impact and 5=strongly impact by climate change. Data are listed in ascending order of patient median impact level. Physician data are represented by both current impact level (light gray bar) and the predicted impact level on patients in 10 to 20 y (dark gray bar). The range of each bar represents interquartile range, with the median represented by a black horizontal line within the bar. If a median coincides with the interquartile range, the border of that bar appears larger. *P<0.05; **P<0.01; ***P<0.001.
Four survey questions addressed participant demographics. Additional questions assessed patients’ belief in the occurrence of climate change; perceived impact of climate change on their community, their community’s health, and several areas of health; top sources of environmental health information; trust in those environmental health sources; frequency of discussing environmental health topics with a physician; and how knowledgeable their family physician was about environmental health. Data collection took place May 29 through June 8, 2017.
Physicians
All faculty and resident physicians of the UW DFMCH (n=180) were included in this study, of whom approximately half work at the 4 UW DFMCH clinics involved in patient data collection. Participants received an e-mail containing an explanation of the research project and a link to a 14-item online Qualtrics survey (online Supplemental Materials; Figure 2). The e-mail was sent to nonresponders 2 additional times. Completed surveys were returned anonymously. Three questions addressed participant demographics. Additional questions assessed physicians’ belief in climate change; their perceived impact of climate change on the community, their patients’ health, and several current and future health concerns; the relevance of climate change to primary care; level of comfort and knowledge discussing climate change and health with patients; and whether primary care physicians should take an active role in this issue. Data were collected June 6 through 22, 2017.
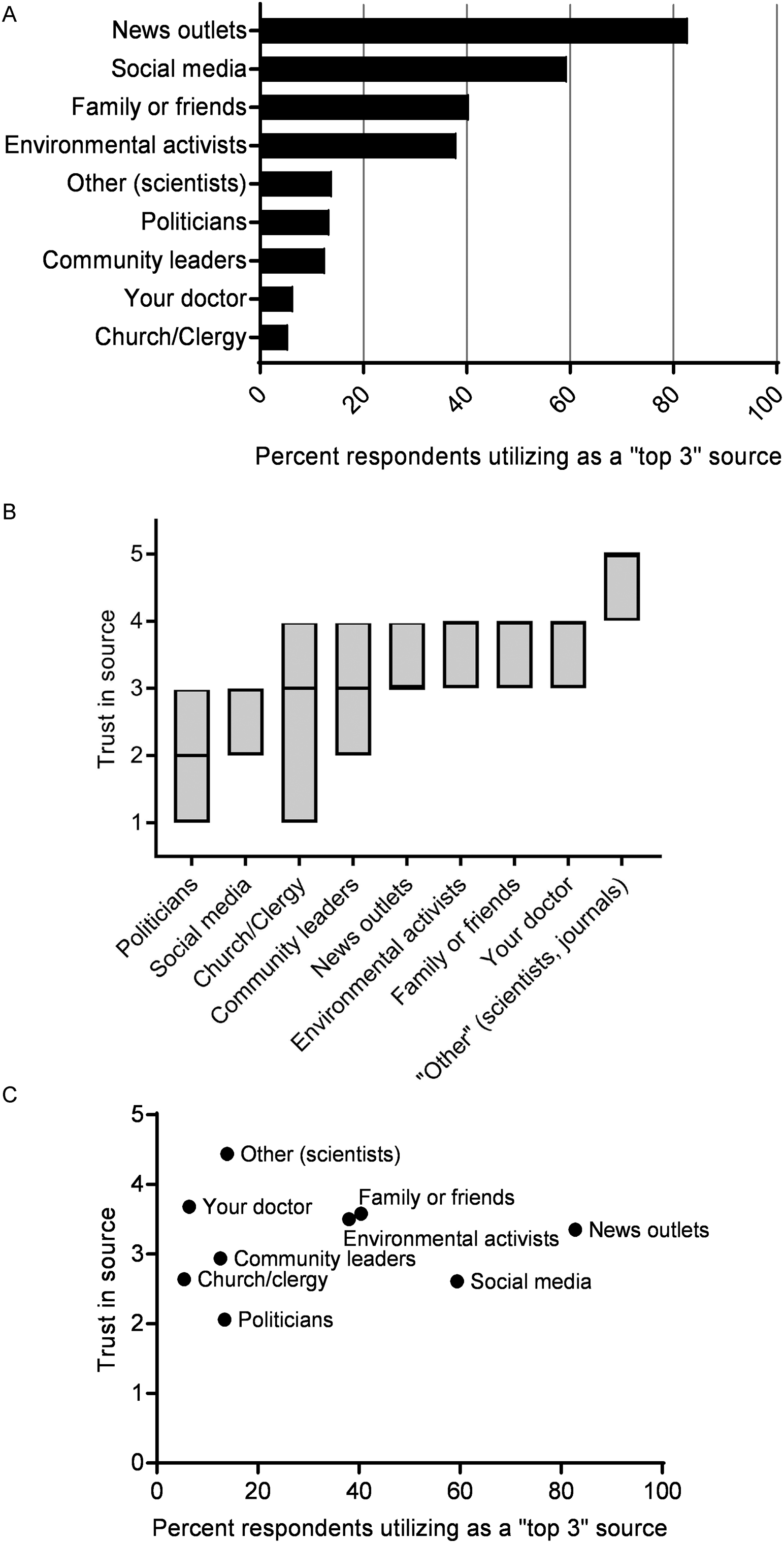
(A) Top patient sources of information. Patients reported their top 3 sources of information for environmental issues from a list of common sources. Percent utilization corresponds to the percentage of patients who listed the sources as 1 of their top 3 sources. (B) Patient level of trust. Mean patient level of trust in sources of information regarding environmental issues, with 1=no trust at all and 5=highest level of trust. The range of each bar represents interquartile range, with median represented by a horizontal black line. (C) Utilization of information source vs trust in that source.
