
Abstract
Introduction
Understanding patterns of avalanche fatalities can aid prevention and rescue strategies. In 2007, we published a report reviewing avalanche deaths in Utah between the 1989–1990 and 2005–2006 winter seasons. In the current report, we discuss Utah avalanche fatalities from the 2006–2007 to 2017–2018 seasons.
Methods
Avalanche fatality data were obtained from the Utah Avalanche Center and Utah State Office of the Medical Examiner. Autopsy reports were reviewed to determine demographic information, type of autopsy (external vs internal), injuries, and cause of death.
Results
Thirty-two avalanche deaths occurred in Utah during the study period. The mean (±SD) age of victims was 32±13 (8–54) y. Thirty victims (94%) were male and 2 (6%) were female. Seventy-two percent of deaths were from asphyxiation, 19% from trauma alone, and 9% from a combination of asphyxiation and trauma. Snowmobilers accounted for the largest percentage of avalanche fatalities (15 victims; 47%) during the 2007–2018 period.
Conclusions
Asphyxia continues to be the most prevalent killer in avalanche burial. Patterns of ongoing avalanche deaths continue to suggest that rapid recovery and techniques that prolong survival while buried may decrease fatality rates. Trauma is a significant factor in many avalanche fatalities. Education and technologies focused on reducing traumatic injuries such as improved education in techniques for avalanche risk avoidance and/or use of avalanche airbags may further decrease fatality rates. Snowmobilers represent an increasing percentage of Utah avalanche deaths and now make up the majority of victims; increased education targeting this demographic in the basics of avalanche rescue gear and avalanche rescue may also reduce fatalities.
Introduction
Avalanches pose a life-threatening risk to participants in outdoor winter activities. Understanding the causes of death in avalanche fatalities and the demographics of avalanche victims aids rescue and resuscitation strategies and may improve survival. In 2007, we published a report that reviewed avalanche deaths in Utah between the 1989–1990 and 2005–2006 winter seasons via a retrospective review of records from the Utah Avalanche Center (UAC) and Utah State Office of the Medical Examiner. 1 This study analyzes a new data set to include avalanche fatalities in Utah from the 2006–2007 to 2017–2018 seasons. Based on market trends in avalanche education and safety equipment, as well as interim publications investigating causes of death in avalanche fatalities in other areas of North America, we hypothesized that the percentage of deaths from asphyxia in avalanche burials would decline in the last decade whereas the percentage of trauma-related deaths would increase.
Methods
Avalanche fatality data were obtained from the UAC for the 2006–2007 to 2017–2018 seasons. The UAC is a federal agency within the Forest Service division of the US Department of Agriculture that conducts daily snow and climate analysis and issues daily avalanche forecasts during the winter season for the Wasatch, Uinta, and La Sal mountain ranges. The UAC investigates all avalanche accidents that occur in Utah and generates an accident report by studying how the snowpack and any human factors may have contributed to the event. The UAC is the only organization that performs this service in Utah.
Medical examiner case files and autopsy reports were reviewed to determine demographic information, type of autopsy (external vs internal), injuries, and cause of death for each avalanche fatality. An internal autopsy continued to be defined as a full examination of internal and external organs, whereas an external autopsy is defined as a visual and tactile examination of the exterior body. The medical examiner's decision to perform an external or internal autopsy was based on circumstances of death, potential legal liability, and appearance on external examination. The default is typically an internal examination. The medical examiner's stated cause of death was based on circumstances surrounding the death as well as physical evidence revealed during the autopsy. Additional information such as reports from law enforcement, search and rescue, and other witnesses were reviewed by the pathologist if necessary. Asphyxia was documented as a diagnosis of exclusion if a lethal injury was not documented on examination. Data are presented as mean±SD with range, as appropriate. A Fisher's exact test was used to calculate significance for differences in cause of death between the current study and our prior data.
The University of Utah institutional review board determined the study to be exempt.
Results
Thirty-two avalanche deaths occurred during the time period studied. The age of victims was 32±13 (8–54) y. Thirty victims (94%) were male and 2 (6%) were female. All fatalities during this period occurred during winter recreational activities. The activities undertaken by the victims at the time of each fatality are shown in Figure 1. Seventy-two percent of deaths were due to asphyxiation, 19% were due to trauma alone, and 9% were due to a combination of asphyxiation and trauma. There was no statistically significant difference in the proportion of deaths due to trauma when compared to our prior data, although the comparison approached significance (P=0.067).
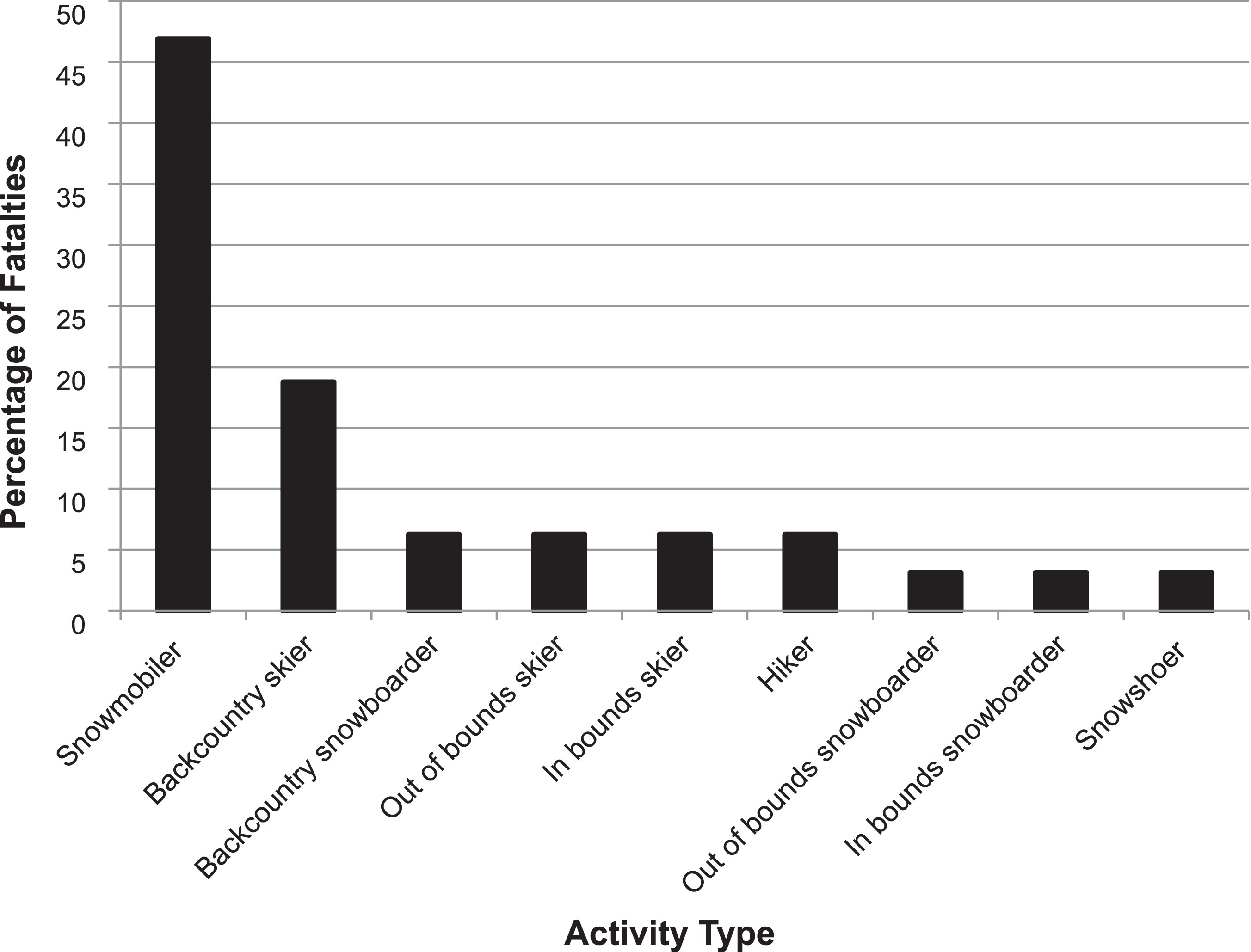
Percentage of avalanche fatalities by activity type in 2006–2018 winter seasons (n=32). Backcountry indicates remote, unpatrolled area; out of bounds, unpatrolled area immediately outside of a winter resort, accessed by a gate at the resort boundary; hiker, foot traveler.
Nearly all of the reported cases (30 of 32 deaths; 94%) received a postmortem examination. Of these examinations, 17 (57%) were internal and 13 (43%) were external.
Avalanche transceiver use was discussed in 12 pathology reports (representing 38% of fatalities). Additional data gleaned from the reports show that of those 12 cases, 6 victims (50%) were found to have a transceiver, and 6 victims (50%) were noted not to be carrying a transceiver. Of the 6 victims wearing a transceiver, 5 deaths were due to asphyxia and 1 was traumatic. Of the 6 victims not using a transceiver, 3 were snowmobilers, 1 was a hiker, 1 was an out-of-bounds skier, and 1 was a snowboarder. Airbag use was reported in 13 of the 32 cases. Of these, 3 victims (23%) were wearing an airbag and 10 (77%) were not. Of the 3 victims wearing an airbag, 2 deaths were due to asphyxia and 1 was traumatic. Rescuer cardiopulmonary resuscitation was discussed in 27 (84%) of the 32 cases; 17 victims (63%) received cardiopulmonary resuscitation in the field, and 10 (37%) did not.