Outcomes
Primary outcomes included patient and physician perceived impact of climate change on overall health. Secondary outcomes for patients included level of impact of climate change on several categories of health, top sources of environmental information, level of trust in those information sources, and the frequency of clinic discussions about climate change and health. Secondary outcome measures for physicians included perceived current and future impact of climate change on several categories of health, level of personal knowledge on climate change and health, level of confidence in counseling patients on this topic, and frequency of clinic discussions about climate change and health.
Data Analysis
Participants were allowed to omit answers to any question they chose. Surveys acceptable for data analysis were predefined as a minimum completion of 80% of the questions.
Descriptive statistics were used for initial analysis of patient and physician responses. Kruskal-Wallis nonparametric analysis of variance (ANOVA) and Dunn’s post hoc testing were used to compare median levels of perceived climate change impact. Parametric ANOVA with Tukey post hoc testing compared age to belief in climate change. χ2 analysis was used for comparison between discrete demographic variables. Statistical significance was defined as P<0.05. Normally distributed data are presented as mean±SD. Nonnormally distributed data are presented as median and interquartile range. Political affiliation was self-identified by choosing from 7 choices, and these data were pooled into 3 general categories for data analysis. Patients identifying as very, moderately, or slightly liberal were categorized as liberal; those identifying as moderate were categorized as moderate; and those identifying as very, moderately, or slightly conservative were categorized as conservative.
Results
Patients
Demographics
Four hundred seventy-one patients were approached, 422 (90%) patients accepted the survey, and 403 acceptable patient surveys were collected for an 86% response rate (approached-to-completed ratio). A majority of patient refusals were due to severity of illness and lack of time rather than survey content. Sixty-three percent of respondents were female, and 72% of respondents had children. There was an approximately equal distribution of responses among age groups and clinic sites. Average age was 45 y (median 46 y) with a range of 18 to 86 y (Table 1).
Patient demographics and relation to belief in climate change
Not all categories add to the total number of respondents (n=403) due to patient omission of information. Patient ages were not grouped for analysis, so analysis of variance testing was used.
Attitudes toward climate change and health, environmental information sources, and trust
Among patients, 95% believed climate change is occurring. There was an association between belief in climate change and political affiliation (Table 1), with the pooled group of self-identified liberals (n=171) more likely to believe in climate change (χ2=20.04, P<0.001; Table 1). There was also an association between sex and belief in climate change, with females more likely to believe in climate change (χ2=6.73, P=0.01; Table 1).
Fifty-seven percent of patients agreed or strongly agreed that climate change is currently affecting their community, and 44% of patients agreed or strongly agreed that climate change is currently affecting their community’s health. When asked about the impact of climate change on common health concerns associated with environmental issues, patients reported a moderate level of impact for all categories, with significant variation among some categories (Figure 1; H=127.6, P<0.001). Post hoc testing revealed that patients believed allergies were more significantly affected by climate change than any other concern (P<0.001).
Patients used news outlets (83%), social media (59%), and family and friends (40%) most frequently as top sources of information for environmental issues (Figure 2A). Doctors were a top source of information for 6% of patients. Patients reported a high level of trust in their physicians, ranking them highest among all provided choices with a median of 4 (interquartile range, 3-4; Figure 2B). The level of trust in physicians was second only to the free-text “other” category (median=5 [4–5]), with respondents (n=35) mostly noting scientists and scientific journals. Social media, one of the top sources of information, was rated lower in trust, with a median of 3 (2–3). A scatterplot comparing utilization of the source of information vs trust of that source of information demonstrated that news outlets are highly used and trustworthy, whereas physicians are trustworthy but rarely used (Figure 2C). Politicians have both low utilization and low trust.
Only 10% of patients reported speaking to their physician about an environmental issue and its health effects. Of those who had (n=40), 65% claimed their doctor was well informed or very well informed.
Physicians
Demographics
Of the 180 family medicine physicians and residents approached via e-mail, 58 completed physician surveys were collected for a 32% response rate (approached-to-completed ratio). A majority of respondents were under 50 y of age, with the 25- to 39-y age group making up the largest proportion (38%) of respondents (Table 2).
Physician demographics
Not all categories add to the total number of respondents (n=58) due to physician omission of information. Given the small cell size for political affiliation, no P value was calculated for this demographic factor.
Attitudes toward climate change and health, knowledge and comfort discussing climate change, and the role of primary care physicians
Ninety-eight percent of physicians participating in this study reported a belief that climate change is occurring (Table 2). Eighty-nine percent of these physicians reported experiencing the effects of climate change within their community, and 64% claimed they had witnessed climate change affecting their patients’ current health. Similar to patients, physicians noted that climate change was having the highest level of impact on allergies (median=4 [3–4]; Figure 1). Compared to patients’ responses, physicians reported a significantly higher impact of climate change on lung disease (P<0.001). Physicians anticipated that within 10 to 20 y, climate change will have a significantly higher level of impact in all areas except allergies (Figure 1).
One-third of surveyed physicians (33%) reported feeling very well or well informed on climate change and its health impacts (Table 3). Seventeen percent of all respondents felt extremely or somewhat comfortable counseling patients on climate change and health, and 48% admitted to being uncomfortable discussing this with patients (Table 3). Climate change was reported to be very or somewhat relevant to patient care by 71% of physicians. Less than one-third of physicians (31%) agreed or strongly agreed that physicians should have an active role in addressing climate change with their patients, and 52% neither agreed nor disagreed (Table 3).
Physician self-reported knowledge, comfort, and anticipated role regarding climate change and health
Discussion
Climate change has emerged as a popular but controversial topic. Although climate change has been discussed for decades, research supporting the impact of climate change on health has lagged behind, with most comprehensive summaries published within the last 5 y.3,8,12,13 Of those studies that have been conducted, many are observational studies noting an association between climate and disease rates. 4 –7 Few studies have assessed whether climate change is directly affecting patients in the clinical setting. This study is the first known to survey patients and physicians within the same community and shared clinic sites concurrently on climate change and health, thus allowing for a comparison between the 2 perspectives of the medical encounter. In addition, this patient population represents the same geographic population as the 1998 survey assessing patient attitudes toward environmental issues, which allows us to assess changes in attitudes during the past 19 y.
Both patients and their family medicine physicians are recognizing the current impact of climate change on health. Whereas only 17% of patients in a 2014 nationwide study reported health impacts of climate change in their household, 44% of patients in our survey reported health impacts in themselves, their family, or their community. 8 This increased level of recognition compared to other studies is even more impressive given that the patient population in this study lives in a region that is more environmentally stable than other parts of the United States. 14
Family physicians are reporting a higher current impact of climate change on health compared to patients, with nearly two-thirds of physicians affirming that climate change is affecting the health of their current patient population. This is similar to physicians in specialty surveys of thoracic physicians and allergists, where 69 and 74% agreed that climate change is affecting their patients, respectively.9,10 Similar to these specialty groups, family physicians are noting allergies and lung disease to be of highest concern.9,10 Despite this high level of concern, physicians are unsure of their role with regards to this topic. Although >70% of family physicians in this study agree that climate change is relevant to patient care, two-thirds do not think that physicians should take an active role in addressing this with patients. This is in stark contrast to specialty surveys, where 85% of thoracic physicians agreed they should have a significant advocacy role. 10 Given that family physicians are integral in addressing public health issues with patients, these data are concerning. There are several possible explanations for this discrepancy between relevance and action. Physicians admitted that most do not feel knowledgeable about how climate change affects health; similarly, four-fifths reported that they did not feel comfortable counseling patients about this topic. It is possible that this lack of education inhibits physicians from currently wanting to play an active role in this issue. Although several comprehensive reports exist, no well-accepted guidelines have been universally adopted for addressing climate change with patients, which further complicates the role of the physician.12,13 Furthermore, the nebulous and comprehensive nature of this topic may be overwhelming and daunting to discuss in a typical clinic visit. In addition, an average clinic visit lasts 17 min, and a lack of time to address climate change issues may make physicians hesitant to take on an active role. 15 It is also important to note that climate change has become a strongly politicized topic. As such, it is increasingly difficult to discuss climate change without a political connotation, which can easily be misconstrued in a medical encounter.