Discussion
Asphyxia continues to be the most frequent killer in avalanche burial, 2 –4 although trauma remains a significant cause of avalanche deaths. As such, the majority of victims are likely to be alive during the immediate postavalanche period, and death may be prevented by timely rescue. The data we present do not allow us to definitively conclude whether devices or behaviors designed to prevent burial (eg, avalanche risk avoidance and/or use of avalanche airbags) had a significant effect on survival or ultimate cause of death. Still, the trends we have identified may suggest these interventions offer some benefit when traveling in avalanche terrain.
Rescue strategies that employ rapid recovery (eg, companion/small team rescue and/or use of avalanche transceivers) and the use of technologies that prolong survival while buried (eg, the AvaLung) are also means to improve outcome. This may be illustrated by the decreasing percentage of fatalities due to asphyxia observed in 2006–2018 (19%) compared with our original data set. 1 Multiple reports 5 have demonstrated the efficacy of avalanche airbag use in preventing burial, and avalanche airbags have become increasingly prevalent among backcountry participants. Given these trends, public educational campaigns and avalanche safety courses should emphasize that everyone traveling in or near avalanche terrain should wear and be familiar with the use of avalanche transceivers, be trained in avalanche rescue, always travel with a partner, and consider the use of an airbag.
Meanwhile, interventions to prevent death due to trauma, namely helmet use, seemed to have progressed little since 2006. Although previous research has shown wide variability in the percentage of avalanche deaths attributed to trauma, ranging from 6% to 43% of fatalities,6,7 several recent studies suggest the percentage of deaths due to trauma may be increasing. In a recent publication 8 analyzing cause of death among avalanche fatalities in Colorado, the authors found that although asphyxia was responsible for the majority of deaths, one third of observed fatalities were due to trauma. Like our study, they identified a higher proportion of avalanche fatalities due to trauma than has often been reported in prior literature. The authors do not identify a clear cause for this trend but do recognize that education and new technologies over the last 2 decades have focused specifically on prevention of burial and asphyxia and would generally not prevent traumatic fatalities. Another article published since our original data set 9 also identified higher rates of death due to trauma in other previously published avalanche fatalities. 10 Although our results do not demonstrate a statistically significant increase in trauma deaths, they suggest a similar trend.
Snowmobilers accounted for the largest percentage of avalanche fatalities (15 victims; 47%) during the 2006–2018 period, reflecting a marked increase from our initial publication. The increasing representation of snowmobilers in avalanche fatalities may reflect widening popularity of snowmobiling as a backcountry activity, as well as improvements in snowmobile technology that have facilitated access to previously inaccessible and avalanche-prone areas. Similarly to other groups, the majority of snowmobiling fatalities (14 victims; 93%) during the 2006–2018 period was secondary to asphyxia, rather than trauma from the machines. This emphasizes the potentially preventable nature of many avalanche deaths in this group as well. Educating snowmobilers on avalanche avoidance, the basics of avalanche rescue gear (a minimum of transceiver, shovel, and probe), and avalanche rescue techniques may help to reduce fatalities. In addition, education for snowmobilers regarding safe travel and practices in avalanche-prone areas would likely be beneficial in reducing deaths. The common practice of “high marking,” or purposefully riding a snow machine up a steep slope from below, presents a particularly high risk of triggering avalanche activity and should be avoided in avalanche terrain.
Finally, the majority of victims in our study were male, mirroring the results of prior studies. This may be partly due to the demographics of backcountry users and increased risk-taking behavior in male participants.
LIMITATIONS
The primary limitation of this study, as in our previous article, is its retrospective character. By the nature of medical examiner investigations, not all victims received the same type of autopsy, and not all autopsies were performed by the same examiner. Traumatic injuries could have been missed in victims receiving only an external examination. Despite these limitations, a large number of victims in this series received internal autopsies. In addition, autopsy examination is the only method of obtaining information in certain cases because many avalanche victims are not evaluated in a hospital.
Footnotes
Acknowledgments
The authors thank the staff of the Utah State Office of the Medical Examiner for their assistance with this project. Special thanks to the staff of the Utah Avalanche Center for their cooperation in assisting with historical records.
Author Contributions
Study design (SEM, GBZ, BHM, AAN); data collection (EDC, BT); manuscript preparation (SEM, GBZ, BHM, EDC, AAN, CKG, CRO, HSK, BT).
Financial/Material Support
None.
Disclosures
Dr Grissom has served as a consultant for Black Diamond Ltd, manufacturer of the AvaLung. He does not own any part of Black Diamond or the AvaLung.
Presented in abstract form at the summer meeting of the Wilderness Medical Society, August 6, 2018, Midway, UT.