Patients are also concerned about climate change’s impact on health, but they are not using physicians as sources of information despite having a high level of trust in them. High trust and low utilization was also seen in the 1998 survey of this patient population, but utilization has decreased even further in this most recent survey. 11 Physicians were the second lowest used source with 6% patient utilization, barely more than church leaders or clergy. Conversely, patients in the 1998 survey reported 19% utilization of doctors. Only 10% of patients report discussing an environmental topic with their physicians, compared to 23% of patients in 1998. 11 The cause for both low utilization of physicians as environmental health resources and worsening utilization during the past 2 decades is likely multifactorial. The shortening of appointment times, the increase in the number of chronic diseases among the patient population, the increase in preventive health topics that must be covered in a single visit, and the advent of the electronic health record leaves little time for additional topics. 15 –17 Increased public access to information and scientific data may also decrease utilization of physicians as resources. Furthermore, the increased education level of patients during the past 19 y may make patients more comfortable seeking out health information through other avenues.
Overall, physicians and patients in our sample appeared to be noticing health effects of climate change but are not discussing this topic in the primary care setting. Physicians particularly did not feel knowledgeable about this topic. Therefore, a large opportunity exists for family physicians to educate themselves and subsequently their patients about how climate change can affect health on an individual and community level. This can occur through several avenues, including political advocacy, research, and direct education. An opportunity also exists to develop guidelines for the discussion of climate change and health within the clinical setting. Despite the American Academy of Pediatrics and American College of Physicians (ACP) having strong policy statements on the impact on climate change on health, little direct action has occurred to address this topic with patients.18,19 Given the time constraints on primary care clinic visits, it may not be feasible to address this topic with each patient. Thus, it would be most beneficial to primarily focus on physician education so that physicians can be cognizant of the impacts of climate change to identify appropriate patients with whom to address this topic. A comprehensive, online resource that has addressed this concern is the ACP climate change toolkit. This toolkit provides physicians with formal presentations, talking points organized by geographic region, and succinct patient education handouts to help initiate these discussions among colleagues and patients.
Several limitations exist in this study. The sample population consists of patients in Dane County, WI; this area tends to be more liberal and to have a higher education level and household income than other parts of the state or country.20,21 Only 17% of participants reported being politically conservative. Although race and ethnicity demographics were not collected in this survey, this patient population is less ethnically diverse than other parts of the nation. 21 In addition, the inclusion criteria limiting participants to English-speaking patients may have excluded a portion of the patient population with a unique perspective on this topic. Thus, selection bias exists.
Data collection was limited to 1 month, and the time of year may have introduced recall bias for certain relevant health concerns, such as allergies. We chose to poll participants from a limited number of clinics within the same health system rather than broaden our selection sample to provide a direct comparison to the prior 1998 study. 11 Although this choice does allow us to uniquely compare data and opinions across the same population over time, it limits the generalizability of our results.
It is possible that a response bias exists: Patients may have declined to participate based on disagreement with the topic. However, the response rate was relatively high (86%), and most patients who declined participation did so prior to being informed of the topic of the survey. Although the response rate for patients was high, the physician response rate was 32% and thus raises the possibility for selection bias. This response rate is typical for an online physician survey,9,10 but it is possible those who completed the survey had a higher interest in the subject matter. Although most patients declined participation prior to learning the topic of the study, physicians were sent a survey via an e-mail describing the purpose of the study prior to deciding whether to complete the survey.
It is important to note that the announcement of the United States’ withdrawal from the Paris Climate Accord on June 1, 2017, occurred during the period of patient survey distribution and may have affected survey responses due to a transient increase in awareness of the topic. Similar to all survey research, subjectivity in Likert-scale responses is unavoidable and contributes to variability in responses. In addition, there may be subjectivity in the interpretation of the term climate change because we did not provide a predetermined definition.
Conclusions
Patients and physicians appear to be concerned about climate change and its health implications, and ramifications of climate change on health will continue to grow. As highly trusted and underutilized resources, physicians are uniquely placed to educate patients and encourage public health efforts in this area. As more research is developed on specific links between climate change and health, family medicine should be at the forefront of internalizing this information, anticipating its impact, and integrating it into patient care.
Footnotes
Acknowledgements
Acknowledgments: We thank the University of Wisconsin Department of Family Medicine and Community Health for their support and amenability. Without the participation of their faculty and patients, this study would not have been possible.
This research was presented at the American Medical Association Research Symposium (Honolulu, Hawaii, November 10, 2017) and at the North American Primary Care Research Group Annual Meeting (Montreal, QC, Canada, November 18, 2017).
Author Contributions: Study concept and design (TMB, JLT); acquisition of data (TMB); analysis of data (TMB); drafting of manuscript (TMB); critical revision of manuscript (TMB, JLT); approval of final manuscript (TMB, JLT).
Financial/Material Support: None.
Disclosures: None.
Supplementary materials
Supplementary material associated with this article can be found in the online version at
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.